Thank you for visiting nature.com. You are using a browser version with limited support for CSS. To obtain the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in Internet Explorer). In the meantime, to ensure continued support, we are displaying the site without styles and JavaScript.
- View all journals

Diseases articles from across Nature Portfolio
Diseases are abnormal conditions that have a specific set of signs and symptoms. Diseases can have an external cause, such as an infection, or an internal cause, such as autoimmune diseases.

Human SHARPIN deficiency is linked to inborn errors of cell death
We report two patients with biallelic SHARPIN deficiency, which manifests with autoinflammation and B cell immunodeficiency and is phenotypically distinct from Sharpin deficiency in mice. In one patient, there was a significant shift from pro-survival signaling to cell-death signaling in fibroblasts and lymphoblasts induced by members of the TNF cytokine superfamily, accounting for the autoinflammation and immunodeficiency. Targeted therapy with TNF inhibitors had a dramatic beneficial effect.

Sertoli cell lysosomes and late-onset hypogonadism
Zhou and colleagues explore reversing testicular aging and late-onset hypogonadism by targeting lysosomal function in Sertoli cells. The aging-related transformation of Sertoli cells into a lipid-hoarding subtype with dysregulated phagolysosomes and autolysosomes was reversed using the TRPML channel agonist ML-SA1, which demonstrates the potential of this targeted therapy in alleviating testosterone decline and systemic male-aging phenotypes.
- Ariane Zamoner
- Pedro Fontes Oliveira
- Marco G. Alves

Targeting RNA opens therapeutic avenues for Timothy syndrome
A therapeutic strategy that alters gene expression in a rare and severe neurodevelopmental condition has been tested in stem-cell-based models of the disease, and has been shown to correct genetic and cellular defects.
- Silvia Velasco
Related Subjects
- Cardiovascular diseases
- Dental diseases
- Endocrine system and metabolic diseases
- Eye diseases
- Gastrointestinal diseases
- Haematological diseases
- Immunological disorders
- Infectious diseases
- Kidney diseases
- Metabolic disorders
- Neurological disorders
- Nutrition disorders
- Oral diseases
- Psychiatric disorders
- Reproductive disorders
- Respiratory tract diseases
- Rheumatic diseases
- Skin diseases
- Urogenital diseases
Latest Research and Reviews

Perspectives on parental support of attention deficit hyperactivity disorder self-management at the transition to adulthood
This Review discusses the specific challenges and strategies in supporting individuals with ADHD during the critical transition to adulthood and outlines arguments for engaging and training parents.
- Hong N. T. Bui
- Nicholas P. Marsh
- Andrea Chronis-Tuscano

Exploring post-COVID-19 health effects and features with advanced machine learning techniques
- Muhammad Nazrul Islam
- Md Shofiqul Islam
- Iqbal H. Sarker

Molecular profiling of a bladder cancer with very high tumour mutational burden
- Manuel Scimeca
- Julia Bischof
- Pierluigi Bove

Correlates of protection against symptomatic SARS-CoV-2 in vaccinated children
The dynamics and durability of immune responses associated with protection against symptomatic infection in children offer insights to guide vaccination policies in pediatric populations.
- Youjia Zhong
- Alicia Y. H. Kang
- Eng Eong Ooi

Dopamine signaling enriched striatal gene set predicts striatal dopamine synthesis and physiological activity in vivo
Here, the authors report that schizophrenia risk variants mapping to a striatal dopamine-related gene set are associated with increased striatal dopamine synthesis capacity and increased striatal activity during reward anticipation in humans.
- Leonardo Sportelli
- Daniel P. Eisenberg
- Giulio Pergola

Extracorporeal cardiopulmonary resuscitation for patients with refractory out-of-hospital cardiac arrest: a propensity score matching, observational study
- Hong-Mo Shih
- Wei-Jun Lin
- Shao-Hua Yu
News and Comment

Life-long health consequences of undernutrition in the Yanomami indigenous population in Brazil
- Thiago dos Reis Araujo
- Ana Paula Davel
- Everardo Magalhães Carneiro

Role of the gut microbiota in the pathogenesis of IgA nephropathy
- Ellen F. Carney

Telemonitoring of patients with acute coronary syndrome
A randomized controlled trial involving a telemedicine-based approach for the management of patients with acute coronary syndrome had several clinical benefits relative to standard of care.
- Sonia Muliyil
Laparoscopic hemihepatectomy is safe and effective
- Peter Sidaway

Sex-specific nanomedicine- and biomaterials-based therapies of chronic wounds
Wound healing mechanisms differ depending on the sex, particularly in chronic wounds. Therefore, sex should be considered in the design of nanomedicine- and biomaterials-based wound healing therapies, both in preclinical and clinical testing.
- Negar Mahmoudi
- David R. Nisbet
- Morteza Mahmoudi
Quick links
- Explore articles by subject
- Guide to authors
- Editorial policies


An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- Elsevier - PMC COVID-19 Collection
Considerations for infectious disease research and practice
As the 21st century unfolds, strategies to prevent and control infectious diseases remain an area of vital interest and concern. The burden of disease, disability, and death caused by infectious diseases is felt around the world in both developed and developing nations. Moreover, the ability of infectious agents to destabilize populations, economies, and governments is strikingly apparent. To an unprecedented degree, infectious disease-related issues are high on the agendas of world leaders, philanthropists, policymakers, and the public. This enhanced focus, combined with recent scientific and technological advances, creates new opportunities and challenges for infectious disease research and practice. This paper examines these issues in the context of three countries: China, India, and the United States.
1. Introduction
Only a few decades ago, there was enormous optimism that the threat of infectious diseases was receding. Scientific and technologic advances, such as the development of antibiotics and vaccines, along with improved hygiene, sanitation, and vector control, enabled dramatic improvements in health and led many to predict the end of infectious disease [1] . This was especially true in the industrialized world, but even the poorest nations showed encouraging signs of victory in the battle against infectious disease.
Nonetheless, we know today that such optimism was premature. It did not take into account critical factors such as the extraordinary increase in international travel and trade, and the movement of people into urban settings—many into mega-cities—where the spread of disease is amplified through crowding, poor sanitation, and inadequate hygiene. It also did not recognize that changing agricultural practices and environmental manipulations would dramatically alter disease vectors and opportunities for exposure. That early optimism did not reflect the continuing challenge of how to change behaviors that increase transmission and exposure, including risky sexual practices and intravenous drug use. In addition, it underestimated the extraordinary resilience and ability of microbes to change and adapt, and the continuing difficulty of ensuring that existing medical knowledge and tools translate into real-world care for anyone who needs it, whether because of inadequate resources, ignorance, or complacency. Sadly, it is now apparent that we also live in an era when we must prepare for the possibility of microbial agents being used intentionally as weapons to do harm [2] .
2. The burden of infectious disease
In our modern world, infectious diseases still claim millions of lives every year. Globally, infectious disease represents the second leading cause of death, and the leading cause of death for children and adults under the age of 50. Infectious diseases place a particularly severe burden on the less-developed parts of the world, causing one in every two deaths. Overall, infectious diseases account for about 30% of healthy years lost to illness, as measured by disability-adjusted life years (DALYs) [3] .
2.1. Emerging and re-emerging infections
Within just the last few decades, more than 30 newly discovered infectious disease threats [4] have emerged. The majority of these have been zoonoses, or human diseases that have their origins in animal disease. HIV, severe acute respiratory syndrome (SARS), H5N1 avian influenza, Ebola, and Nipah virus are a few such examples [5] . We have also witnessed the re-emergence or resurgence of old diseases like West Nile disease, monkeypox, dengue fever, malaria, and TB, often in new geographic regions. In some cases, the resurgence of diseases like malaria and TB has come in new and more dangerous forms that are drug-resistant, which is becoming a serious problem worldwide. Unfortunately, the widespread and often inappropriate use of antimicrobials has led to the emergence of resistant strains of many microbes, complicating the management of a wide variety of diseases, and threatening future treatment options [2] .
Virtually all nations have been affected by these emerging and re-emerging infectious diseases. In addition, prospects for more emerging diseases will likely increase in coming years due to continuing globalization of trade and travel, urbanization and crowding, inadequate health care, and encroachment on the environment—all leading to new interactions between people and animals and other vectors of disease. While the scope of the problem is vast, the encouraging fact is that we have an opportunity to make enormous improvements in health through new understandings of the threats we face and appropriate applications of scientific and technological advances.
2.2. Infectious component of chronic diseases
It is important to recognize that there can be a substantial infectious component to chronic disease. In fact, many chronic conditions once thought unrelated to infectious disease are now linked to bacterial, viral, or parasitic agents. This is an area of active exploration and research, and many fascinating examples are emerging in the realm of cancer, cardiovascular disease, neurological disease, ulcers, diabetes, and others, with far-reaching implications for health.
Recent research indicates that viruses are a causal factor in 15–20% of all human cancers [1] . For example, human papilloma virus causes almost all cases of cervical cancer, a major killer of women worldwide. Liver cancer is the third leading cause of cancer death in the world, and hepatitis B and C account for about 80% of all liver cancers. In many of these cases, viral genes are necessary for the initial development of the tumor as well as for the continuing survival of tumor cells in the final malignant stage. This suggests there may be opportunities to prevent or possibly cure certain cancers through control of either the initial viral infection or through the inhibition of viral functions [6] . In fact, the use of hepatitis B vaccine has already resulted in a decreased incidence of liver cancer in certain populations [1] .
2.3. Infectious disease in the US, China, and India
No nation is immune to the complex challenges of infectious disease. In more developed countries such as the United States, but also in China and India, the burden of infectious disease is less pronounced but still severe. The US has demonstrated the greatest progress in the struggle against infectious disease, with a 10-fold decrease in the number of infectious disease deaths over the first half of the twentieth century, thanks to improvements in sanitation, hygiene, and the introduction of antibiotics and vaccines. In the following decades, there were continuing improvements—although less dramatic—until the 1980s, when infectious disease rates actually began to increase because of emerging and re-emerging infectious diseases, including HIV/AIDS. However, even when deaths from HIV/AIDS are excluded, there is still a general upward trend in the number of deaths from infectious disease [2] .
Both China and India have made enormous strides in improving the health and curbing the spread of infectious diseases, reflecting the remarkable economic progress of these two nations [7] . However, people in these countries remain at a higher risk of developing infectious diseases and dying from their illness than people in the US, largely due to poor sanitation, unhygienic living conditions, and inadequate access to quality healthcare.
India suffers the greater burden of infectious disease. India is estimated to have the second highest number of HIV/AIDS cases in the world (second only to South Africa), with over 4.58 million infected people. Half a million people are projected to die from AIDS in India next year, and 600,000 are in urgent need of antiretroviral therapy [8] . Tuberculosis, including multi-drug resistant-tuberculosis (MDR-TB), also represents a major challenge for India. Cholera and dengue fever have been longstanding health problems in India; however, outbreaks of both of these diseases have increased significantly of late. Acute respiratory infections, diarrhea, and neonatal infections remain major childhood killers, despite significant improvements in immunization rates in recent years [8] .
China is better off than most of the countries to its south. The toll of many infectious diseases, including sexually transmitted disease, malaria, schistosomiasis, and vaccine-preventable diseases, was substantially reduced over past decades, although recent reports from China indicate continuing problems with increasing trends for some areas [9] , [10] . The most prevalent disease is tuberculosis, followed by hepatitis B, dysentery, syphilis, and gonorrhea. According to official reports, these five diseases account for almost 88% of all reported cases [11] . Although overall prevalence remains relatively low, HIV/AIDS is fast becoming a major problem. As of the end of 2005, the Chinese Ministry of Health estimated that 650,000 people in China were infected, with an estimated 70,000 new HIV infections and 25,000 deaths that year [12] . The joint United Nations Program on HIV/AIDS (UNAIDS) predicted that by 2010 over 10 million people could become infected, and it termed this HIV epidemic as “China's titanic peril” [13] .
China is highly vulnerable to other emerging infectious diseases as well. Animal husbandry practices in China have led to close contacts between animal and human populations. In fact, China has more people, pigs, and poultry (1.3 billion, 508 million, and 13 billion, respectively) living in close proximity to people than any nation in the world—or in history [14] . With high levels of avian flu circulating within the country, China is now dangerously positioned to become the source of a new pandemic flu. Such conditions also raise significant concerns about the emergence of another serious zoonotic disease like the SARS outbreak, which began in China.
3. The widening context of infectious disease threats
Addressing the problems of serious endemic infectious disease is a fundamental and urgent requirement. However, the increasingly transnational nature of emerging infectious diseases constitutes one of the greatest challenges of our modern era. In today's highly interconnected world, a disease that occurs in one part of the world can travel around the globe in less than 24 hours. In recent years, avian flu, SARS, and HIV/AIDS have received prominent coverage, but they are only three on a list of infectious diseases that require a global response.
Moreover, outbreaks of these diseases have the potential to cause profound economic damage, as well as social and political instability. India learned this lesson in 1994 when there was an outbreak of pneumonic plague in Surat. The national and international response led to the closure of airports and dramatic disruptions in tourism and trade, at an estimated cost to India of approximately $1.7 billion [15] . More recently, this lesson was brought home to China when SARS emerged in Guangdong Province in 2003 and spread rapidly throughout China and around the globe. Health authorities were unprepared, and serious deficiencies were revealed in China's ability to mount an effective, coordinated response. Early on, official efforts to conceal the extent of the emerging epidemic exacerbated the situation and critical time for disease identification and containment was lost. The consequences were devastating for China and the world; more than 8000 people were infected and some 800 died; cities were paralyzed for months; travel was disrupted; and the direct economic impact on other countries in the region was estimated to be as high as $30 billion [8] . China was forced to reassess its ability to control communicable disease, and to make new commitments to strengthen its systems for infectious disease control.
4. Critical role of infectious disease research
As new attention and concern is directed to the challenges of global health and infectious disease, extraordinary advances in life sciences research and biotechnology have already begun to drive a global transformation in the design, development, and delivery of new tools to combat infectious diseases. In addition to basic research into how infectious organisms cause disease, and how the human immune system responds—both of which will enable new understanding into the nature of disease and how to address it—new opportunities have appeared. These include rapid and effective strategies for early detection of microbes, antibiotic sensitivity profiles, targeted efforts to improve drugs and therapeutics to manage or cure infectious disease, new and improved vaccines for prevention and control of disease, and new systems to more efficiently deliver therapeutic and preventive interventions. Other technology advances with important implications for infectious disease and public health include enhanced systems for disease surveillance and early recognition, as well as opportunities to more meaningfully analyze and model disease outbreaks and develop strategies for their control.
The emergence and rapid expansion of fields such as recombinant biology, genomics and proteomics, systems biology, synthetic biology, information technology (including computer and mathematical modeling), genetic epidemiology, and nanotechnology underlie much of these new understandings, capabilities, and opportunities [16] . For example, the application of functional genomics and proteomics enables a deeper understanding of the etiology of disease and its manifestations. Synthetic biology offers important new strategies for drug discovery and design. Work at the intersection of these fields and cross-disciplinary approaches are increasingly critical. For example, because many important pathogens persist in animal reservoirs or may be transmitted to human hosts through other vectors, examination of important aspects of infectious disease transmission in these systems, including animal and human host resistance and susceptibility, vector efficiency, genetic variabilities, and population dynamics, will be essential.
At the same time that advances in science offer new tools to analyze information and better understand disease, they also offer opportunities to greatly enhance the speed of progress. For example, continuing technology advances in DNA sequencing will make it possible to rapidly characterize more and more genomes, offering greater insights into basic composition and individual variation in both human and pathogen populations. The ability of genomics to support the development of increasingly rapid and reliable assessment tools like microarrays will be a huge asset to the swift diagnosis of infectious disease agents. Applications from the fields of robotics and informatics will facilitate rapid, high-throughput screening for new potential antimicrobial drug candidates. Information technology will enable large quantities of data to be rapidly mined, with a goal of more effective disease identification or trend tracking in real time that enables swift response.
Continuing advances in technology will make a range of important tools, techniques, and assays increasingly accessible to those with less training and expertise, which will greatly broaden their utility and impact. However, as these advances move forward, parallel efforts must be undertaken to reduce costs. Cost remains a major barrier to effective application of these tools, whether for research, for clinical care, or for public health disease control interventions. Correspondingly, the link between infectious disease research, and health care needs, services, and training must be strengthened in order to ensure that the appropriate research agenda is addressed and implemented. Moreover, without a commitment to some minimal level of infrastructure for healthcare, the benefits of scientific advances will not translate into meaningful care for those in need.
5. The changing context of life sciences research
The field of infectious disease is being transformed by advances in new fields of science. While US scientific research in the life sciences and biotechnology sectors still leads the world, the US no longer stands alone in its levels of research productivity or research funding [16] , [17] . Both China and India are becoming major players, which has important implications for the conduct and content of infectious disease research and practice.
With booming economies and new spending power, both India and China see enormous opportunities to invest in key areas of emerging scientific activity, such as genomics and proteomics, information technology, and nanotechnology, and are placing an increasing premium on innovation in their scientific enterprise [18] , [19] . Clearly, advances in these fields are vital for addressing some of the most pressing disease challenges in those countries and beyond, but investment is also seen as a critical component of their national economic development strategy.
One indicator of the growing role of China and India can be seen in the reversal of the “brain drain.” With considerable new investments to strengthen educational institutions, research facilities, and research funding, growing numbers of talented Indian and Chinese scientists are choosing to stay in their home country to undertake scientific training and careers. In addition, the number of Western scientists seeking research opportunities in Chinese and Indian institutions is on the rise. Many foreign companies, including large multinationals, are deciding to establish sites or launch ventures in China and India because of the large and relatively inexpensive talent pool and the lower costs of doing business [16] .
While China and India are well positioned to become powerful players in the infectious disease arena, rapid expansion of their life sciences research and the associated pressures to produce economy-boosting science have led to concerns about quality control, ethics, and the adequacy of research and production oversight [20] . Continued success and the ability to compete at the global level will require sustained investment to strengthen and extend the scientific research infrastructure in these countries, including improving the quality of higher education, regulatory oversight, adherence to ethical and biosecurity regulations, and open, transparent collaboration.
It is in all our best interests to strengthen the cooperative nature of these scientific endeavors. Enchancing scientific links and forging far-reaching scientific collaborations will have many benefits. For one thing, a large share of the serious infectious disease problems of global concern currently exist or are likely to emerge from regions that include China and India. Research and development in those areas has special value because it is generally easier and more economical to study diseases where they are endemic. With respect to public health, such collaboration becomes imperative because of the transnational consequences of many of those infectious diseases. Fundamental knowledge about the nature of certain organisms and the diseases they cause, as well as opportunities for early detection, response, and control, can most effectively be achieved through broad-based collaboration. Such collaboration builds confidence and transparency and promotes sharing of data in a timely manner. This will strengthen the science base and opportunities for discovery, and amplify resources for meaningful action. Open scientific collaboration among these nations will also help to support quality research of the highest scientific and ethical standards.
6. Potential for misapplication
In an era of terrorism, such collaboration takes on additional importance. It is evident that growth in biotechnology and the explosion of knowledge about the fundamental building blocks of life—and how to manipulate them—bring with it staggering and unpredictable power. While advances in modern biology offer great hope to improve health and prevent disease, they also offer tools that can be used—through malevolence, misapplication, or sheer inadvertence—to create new and more dangerous organisms, and effective mechanisms for delivery. From a scientific perspective, managing this threat is a complex challenge. No one wants to impede the progress of legitimate and important science. However, we must recognize a set of real concerns. Meaningful solutions will require the full engagement and support of the scientific community, as well as a mix of strategies that include professional standards and codes of conduct, national rules and regulations, international guidelines and agreements, and a fundamental shift in understanding and accountability about how science is done.
The potential threat of bioterrorism is felt most profoundly in the US, where the anthrax attacks in 2001 heightened attention and concern. In recent years, new initiatives have been undertaken to examine the implications of advances in life sciences research and biotechnology, and the government has tightened its ability to monitor the procurement and use of dangerous pathogens [16] . Other countries have indicated concern about this threat as well. For example, the Chinese government and its scientific leaders have developed codes of conduct and other regulations to address biosecurity and reduce the risk of bioterrorism [21] . India has also begun to address this threat through policy and programs now underway [22] . Many cross-national initiatives have also been undertaken to engage these and other nations, and to develop a scientific awareness and ethos to foster adequate and appropriate oversight of biosecurity, including the responsible stewardship of research activities, knowledge, and materials. International cooperation will be essential to achieving these goals.
7. Conclusion
Looking to the future, all nations share a common need to meet the challenge of more effectively detecting, tracking, treating, and preventing infectious diseases. The scientific research community must respond by identifying critical needs and developing strategies to address them. These challenges will require the integration of cutting-edge science and technology with a complex array of social, political, legal, ethical, and economic realities. Moreover, it will require new partnerships across nations, and a more effective coordination of public- and private-sector efforts. And throughout, it will require a delicate balancing act between competing priorities, including: global health needs; personal, national, and international security; the role of the research enterprise and industry on the economy of a growing number of countries; and support for the advancement of science and its safe application.
Margaret A. Hamburg, M.D., is Senior Scientist at the Global Health and Security Initiative, Nuclear Threat Initiative (NTI), and an expert in public health, infectious diseases, and emergency preparedness. She was founding Vice President for Biological Threats at NTI and helped to create their Global Health and Security Initiative. Prior to this, Dr. Hamburg held the positions of: Assistant Secretary for Planning and Evaluation, US Department of Health and Human Services; New York City Commissioner of Health; and Assistant Director of the National Institute of Allergy and Infectious Diseases, NIH. A graduate of Harvard College and Harvard Medical School, Dr. Hamburg serves on numerous boards and committees. She is a member of the Institute of Medicine/NAS, the Council on Foreign Relations, and American Association for the Advancement of Science.
Skip to content
Meet Our Faculty
Meet our expert faculty in the Division of Infectious Diseases in the Department of Medicine.
Infectious Diseases Fellowship Program
Apply to our fellowship.
Find out how to apply for the Infectious Diseases Fellowship Program at CUIMC.
View Our Labs
Explore our labs and discover cutting-edge research in the Divison of Infectious Diseases.
Patient Care
- Make a Gift
Research Projects
Staphylococcus aureus.
The past decade has witnessed a dramatic increase in Staphylococcus aureus infections acquired from the community. Yet there remains a limited understanding of how these strains spread and subsequently become established and persist within communities. Our research is focused on identifying molecular mechanisms that allow epidemic S. aureus strains such as USA300 to successfully disseminate. This project uses a combined approach of whole-genome comparative sequencing of longitudinally collected samples, genetic manipulation, and functional studies on bacterial adhesion and survival. These molecular studies are informed by ongoing epidemiological studies on S. aureus transmission in the local community. This work has identified a potentially newly emerging S. aureus strain, ST398, which was previously only associated with close contacts to animals. Ongoing studies are aimed at elucidating the molecular mechanisms of its cross-species transfer and current animal-independent spread.
Klebsiella Pneumoniae Infections in Transplant Patients
Infections with carbapenem-resistant Enterobacteriaceae (CRE) have emerged as an urgent threat to healthcare, the “category of highest concern” in the 2013 CDC antimicrobial threat report. These multi-drug resistant infections are associated with high mortality. Recipients of solid organ transplantation, in particular liver transplant recipients are at increased risk for CRE infections. While intestinal colonization with CREs has been proposed as a potential risk factor for infections during CRE outbreaks, its actual contribution to infection remains incompletely understood. Moreover, there is a fundamental gap in knowledge on how these antibiotic resistant organisms transition from colonization to infection within affected hosts. We have established a cohort study of patients undergoing liver transplantation in which we aim to investigate the contribution of colonization to subsequent CRE infection. The long-term goal of this project is to elucidate at the bacterial genome level how CRE infections emerge and spread. Understanding these processes is critical to developing intervention and real-time clinical monitoring approaches to limit the impact of CRE infections at an individual and population level.
Microbiome in Infectious Diseases
During intestinal colonization, microorganisms closely interact with their surrounding bacterial communities and the immune system. Even single doses of antibiotics can profoundly affect the composition of the gut microbiota. The effects of organ transplantation on the microbiome are multifaceted, including the underlying disease, immunosuppressants, perioperative antibiotics, and the surgery itself. We are investigating how the intestinal microbiome modulates colonization with multi-drug resistant organisms in liver transplant recipients. Additional studies focus on the interaction of the intestinal and oral gut microbiome with the immune system in persons living with HIV.
Division of Infectious Diseases section navigation
Infectious diseases research.
The Division of Infectious Diseases engages in a broad spectrum of basic, clinical, translational, and epidemiologic sciences. The division garners more than $30 million in research funding per year.

Infectious Diseases faculty collaborate actively with other top-rated local and regional programs, including the Emory Vaccine Center , the Emory Department of Microbiology and Immunology , the Emory Rollins School of Public Health , and the Centers for Disease Control and Prevention (CDC) , in addition to numerous centers in the United States and abroad.
You can view ongoing trials in Infectious Diseases by visiting Emory Clinical Trials .
Research Programs
- Antibiotic Resistance Center
- Center for AIDS Research
- Kwazulu-Natal Drug Resistance Surveillance Study
- Emerging Infections Program
- Emory Clinical Trials Unit
- Emory T32 Training Program in Translational Research to End the HIV Epidemic
- Hope Clinic - Vaccine Research
- Prevention Epicenter of Emory and Collaborating Healthcare Facilities (PEACH)
- Ponce Clinical Research Site
- Infectious Diseases Clinical Research Collaborative
- Integrating HIV and heart health in South Africa (iHEART-SA) project
- Research in HIV and Women's Health and Y This Harmony Matters (RHYTHM)
Basic Science Research Opportunities
Basic scientific research within the Division of Infectious Diseases focuses on:
- Mechanisms and control of antibiotic resistance
- Treatment of hospital-acquired infections, such as Clostridium difficile ( C. difficile )
- Pathogenesis of infectious diseases, such as bacterial meningitis
- Basic and translational research in HIV
- Immunology of host defenses and vaccine development
Major areas of investigation of bacterial pathogens include:
- Analysis of virulence mechanisms of invasive bacterial pathogens
- The role of endogenous bacterial CRISPR/Cas9 systems in host immune evasion and targeted DNA editing
- Genomics of bacterial virulence and antibiotic resistance; study of the microbiome
- Studies of the molecular mechanisms of antibiotic resistance
- Research into the role of transposable elements and repetitive nucleotide sequences in microbial pathogenesis and agents associated with bioterrorism
- Metagenomics of pathogens for basic and clinical research
The Division of Infectious Diseases participates in graduate programs and research in microbiology and molecular genetics, immunology and molecular pathogenesis, as well as population biology, ecology, and evolution.
Additional opportunities are available for basic science research in:
- Toxin-mediated infections
- Intracellular pathogens
- Hemorrhagic fever viruses
- Zoonotic pathogens
- Parasites and fungi
- Population biology
- Genomics and metagenomics
Emory Vaccine Center and Emory Hope Clinic
The Emory Vaccine Center receives more than $24 million in sponsored research funding. Primary program areas in basic science and translational research currently include HIV/AIDS, tuberculosis, malaria, Hepatitis C virus (HCV), cytomegalovirus, gamma-herpes viruses, influenza and DNA and protein-conjugate vaccines.
The Hope Clinic , a unit of the Emory Vaccine Center directed by Mark Mulligan, MD, conducts clinical research, vaccine trials and critical research on vaccine policies. A number of additional opportunities for basic scientific research are available in the Graduate Divisions of Microbiology and Immunology and through the Centers for Disease Control .
Clinical and Diagnostic Microbiology
Emory University Hospital and Grady Memorial Hospital have outstanding resources in diagnostic and clinical microbiology.
Areas of focus include:
- Development and assessment of diagnostic tools based on nucleic acid detection
- Optimization of laboratory procedures for diagnosis of mycobacterial infections
- Assessment of the accuracy of automated systems for detection of antimicrobial resistance
Clinical/Translational Research Opportunities and Global Health
Major areas of focus for clinical/translational research in infectious diseases include:
- HIV/AIDS; access to and retention in care
- Sexually transmitted infections
- C. difficile infections; prevention and treatment modalities
- Tuberculosis
- Vaccine research
- Healthcare epidemiology and healthcare infections
- Transplant Infectious Diseases
- Emerging infectious diseases
- Global health
- Bioterrorism
Clinical research training opportunities are enhanced by the presence of Clinical Interaction Sites at the Emory-affiliated hospitals .
In addition, opportunities for clinical and translational research training are enhanced by the presence of the NIH-funded CTSA award ( Georgia Clinical and Translational Science Alliance , or CTSA) which was awarded to Emory University in collaboration with Morehouse School of Medicine and the Georgia Institute of Technology. A major component of the ACTSI is the Research Education, Training and Career Development program, which includes the Master of Science in Clinical Research (MSCR).
- Make a Gift
- Education & Training
- Global Health Security
- Emerging Infectious Diseases and Epidemics
- Medical and Public Health Preparedness and Response
- Deliberate Biological Threats
- Opportunities and Risks in the Life Sciences
- Preferred reporting items for epidemic forecasting and prediction research: the EPIFORGE 2020 statement
- Rad Resilient City Initiative
- Protecting Building Occupants from Exposure to Biological Threats
- How to Lead during Bioattacks
- Publications
- Assumptions of US PPE Needs for COVID-19
- Tips to Improve Indoor Ventilation in K-12 Schools
- Tips to make the air in your home safer during COVID-19
- COVID-19 Congressional Testimonies & Briefings
- COVID-19 Fact Sheets
- COVID-19 Situation Reports
- CommuniVax Roundups
- Testimonies & Briefings
- Post-Pandemic Recovery: From What, For Whom, and How?
- National Strategy for Improving Indoor Air Quality
- A National Conversation on Indoor Air & K-12 Schools During the COVID-19 Pandemic
- Global Forum on Scientific Advances Important to the Biological and Toxin Weapons Convention
- Events Archive
- Catastrophic Contagion
- Atlantic Storm
- Dark Winter
- Newsletter: Health Security Decoded
- Call for Papers
- The Capitol Hill Steering Committee
Disease X Medical Countermeasure Program
When will the next pandemic occur.
Any Time. Infectious disease outbreaks now occur 3 times more often than 40 years ago.
WHAT IS MOST LIKELY TO CAUSE THE NEXT PANDEMIC THREAT?
We don’t know. But, of about 2 dozen viral families capable of infecting humans, 6 families (Adenoviridae, Coronaviridae, Orthomyxoviridae, Paramyxoviridae, Picornaviridae, and Poxviridae) have these traits that will likely cause the next pandemic.
- No immunity – No preexisting immunity in the world’s population
- Airborne – Spread via respiratory transmission
- Silent – Transmissible by infected people who have no symptoms
- Harmful – No existing, effective therapeutics or vaccines
ARE WE PREPARED TO MAKE VACCINES, ANTIVIRALS, AND TESTS EVEN FASTER DURING THE NEXT PANDEMIC?
No. Currently there is $0 sustained federal funding dedicated to developing medical countermeasures for unknown viral threats.
Developing the COVID-19 vaccines in 1 year was only possible because of 15 years of prior coronavirus research + a $12 billion federal investment.
HOW CAN WE MAKE MEDICAL COUNTERMEASURES WITHOUT KNOWING WHICH DISEASE (“DISEASE X”) WILL STRIKE NEXT?
By focusing medical countermeasure development efforts on the viral families most likely to cause pandemics, rather than on a specific virus that may or may not present a future threat.
The United States should fund a new dedicated Disease X Medical Countermeasure Program that leverages technologies and vaccine platforms most suitable to the viral families that are likely to cause future catastrophic disease outbreaks. Medical countermeasures against 1 member of a viral family could easily be adapted to another member quickly when the next threat emerges. With this flexible approach, private–public partnerships could develop vaccines , antivirals , and tests for a range of unknown potential pandemic pathogens in months, not years. Stopping the next COVID-19-type pandemic a month earlier in the United States would save approximately $500 billion.
Infographic
View the full infographic below, or download the PDF here .

Additional Information
The Characteristics of Pandemic Pathogens
Expediting Development of Medical Countermeasures for Unknown Viral Threats
- Find It Fast
- The PCORI Strategic Plan
- Our Programs
- Our Vision & Mission
- Financial Statements and Reports
- Board of Governors
- Methodology Committee
- Authorizing Law
- Planning Our Organizational Learning, Reporting Our Results
- Evaluating Key Aspects of Our Work
- PCORI Evaluation Group (PEG)
- Advisory Panel Openings
- Advisory Panels FAQs
- Application Review and Selection Process
- Procurement Opportunities
- Provide Input
- Explore Our Portfolio
- About Our Research
- PCORI in the Literature
- Peer Review
- Putting Evidence to Work
- Evidence Updates
- Evidence Synthesis Reports and Interactive Visualizations
- Emerging Topics: Reports and Horizon Scans
- PCORI Stories
Highlights of PCORI-Funded Research Results
- Cardiovascular Disease
- Intellectual and Developmental Disabilities
- Maternal Morbidity and Mortality
- Rare Diseases
- Women's Health
- View All Topics
- Foundational Expectations for Partnerships
- Foundational Expectations in Action
- The Value of Engagement in Research
- Engagement Award Program
- Engagement Resources
- Engagement in Health Research Literature
- Influencing the Culture of Research
- Engage with Us
Funding Opportunities
- All Funding Opportunities
- What & Who We Fund
- PCORI’s Research Funding Process
- What You Need to Know to Apply
- Merit Review
Applicant and Awardee Resources
- View All Events
- Call for Poster Abstracts
- Scholarships for Patients, Caregivers and PCORI Ambassadors
Jump to Section
Rare disease and research engagement (rare), project summary.
Designing comparative effectiveness research for rare diseases is challenging. For any rare disease, sample size is small, natural history is not well defined, and treatment approaches are often empirical. However, many patients with rare diseases share common challenges, offering the opportunity to develop cross-cutting research with impact throughout the rare disease community. One such common challenge is the high rate of mental health disorders experienced by rare disease patients; the incidence of mental health disorders is significantly higher in individuals with rare diseases, compared to the general public.
Proposed Solution: The Rare Disease and Research Engagement (RaRE) project will develop a Rare Disease Partnership Model and stakeholder-informed patient-centered outcomes research (PCOR) priorities at the intersection of rare disease and mental health. Objectives:
- Build national network of diverse rare disease stakeholders interested in PCOR for rare diseases
- Develop a comprehensive engagement model and governance structure to enhance collaborations among disparate rare disease communities for PCOR partnership
- Identify cross-cutting patient-centered outcomes and research questions amenable to pragmatic CER studies
- Develop a roadmap to implement and sustain robust stakeholder engagement in cross-cutting rare disease PCOR
Activities:
- Adopt governance document
- Conduct literature review/environmental scan
- Develop stakeholder engagement plan
- Host community convening
- Identify patient-centered outcomes and quality-of-life measures at intersection of rare disease and mental health
- Prioritize research questions for rare disease/mental health
- Adopt dissemination strategy
- Develop roadmap for sustaining meaningful engagement of diverse groups of stakeholders
Outcomes and Outputs:
Short-term: Establish opportunities for multi-stakeholder partnerships to support rare disease PCOR.
Medium-term: Generate a Rare Disease Partnership Model and stakeholder-informed rare-disease PCOR priorities.
Long-term: Researchers will implement cross-cutting rare disease PCOR with potential for broader generalizability and uptake.
- PCORI’s rare disease funding portfolio will be expanded.
- PCORI-funded cross-cutting PCOR in rare diseases will generate evidence to inform decision making for patients living with these conditions.
- Patients living with rare disease will experience better health outcomes and quality of life.
Patient and Stakeholder Engagement Plan: The plan will focus on three issues: how to ensure meaningful engagement of people on the project team; outline strategies for recruiting a diverse group of people who represent various stakeholder groups to attend the community convening; how to sustain a robust national group of stakeholders across rare disease communities for future work (Rare Disease Partnership Model). The stakeholder engagement plan will be written with input from the project team and will include: goals for engagement, partner roles, engagement structure, recruitment strategy, stakeholder orientation and preparation, and retention of stakeholders. This plan will be reviewed and adapted, as necessary, by the project team.
Collaborators: PCORI Ambassadors, members of the PCORI Rare Disease Advisory Panel, patients, caregivers and family members, providers, representatives of patient and disease-specific organizations, payers, and researchers.
Project Information
- Engagement Award Conference
- Medicine >
- Education & Training >
- Fellowship Programs >
- Infectious Disease >
- Research and Scholarship >
Potential Research Project Topics
Explore the wide range of research subjects you can undertake with the guidance of dedicated, enthusiastic faculty.
Topics for research projects with specific investigators include:
- Acinetobacter baumannii pathogenesis ( Thomas Russo )
- Bioinformatics ( Elaine Haase ; Alan Lesse ; Kedar Aras ; Marc Halfon )
- Drug development ( Thomas Suchyna ; Thomas Russo )
- Epidemiology of New Delhi Metallobetalactamases (NDM) producing Enterobacteriaceae in Michigan ( Gurmat Gill )
- Epidemiology of vancomycin resistant Enterococcus infections in patients with malignancies ( Nikolaos Almyroudis )
- Extraintestinal pathogenic Escherichia coli pathogenesis ( Thomas Russo )
- Host-pathogen interactions ( Michelle Visser ; Thomas Russo )
- Increasing Awareness and Health – Quality Improvement Project ( Gurmat Gill )
- Infectious Diseases ( Raymond Cha ; Alan Lesse ; Surksha Sirichand )
- Influence of female education on female autonomy and empowerment, and its role in influencing the future generation ( Gurmat Gill )
- Innate Immunity ( Brahm Segal ; Spyridon Stavrou )
- Intestinal pathogenic Escherichia coli pathogenesis ( John Crane )
- Investigating malaria prevalence and epidemiology in the Brazilian State of Acre ( Gurmat Gill )
- Klebsiella pneumoniae pathogenesis ( Thomas Russo )
- Mechanism of Emergence of Antibiotic Resistance ( John Crane )
- Microbial pathogenesis ( Amy Jacobs ; Thomas Melendy ; Thomas Russo ; Anthony Campagnari ; John Crane )
- Opportunistic infections in the immunocompromised host ( Nikolaos Almyroudis )
- Resistant bacteria in patients with malignancies ( Nikolaos Almyroudis )
- Role of nitric oxide in host defense in the intestinal tract ( John Crane )
- Role of zinc in intestinal infection ( John Crane )
- Supervision At a Glance – Quality Improvement Project ( Gurmat Gill )
- Vaccine development ( Timothy Murphy ; Joseph Bertino ; Thomas Russo ; Anthony Campagnari ; Terry Connell )
Director's Welcome

From the minute you join our fellowship program, you’ll work with highly qualified, friendly faculty.
- 5/10/23 Read the director’s welcome letter
Choosing the right Fellowship

Discover the components of a rewarding infectious disease fellowship. Find out how to select a program that fosters your development as a physician-scientist.
Upcoming Events
About buffalo.

Infectious Disease Topics A-Z
See our current Projects Newsletter sign up
A comprehensive list of infectious diseases that CIDRAP covers. Our site is an authoritative, reliable, and timely source of science-based information about global, emerging infectious diseases.
Our underwriters
Unrestricted financial support provided by.

- Antimicrobial Resistance
- Chronic Wasting Disease
- All Topics A-Z
- Resilient Drug Supply
- Influenza Vaccines Roadmap
- CIDRAP Leadership Forum
- Roadmap Development
- Coronavirus Vaccines Roadmap
- Antimicrobial Stewardship
- Osterholm Update
- Newsletters
- About CIDRAP
- CIDRAP in the News
- Our Director
- Osterholm in the Press
- Shop Merchandise
- Open access
- Published: 17 April 2024
MODELS: a six-step framework for developing an infectious disease model
- Jia Rui 1 , 2 na1 ,
- Kangguo Li 1 , 2 na1 ,
- Hongjie Wei 1 , 2 na1 ,
- Xiaohao Guo 1 , 2 ,
- Zeyu Zhao 1 , 2 ,
- Yao Wang 1 , 2 ,
- Wentao Song 1 , 2 ,
- Buasiyamu Abudunaibi 1 , 2 &
- Tianmu Chen ORCID: orcid.org/0000-0003-0710-5086 1 , 2
Infectious Diseases of Poverty volume 13 , Article number: 30 ( 2024 ) Cite this article
265 Accesses
Metrics details
Since the COVID-19 pandemic began, a plethora of modeling studies related to COVID-19 have been released. While some models stand out due to their innovative approaches, others are flawed in their methodology. To assist novices, frontline healthcare workers, and public health policymakers in navigating the complex landscape of these models, we introduced a structured framework named MODELS. This framework is designed to detail the essential steps and considerations for creating a dependable epidemic model, offering direction to researchers engaged in epidemic modeling endeavors.
Graphical Abstract
Since the outbreak of the coronavirus disease 2019 (COVID-19) pandemic, numerous COVID-19 modelling studies have been published. Although some proposed models are noticeable and exhibit creative designs, others contain methodological errors. Considering advancing of knowledge regarding disease epidemic characteristics, transmission patterns, control strategies, and the impacts of public health and social measures (PHSMs), researchers have increasingly utilized mathematical language and models to quantitatively elucidate the dynamics of disease spread among hosts, as well as the interplay between etiology and the environment. This endeavor has culminated in the development of theoretical epidemiology, enabling a comprehensive exploration of the effects of diverse preventive and control measures. However, epidemiological models of various diseases are often constrained by inherent limitations arising from the challenges of model selection and construction.
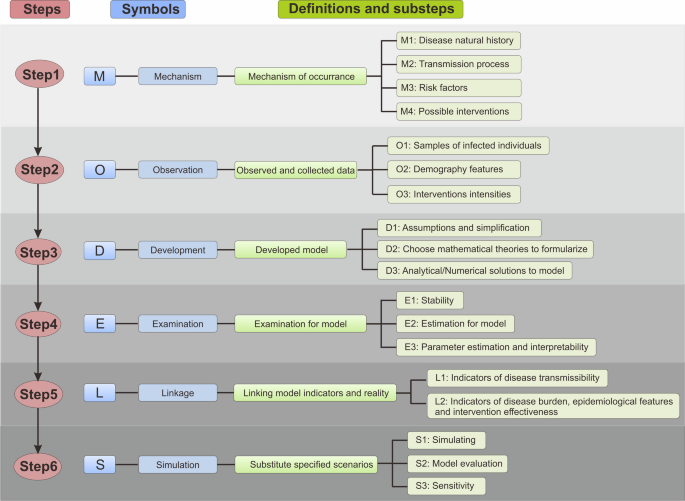
Grappling with the diverse content of these models is challenging for beginners, primary health workers, and public health officials. In this study, we developed a novel framework for developing an infectious disease model called MODELS, comprising six steps: (1) Mechanism of occurrence, (2) Observed and collected data, (3) Developed model, (4) Examination for model, (5) Linking model indicators and reality, and (6) Substitute specified scenarios.
We also outline the process of model construction (Fig. 1 ), establish an infectious disease modelling framework, and provide researchers with valuable insights into future modelling endeavors. Our proposed framework provides guidance for researchers interested in epidemic models.

- MODELS framework
M: Mechanism of occurrence
The first step, the mechanism of occurrence in infectious diseases, involves a complex interplay of factors that determine the development, transmission, and control of these diseases. Understanding the mechanism of occurrence is fundamental for accurate modelling and prediction of disease dynamics, as well as for developing effective intervention strategies. In this section, we delve into the key components that constitute the mechanism of occurrence, including the natural history of disease, transmission process, risk factors, and possible interventions. During determining the process of mechanism of occurrence in infectious diseases, we often encounter various challenges. This is particularly true in the early stages of a novel infectious disease outbreak, where there tends to be a lack of clear understanding of its natural history. Therefore, it is essential to integrate and continuously update data from clinical, epidemiological, and laboratory studies in order to ensure the reliability of these parameters.
M1: Disease natural history
The natural history of a disease encompasses its entire trajectory, starting from its onset and progressing through various stages to its outcome without any treatment or intervention [ 1 ]. In the first step of modelling, it is necessary to consider whether to develop the study at the individual perspective or at the group perspective. The disease process is characterized by dynamic changes in an individual's status, including susceptible individual, exposed individual, symptomatic or asymptomatic infected individual, and recovered individual. From the group perspective, this means that the population is divided into groups based on their status at different times, these categories have similar transmission characteristics and don’t need to consider differences at the individual level.
When considering the natural history, the key epidemiological characteristics of the infectious disease are considered, including infectivity, pathogenicity, and virulence. It is essential to elucidate the natural history of the disease process by tracking these status updates. The status flowchart varies depending on the specific type of infectious disease.
M2: Transmission process
Developing a dynamic transmission model requires a comprehensive understanding of the disease, encompassing various aspects such as transmission patterns, incubation periods, infectious periods, and population demographics. Selecting an appropriate modelling approach relies on understanding the primary modes of transmission, such as respiratory droplets, direct contact, and vector-borne transmission through organisms such as mosquitoes.
Transmission dynamic models are based on essential characteristics known as the "three links" (infectious source, transmission route, and susceptible population) and the "two factors" (natural and social factors). These models consider multiple transmission routes, including human-to-human, environmental (e.g., through food or water), and vector-to-human transmission. Additionally, the influence of natural factors, such as environmental conditions like temperature and humidity, on pathogen survival and transmission is considered.
Dynamic transmission models incorporate practical control measures to align with real-world transmission and disease control efforts. These measures encompass both pharmacological interventions, such as antiviral drugs, antibiotics, and vaccines, and non-pharmacological interventions, such as contact tracing, testing and screening, school closures, hand hygiene, social distancing, and mask-wearing. Environmental disinfection, drinking water treatment, and vector control strategies are also considered.
R3: Risk factors
Risk factors play a critical role in the transmission and impact of infectious diseases. By understanding and identifying these factors, we can gain insights into the vulnerability of populations, the severity of disease outcomes, and the potential for disease spread. In this section, we explore two broad categories of risk factors: nature and social factors (Fig. 2 ).

Risk factors on disease transmission
M3.1 Nature factors
Nature factors include a range of environmental, geographic, and ecological factors that influence the prevalence and distribution of infectious diseases. For example, meteorological factors, such as temperature, humidity, and rainfall patterns, directly affect the activity and transmission of pathogens. Geographic factors, including terrain, proximity to water bodies, and elevation, can affect the distribution of disease vectors or reservoirs. Ecological factors consider the intricate interactions among pathogens, hosts, and the environment, highlighting the complex dynamics that contribute to disease emergence and persistence.
Geographical factors have a significant impact on disease prevalence. The distribution of diseases and their vectors is influenced by the terrain, proximity to water bodies, and elevation. For example, the geographical distribution of vector organisms varies considerably. Meteorological factors play crucial roles in the transmission dynamics of insect-borne infectious and zoonotic diseases. Temperature directly affects the activity and growth cycles of insect vectors. Furthermore, temperature also has a greater impact on respiratory infectious diseases; lower temperatures during winter, combined with weakened human resistance, tend to result in a higher incidence of respiratory infections such as influenza.
Ecological and meteorological factors significantly contribute to the prevalence of infectious diseases. These factors encompass the intricate interactions between pathogens, hosts, and the environment. Disruptions in ecosystems, such as habitat fragmentation, deforestation, and changes in land use, alter the distribution and abundance of disease vectors and reservoirs, leading to increased contact between humans, wildlife, and vectors. This heightened interaction facilitates the spillover of zoonotic diseases into human populations. The ecological balance within ecosystems plays a crucial role in the amplification or suppression of infectious diseases.
M3.2: Social factors
Social factors encompass various societal and behavioral aspects that influence the transmission of infectious diseases. These factors include socioeconomic conditions, living standards, healthcare access and infrastructure, educational levels, cultural practices, and population density.
Socioeconomic conditions and living standards significantly affect the disease spread. Access to clean and hygienic living environments free from toxins is essential for reducing the occurrence of certain diseases.
Healthcare access and the level of public health services are critical factors affecting infectious disease outcomes [ 2 ]. Improved medical and health conditions coupled with robust public health measures enhance disease prediction, diagnosis, and treatment. Increased vaccine coverage and improved detection systems reduce the incidence of infectious diseases.
Moreover, the social system and speed of government response significantly affect epidemic control. The strict enforcement of importation measures, quarantine protocols, and effective treatment strategies have proven crucial in containing the spread of infectious diseases, as exemplified during the COVID-19 pandemic.
Recognizing the interplay between social factors and infectious diseases is vital for effective disease management and prevention. By understanding the societal context, interventions can be tailored to address specific risk factors and promote behavioral changes. To achieve comprehensive and sustainable disease control, collaboration between PHSMs and environmental factors is essential.
Overall, a comprehensive understanding of the social factors and other epidemiological considerations is crucial for designing and implementing effective strategies to mitigate the impact of infectious diseases and protect public health.
M4: Possible interventions
According to the characteristics of various infectious diseases, integrated interventions are implemented to prevent the continued spread of infectious diseases by targeting the leading links of transmission. Three basic components of the epidemiological process of infectious diseases are targeted (Fig. 3 ).

The process by which interventions affect the transmission process of infectious diseases
M4.1: Managing sources of infection
The key elements include: (1) timely reporting of infectious diseases; (2) control measures for patients, carriers, and close contacts; (3) control measures for animal sources of infection; (4) measures for environmental contamination of infected sites.
M4.2: Interrupting transmission routes
Specific measures are employed that are based on the transmission process of the infectious diseases: (1) intestinal infectious diseases: effective management of the disposal of feces and other contaminants and environmental disinfection; (2) respiratory infectious diseases: air disinfection, ventilation, and personal protection (e.g., wearing masks); (3) zoonotic diseases: insecticide and pest control; (4) infectious diseases with complex transmission routes: establishment of comprehensive protective measures to address various transmission patterns.
M4.3: Safeguarding highly susceptible populations
Primary measures include vaccination, developing an immune barrier, providing preventive medications to people at risk, and taking personal protective measures.
O: Observed and collected data
Observation and data collection are essential for modelling infectious diseases. These activities help determine the epidemiological characteristics of infectious diseases, such as the rate of virus transmission, incubation period, and mode of transmission, which are essential for the accurate modelling and prediction of disease spread. By analyzing the epidemic data, we can forecast the trajectory and magnitude of future outbreaks, assess the effectiveness of control measures, and optimize disease control strategies. For some researchers with primary data, people who work at the center for disease control and prevention or in hospitals, it is often easier to proceed in this step, and they have an established system for data such as disease or vector surveillance. For researchers who do not have access to primary data, there may be some challenges at the step of obtaining accurate and usable data sources. They may only be able to choose open source databases for their research.
O1: Samples of infected individuals
Case-specific information is essential for understanding the dynamics of infectious diseases. On-site surveys or historical surveillance data are used to gather data on infected individuals. The stratification of infections based on different dimensions is often necessary.
O2: Demography features
In our increasingly interconnected world, demographic factors play a significant role in disease transmission. Factors such as urbanization, population aging, travel, and migration contribute to the spread of epidemics. Understanding the links among environmental factors, human health, and disease transmission is crucial. Global climate change, for example, affects the distribution of vector-, food-, and water-borne diseases and interacts with vulnerability factors and disease transmission dynamics. Additionally, health equity is closely tied to economic growth, healthcare resources, and accessibility of educational resources. Gathering demographic data, such as birth rates, death rates, population numbers, and migration patterns, from reliable sources such as the World Health Organization (WHO), World Bank, or national statistical yearbooks, helps inform modelling efforts and assess disease risk.
O3: Intervention intensities
Incorporating interventions into disease models allows the estimation of the impact of improved diagnostics, new drugs, and different control measures. Data on intervention parameters such as treatment efficacy, diagnostic accuracy, and implementation coverage are typically obtained through a thorough review of the scientific literature and relevant studies. These data help assess the effectiveness and cost-effectiveness of interventions in controlling infectious diseases.
The accuracy and validity of infectious disease models can be enhanced by systematically collecting and analyzing relevant data during the observation and data collection phases. This enables researchers to generate more reliable predictions and develop effective strategies for disease control and prevention. Once the necessary data are collected and observed, the next step is to develop a mathematical model representing the transmission dynamics of the infectious disease.
D: Developed model
Developing a mathematical model representing the transmission dynamics of infectious diseases is a crucial step in epidemiological research. This model is a powerful tool for simulating and understanding how a disease spreads within a population, enabling the exploration of different scenarios, assessment of intervention strategies, and prediction of future trends. It's important to note that the construction of models should be based on the type of disease, research objectives, and available data. In this section, models are categorized into data-driven models and mechanism-driven models. In “ Choose mathematical theories to formalize ”, it is mentioned that different models should be selected based on varying conditions.
D1: Assumptions and simplification
To select the most appropriate model, researchers start with an existing qualitative understanding of the epidemiological process of the disease and then select it concerning the disease type and the study objectives.
D1.1: Type of disease
Infectious diseases are diseases that arise when a pathogen infects an organism and can be transmitted from person to person, animal to animal, or animal to human. Many different types of infectious diseases have been observed, each of which can be broadly classified according to its transmission characteristics as gastrointestinal, respiratory, contact, blood, and sexually transmitted diseases, as well as animal- and vector-borne infectious diseases. Depending on the categories to which the disease under study belongs, researchers can choose between a purely human-to-human transmission model or a cross-population transmission model.
D1.2: Objectives of the study
Models can be used to express the epidemiological process of a disease in symbolic numerical formulas that quantitatively reveal inner laws, and are used for analysis, interpretation, prediction, control, or decision evaluation. Further analytical studies of various types of infectious diseases, specifically disease prediction, estimation of transmission capacity, and evaluation of the effectiveness of interventions, are carried out. For example, when simulating the effects of an intervention, the parameters and links to be evaluated for a single intervention or a combination of interventions must be matched, and the parameters are further supplemented or adjusted to evaluate the effects of intervention [ 3 ]. It is often possible to construct a transmission model with single or multiple control measures to simulate epidemic trends with single or combined measures, and thus assess the effectiveness of a particular control measure [ 3 , 4 ].
D2: Choose mathematical theories to formularize
We classified mathematical models as either data-driven or mechanism-driven (Table 1 ). Data-driven models predominantly focus on extracting insights and making predictions from existing datasets, while mechanism-driven models concentrate more on formulating models based on the biological and sociological principles underlying disease transmission. These models hold distinct applicative values in varying contexts. In scenarios characterized by the availability of substantial high-quality data combined with a lack of understanding of the underlying mechanisms, the selection of data-driven models is advisable. Conversely, when there is a comprehensive understanding of the mechanisms involved or examining the effects of various intervention strategies, mechanism-driven models become the preferred choice. In practical applications, it is often beneficial to integrate both types of models, enabling a more holistic understanding and effective response to the challenges posed by infectious diseases.
D2.1: The data-driven model
The data-driven model contains a series of models exploring the relationship between disease occurrence and time, which is an important topic in the mathematical modelling of infectious diseases in China. Common methods include time regression, control graph, time series, autoregressive integrated moving average (ARIMA), Monte Carlo algorithm, grey theoretical, and neural network models.
D2.2: The mechanism-driven model
The mechanism-driven model is classified by different research object types and parameters, including (1) group and deterministic models, such as transmission dynamics models, and (2) individual models and random models, such as agent-based models, multi-agent systems, and cellular automata.
D3: Analytical/Numerical solutions to model
Except for highly simple models that can be solved analytically, almost all models are too complicated to find analytical solutions and can be solved numerically, such as by using a computer. In general, the procedure employs model formularization techniques to find solutions for the model. The existence and uniqueness of the model solution are inspected in this step. If a solution does not exist, then the model development process must be re-checked. In some large projects, this step may be called “build a computational model for the model.”
E: Examination for model
After developing and analyzing a mathematical model of infectious disease transmission, it is crucial to thoroughly examine and evaluate it. This step is essential for assessing the validity and accuracy of the model and identifying potential areas for improvement. Examining the performance of the model can ensure that it aligns with empirical observations and provides meaningful insights into the dynamics of infectious diseases. Ensuring model stability is an essential aspect of working with mathematical or statistical models in the step of examination, particularly when they are applied to complex systems like the dynamics of infectious diseases. This process involves both statistical techniques and comparisons with empirical data.
E1: Stability
Model stability refers to the degree of consistency in the output of a model when slight variations in the epidemic data are observed [ 5 ]. In epidemiological research, models are often used to predict disease transmission trends, assess the effectiveness of interventions, and provide a theoretical basis for public health decision-making. If a model lacks stability, even minor changes in the input data can lead to significant variations in the output, thereby affecting our understanding of disease dynamics and the accuracy of intervention strategies.
E2: Estimation for model
When a model is developed with a specified formulation using specific knowledge of the mechanism and mathematics, it must be examined before it can be used for prediction, estimation, or other applications. First, it must be determined whether the model is self-consistent; that is, it should not be contrary to existing theories. For example, if a model asserts that “a basic reproduction number less than 2 means the disease will spread over almost the entire population,” then something has gone wrong. Second, the model must be well organized and robust to small amounts of noise and missing data. Such an examination involves a stability analysis of the model equations, and error analysis of the numerical methods used to solve the model numerically. After the behavior of the model is tested analytically or numerically, it still must be confirmed that the model explains the data that are already accumulated and whether it is better than the existing models. In such an analysis, modelers may implement parameter fitting, smoothing, or filtering techniques to estimate the state variables and parameters [ 6 , 7 ].
E3: Parameter estimation and interpretability
Parameters can usually be divided into two categories: scenario- and disease-specific. Scenario-specific parameters refer to the differences in transmission from different locations, populations, and times, which are represented by the transmission rate coefficient. The initial values of various variables, such as the number of susceptible persons, infectious sources, and immunized populations in the study area, must be set after parameter estimation. Disease-specific parameters are commonly used in natural history. In infectious disease modelling, the calculation and acquisition of parameters such as incubation period ( ω ), disease duration ( γ ), etc. usually involves the following methods: literature review, epidemiological surveys, and data analysis by descriptive statistics.
E3.1: Estimation of transmission-specific parameters
Transmission-specific parameters mainly include transmission rate ( β), population exposure, and probability of infection for a single exposure. Such parameters can be estimated in two ways: through field surveys, such as exposure surveys, and simulations, e.g., the fitting of actual epidemic data.
In the cross-sex model, β must be split into the transmission rates between male to male ( β mm ), male to female ( β mf ), female to female ( β ff ), and female to male ( β fm ). In the model across age groups, β must be split into transmission rate between different age groups ( β ij ) and transmission rate within age groups ( β ii ). In the case of models that consider contaminants in the environment, the environmental transmission coefficient to the population ( β w ) also must be considered. In the case of cross-population models, the transmission coefficient ( β a ) of the animal or vector to the population also must be considered.
E3.2: Estimation of disease-specific parameters
Disease-specific parameters usually refer to disease natural history parameters, such as ω , latency period ( ωʹ ), γ , infectious period, proportion of occult infections ( p ), proportion of severe cases ( p s ), and mortality ( f ). Such parameters are relatively variable among different disease species, and differences in parameters between regions for the same disease are usually less pronounced than those between different disease species. When modeling, such parameters can be obtained through first-hand data in the field or through references as they are more difficult to obtain in the field; sensitivity analysis or uncertainty analysis should be carried out appropriately for parameters from references.
E3.3: Estimation of intervention-specific parameters
Currently, the main preventive and control measures for infectious diseases include pharmacological (vaccination and medication) and nonpharmacological interventions (isolating patients, wearing masks, increasing social distancing, etc.). The effectiveness of non-pharmacological interventions has been confirmed by multiple studies; they successfully control the prevalence of various diseases through the strict implementation of various public health policies, such as isolating cases, tracing close contacts, and social distancing. The corresponding parameter for isolating cases is increasing the isolation coefficient ( φ ), increasing the social distance is reflected in the population contact degree ( x ), and wearing a mask is reflected in changing the probability of infection with a single-contact infection rate ( p ). The study evaluates the effectiveness of vaccination, mainly including the vaccination rate ( δ ) and the vaccine effect parameters. In terms of medication treatment, studies have evaluated the prevention and control effect of the population; the main parameters include the shortening of disease duration ( γ ), the reduction of patient severe illness rate ( q ), and the reduction of severe case fatality rate ( f c ).
L: Linking model indicators and reality
The goal of developing mathematical models for infectious disease transmission is to bridge the gap between theoretical insights and practical applications. Although models provide valuable insights into the dynamics of disease spread, it is crucial to establish a strong link between model indicators and real-world observations. This ensures that the predictions and recommendations of the model are relevant, reliable, and actionable for disease control and prevention. Finding appropriate and accurate indicators based on the scientific questions posed by different studies may be challenging for some of the researchers who are at the beginning of their research work.
L1: Indicators of disease transmissibility
The basic reproduction number ( R 0 ) is an important indicator of the transmissibility of an infectious disease. R 0 is defined as the number of new cases generated by an infected individual in an otherwise fully susceptible population in the absence of interventions. A greater R 0 value indicates greater transmissibility of the infectious disease [ 8 ].
When R 0 < 1, the disease will not cause an epidemic, the number of infections will decrease, and the disease will be gradually eliminated. When R 0 > 1, the disease will cause an epidemic. Thus, R 0 = 1 is the threshold for the transmission of infectious diseases [ 9 ].
This definition indicates that the calculation of R 0 requires more stringent conditions, that is, the entire population is susceptible. The proportion of the susceptible population declines gradually as the epidemic progresses or interventions are implemented; at this point, it is no longer appropriate to use R 0 to measure propagation capacity. The effective reproduction number ( R eff, ) or the time-varying reproduction number ( R t ) should be applied [ 10 ].
L2: Indicators of disease burden, epidemiological features, and intervention effectiveness
The total attack rate (TAR) is the percentage of cumulative cases of a disease in the total population during an epidemic:
The total asymptomatic infection rate (AIR) is the percentage of cumulative asymptomatic infections caused by a disease in the total population during an epidemic:
The total infection rate (TIR) is the percentage of cumulative infections of a disease in the total population during an epidemic:
Thus, TIR = TAR + AIR.
Duration of outbreak (DO) is the time interval from the start of transmission of the infectious disease to the end of the outbreak [ 1 ]. DO can be defined in two ways: the time interval from the first case onset to the last case onset, that is, calculated from the epidemic curve; and the time interval from the first case onset to the last case recovery. It is calculated as follows:
where t 1 is the date of onset of the first case and t 2 is the date of onset or recovery of the last case.
Peak incidence is the maximum incidence or number of infectious diseases at the shortest wcalculated time (e.g., day or week) during an epidemic.
The time of peak incidence is the specific time (e.g., date) at which the peak incidence of a disease occurs during an epidemic.
The severity rate is the proportion of severe cases in the total cases and is one of the most important indicators of virulence.
Mortality rate indicates the proportion of deaths due to a disease among patients with that disease in a certain period and indicates the risk of death for patients with that disease [ 1 ]:
Secondary attack rate (SAR), also known as secondary incidence rate, is an important indicator used to measure the spread of an infectious disease. It is the percentage of susceptible contacts who develop a disease between the shortest and longest incubation periods for certain infectious diseases as a percentage of the total number of all susceptible persons:
S: Substitute specified scenarios
In infectious disease modelling, the ability to substitute specified scenarios is a fundamental step in bridging theoretical insights with practical applications. By simulating and assessing specific scenarios, researchers can gain a comprehensive understanding of the potential outcomes of various interventions and policy measures.
S1: Simulating
Building on the groundwork laid out in the previous five steps, the next crucial phase involves running the infectious disease model using computational methods to simulate various disease transmission scenarios. Different diseases exhibit unique modes of transmission – airborne, vector-borne, or direct contact – each necessitating tailored modelling approaches. For instance, models for airborne diseases like influenza might emphasize social interactions and mobility patterns, while those for vector-borne diseases such as malaria need to factor in environmental influences and vector population dynamics. Additionally, the variability in transmission rates, incubation, and infectious periods across diseases necessitates the incorporation of these differences in scenario planning, possibly through simulations that vary contact rates or the duration of infectious periods. Population settings also play a critical role; factors like population density, age distribution, and healthcare access profoundly impact disease spread. High-density areas might require scenarios accounting for overcrowding, whereas rural areas might focus on healthcare accessibility. Cultural and behavioral aspects, such as social gathering prevalence or attitudes towards vaccination and public health practices, alongside economic factors and resource availability, are pivotal in shaping scenario development, especially in lower-income settings with limited health infrastructure. The specificity of scenarios is equally important; they must be relevant to both the disease and its context. For highly infectious diseases like COVID-19, scenarios could range from lockdown measures to mask mandates, while for Human Immunodeficiency Virus/AcquiredImmune Deficiency Syndrome (HIV/AIDS), the focus might be on awareness campaigns or antiretroviral therapy coverage. Moreover, dynamic adaptation of scenarios is essential, responding to evolving disease patterns or new data, like emerging virus variants. In this context, collaboration with public health experts and epidemiologists who have insights into local conditions and disease specifics is invaluable, enhancing both the relevance and effectiveness of the proposed scenarios in model stability assessment.
Researchers can choose to either develop their custom model code or utilize pre-existing packages specifically designed for infectious disease modelling, such as the SimInf and EpiModel packages in R ( https://www.r-project.org/ ), or the epydemic and Eir packages in Python ( https://www.python.org/ ).
Using simulation, researchers can explore the dynamic behavior of the disease under different conditions and interventions. The model generates predictions and projections by the input of specific parameters and variables, thereby providing valuable insights into the potential outcomes of various interventions and policy measures. Simulations enable the assessment of the effectiveness of different control strategies and the evaluation of the impact of preventive measures on disease transmission.
S2: Model evaluation
Model fitting methods typically include the least squares estimation (LSE), maximum likelihood estimation (MLE), root mean square estimation (RMSE), akaike information criterion (AIC), and bayesian information criterion (BIC). For differential equation models, an algorithm that uses an adaptive step selection strategy, along with the fourth-order Runge–Kutta method with equidistant nodes as the discretization method, is a common algorithm for solving initial-value problems for ordinary differential equations (Table 2 ).
Further goodness-of-fit tests are required to determine whether the differences between the model results and actual data are statistically significant; the goodness-of-fit tests used include the chi-square test. The coefficient of determination ( R 2 ) can also be calculated and tested for statistical significance. Cox regression can be used to analyze the vaccine effects to determine the time of entry into the group and the time to the endpoint. Methods such as multiple regression analyses and generalized linear models are often used to reconcile confounding factors when analyzing influences. Commonly used software includes SPSS ( https://www.ibm.com/spss ), SAS ( https://www.sas.com/ ), R ( https://www.r-project.org/ ), Python ( https://www.python.org/ ), MATLAB ( https://www.mathworks.com/products/matlab.html ), and Berkeley Madonna ( https://berkeley-madonna.myshopify.com/ ).
If the model evaluation results are unsatisfactory, it is necessary to revisit Step 3 and reevaluate the model assumptions and construction. This iterative process ensures that the model aligns with real-world observations and produces reliable and accurate predictions. Once the model evaluation results meet the desired criteria, researchers can proceed with the infectious disease modelling process.
S3: Sensitivity
Parameter sensitivity refers to the degree of influence the model parameters exert on the model output. In epidemiological research, a sensitivity analysis of parameters is used to assess how changes in specific parameters affect a model's results. By altering the model parameters, researchers can understand the contribution of each parameter to the outcome, allowing the modelers to optimize the model and provide more accurate predictions.
The “knock-out” simulation is derived from knock-out technology, an experimental technique used in genetics in which a normal gene is replaced by a defective gene at an identical chromosomal locus, the normal gene thereby being "knocked out" by the defective gene. In modelling studies, the simulation process sets a parameter to zero and estimates its contribution by counting the number of reduced cases or the total incidence rate. For example, in the SEIARW model, the contribution of environmentally mediated afferents is explored by setting β w to 0 and reflecting its role by counting the number of cases reduced.
The difference between model stability and parameter sensitivity lies in their respective focuses. Model stability concerns the impact of slight variations in input data on the output of the model, whereas parameter sensitivity focuses on the influence of changes in model parameters on the output. Although both concepts involve model stability and reliability, model stability primarily addresses the overall stability of the model, whereas parameter sensitivity examines the impact of individual parameters. In epidemiology, both model stability and parameter sensitivity analyses play crucial roles in understanding and improving the accuracy of epidemiological models.
Conclusions
The MODELS framework offers a systematic and comprehensive approach to develop infectious disease models. By emphasizing the importance of data collection, model formulation, consideration of social and ecological factors, and model evaluation, this framework provides a roadmap for generating reliable and actionable models. Additional file 1 is a case study based on the MODELS framework. By following the MODELS framework, researchers and policymakers can enhance their understanding of disease dynamics and make informed decisions to effectively control and prevent infectious diseases. Ultimately, this framework will contribute to global efforts to mitigate the impact of infectious diseases.
Availability of data and materials
All data and materials are from cited references.
Abbreviations
Coronavirus disease 2019
World Health Organization
Human Immunodeficiency Virus
AcquiredImmune Deficiency Syndrome
Public health and social measures
Autoregressive integrated moving average
Basic reproduction number
Effective reproduction number
Time-varying reproduction number
Total attack rate
Asymptomatic infection rate
Total infection rate
Duration of outbreak
Secondary attack rate
Least squares estimation
Maximum likelihood estimation
Root mean square estimation
Akaike information criterion
Bayesian information criterion
Coefficient of determination
CDC. Principles of Epidemiology|Lesson 1—Section 9 2021 updated 2021/12/20/. Available from: https://www.cdc.gov/csels/dsepd/ss1978/lesson1/section9.html .
Nicholson F. Infectious diseases: the role of the healthcare professional. In: Stark MM, editor. Clinical forensic medicine. Cham: Springer; 2018. p. 343.
Google Scholar
Joel E, Cohen P. Infectious diseases of humans: dynamics and control. JAMA. 1992;268(23):3381.
Article Google Scholar
Keeling MJ, Rohani P. Modeling infectious diseases in humans and animals. USA: Princeton University Press; 2007.
Parsamanesh M, Erfanian M, Mehrshad S. Stability and bifurcations in a discrete-time epidemic model with vaccination and vital dynamics. BMC Bioinf. 2020;21(1):1–15.
Wang B, Zou X, Zhu J. Data assimilation and its applications. Proc Natl Acad Sci USA. 2000;97(21):11143–4.
Article CAS PubMed PubMed Central Google Scholar
Katzfuss M, Stroud JR, Wikle CK. Understanding the ensemble kalman filter. Am Stat. 2016;70(4):350–7.
Delamater PL, Street EJ, Leslie TF, Yang YT, Jacobsen KH. Complexity of the basic reproduction number (R(0)). Emerg Infect Dis. 2019;25(1):1–4.
Article PubMed PubMed Central Google Scholar
Batista M. On the reproduction number in epidemics. J Biol Dyn. 2021;15(1):623–34.
Article PubMed Google Scholar
Gostic KM, McGough L, Baskerville EB, Abbott S, Joshi K, Tedijanto C, et al. Practical considerations for measuring the effective reproductive number, Rt. Plos Comput Biol. 2020;16(12): e1008409.
Download references
Acknowledgements
This study was supported by the National Key R&D Program of China (2021YFC2301604), Fundamental Research Funds for the Central Universities (20720230001) and the Self-supporting Program of Guangzhou Laboratory (SRPG22-007).
Author information
Jia Rui, Kangguo Li, Hongjie Wei contributed equally.
Authors and Affiliations
State Key Laboratory of Vaccines for Infectious Diseases, Xiang An Biomedicine Laboratory, School of Public Health, Xiamen University, Xiamen city, China
Jia Rui, Kangguo Li, Hongjie Wei, Xiaohao Guo, Zeyu Zhao, Yao Wang, Wentao Song, Buasiyamu Abudunaibi & Tianmu Chen
State Key Laboratory of Molecular Vaccinology and Molecular Diagnostics, National Innovation Platform for Industry-Education Integration in Vaccine Research, Xiamen University, Xiamen City, China
You can also search for this author in PubMed Google Scholar
Contributions
J.R., T.C and H.W. designed research, J.R., K.L., X.G., Z.Z., Y.W., and W.S. wrote the first draft of manuscript, J.R., K.L., X.G. and T.C. supervised, B.A. polished the manuscript. All authors contributed to revision of the manuscript critically for intellectual content and have given final approval of the version to be published.
Corresponding author
Correspondence to Tianmu Chen .
Ethics declarations
Ethics approval and consent to participate.
Not applicable.
Consent for publication
Competing interests.
The authors declare no competing interests.
Supplementary Information
Additional file 1: figure s1..
Flowchart of the susceptible-infected-recovered (SIR) model. Figure S2. Cumulative cases of EVD. Figure S3. Daily incidence of EVD. Figure S4. Simulated cumulative cases of EVD for different basic reproduction numbers and recovery rate.
Additional file 2.
Example data.
Additional file 3.
Figure drawing R code.
Additional file 4.
Sensitivity analysis R code.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Rui, J., Li, K., Wei, H. et al. MODELS: a six-step framework for developing an infectious disease model. Infect Dis Poverty 13 , 30 (2024). https://doi.org/10.1186/s40249-024-01195-3
Download citation
Received : 06 December 2023
Accepted : 11 March 2024
Published : 17 April 2024
DOI : https://doi.org/10.1186/s40249-024-01195-3
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Epidemic models
- Model construction
Infectious Diseases of Poverty
ISSN: 2049-9957
- Submission enquiries: Access here and click Contact Us
- General enquiries: [email protected]
- Institute for Cardiovascular Disease Research
- Location Location
- Contact Contact
Research Projects

Cardiovascular dysfunction accounts for some of the most common and devastating diseases in the country, as well in the institute's home state of South Carolina. This research promises to uncover new understandings and breakthroughs to reduce mortality and morbidity rates due to cardiovascular disease.
Partner with Us
Become a strategic partner by starting an applied research project with us, funding the research or collaborating with us on the work.
A Holistic, Interdisciplinary Approach to Understanding Cardiovascular Disease
The Institute for Cardiovascular Disease Research is a multi-primary investigator undertaking, with highly regarded experts in the field leading novel and unique research contributions within the four-year institute plan. We seek to provide a new understanding of the ways that body inflammation plays a part in high blood pressure and identify new treatments to reduce the frequency and impact of cardiovascular disease.
High Blood Pressure Associations with Chronic, Unpredictable Stress
The chronic, unpredictable stress that comes with the everyday realities of modern life leads to widespread inflammation in the body, which causes dysfunction in the brain, vascular system, kidneys and heart along with elevated blood pressure and, eventually, cardiac failure.
Targeting the cause of inflammation, or inflammasomes, leading to cardiovascular dysfunction may uncover important high blood pressure triggers that originate in the nervous system, and open doors to new treatment strategies.
Targeted inflammasomes: NLRP3 (nucleotide-binding domain, leucine-rich–containing family, pyrin domain–containing-3) and AIM2 (absent in melanoma 2)
Focus of the institute: Neurogenic hypertension associated with chronic unpredictable stress
Research vision: A new understanding of the molecular mechanisms of inflammation in hypertension and identify new therapeutic targets to reduce morbidity and mortality in these common and devastating illnesses
Areas of Focus
By taking an interdisciplinary approach to cardiovascular health, we will advance our understanding of how stress leading to high blood pressure impacts the brain, kidneys, blood vessels and heart causes disease that ends with cardiac failure.

Project 1: Vascular System and Stress
High blood pressure and the vascular damage it does—leading to cardiovascular disease—is an enormous emotional and financial burden on patients with chronically elevated blood pressure.

Project 2: Brain and Stress
Stress has a profound impact on the brain, mood and body including causing or affecting a number of cardiovascular and other diseases and disorders. Yet, an overwhelming majority of adults report experiencing daily stress.

Project 3: Kidneys and Stress
Patient populations with higher prevalence of autoimmune disease—like women and those of the female sex, veterans and underrepresented communities of all kinds—are also at higher risk for cardiovascular disease.

Project 4: Heart and Stress
Patient populations with higher prevalence of autoimmune disease—like women and those of the female sex, veterans and those suffering from trauma and Black and African American communities—are at higher risk for cardiovascular disease.
The highest impact research today involves leveraging multiple perspectives, skillsets and areas of expertise to come up with the most comprehensive possible understanding of or solution to a significant issue.

Challenge the conventional. Create the exceptional. No Limits.
- Services Paper editing services Paper proofreading Business papers Philosophy papers Write my paper Term papers for sale Term paper help Academic term papers Buy research papers College writing services Paper writing help Student papers Original term papers Research paper help Nursing papers for sale Psychology papers Economics papers Medical papers Blog

Top 100 Disease Research Topics For Paper Writing

Students have many disease research topics to consider when writing research papers and essays. A disease occurs when the body undergoes some changes. Science philosophy has pointed at pathogens and the causes of illness. Today, medicine focus on biochemical factors, nutrition, immunology levels, and environmental toxins as the causes of diseases. Research papers on disease topics can focus on specific illnesses independently or in groups. You can also write about infectious diseases like COVID-19 and HIV or non-communicable diseases. Non-communicable diseases are also known as chronic illnesses. These are diseases that you can’t get from a sick person. They include heart disease, cancer, stroke, and lung disease. These diseases account for up to 70% of global deaths. Nevertheless, whether you opt to write about advanced topics in Lyme disease or something simple like flu, research will be paramount. You can also buy research papers cheap, if you don’t have time for it. So, d on’t put your grade at risk and get research paper online help .
Why Choose Our Disease Research Topics?
Educators want you to convince them that you have taken the time to think about your topic and research it extensively. What’s more, your research should make a meaningful contribution to your study field. Therefore, select a good topic and research it extensively before you start writing. Analyze your information to determine what will make it to your research paper. Here is a list of 100 disease research paper topics worth considering for your paper or essay.
Top Disease Research Topics
Maybe you want to research and write a research paper on a topic that anybody will find interesting to read. In that case, consider ideas in this list of disease research topics.
- How NSAIDS lead to peptic ulcers
- What are pandemic diseases?
- What is the role of pandemic diseases in the mankind history?
- What are the symptoms of acute lung disease?
- Explain how Attention Deficit Hyperactivity Disorder affects children
- Discuss the AIDS pandemic in third world countries
- Describe the main causes of AIDS
- Explain how AIDS affects children
- Discuss the treatment of AIDS
- Is alcohol addiction a disease?
- Discuss the Alzheimer’s disease scope and how it affects the elderly persons’ brain
- How can you help dementia or Alzheimer’s disease patients and caregivers?
- What are the symptoms of Alzheimer’s disease?
- What is autoimmune disease?
- Explain how autoimmune thyroiditis begins
- Examine acute protective membrane inflammation in bacterial meningitis
- Compare pathology of AIDS and black death
- Discuss the effects of cancer in today’s society
- Autism and its causes
- Different types of cancer and their prevalence
These are topics disease experts will recommend researching and writing about. And because students can write about these topics without getting complex, anybody will find them interesting. If you’re searching for research topics on Alzheimer’s disease, this list also has some ideas for you to consider.
Infectious Disease Topics for Research Papers
Are you interested in infectious disease research topics? If yes, you will find this list interesting. This category comprises hot topics in infectious disease fields. Consider some of these ideas for your research paper.
- The virology, epidemiology, and prevention of COVID-19
- The diagnosis of COVID-19
- Prevention vaccines for SARS-CoV-2 infection
- Questions people ask about COVID-19
- Clinical features of COVID-19
- COVID-19 management in a hospital setting
- Infection control for COVID-19 in homes and healthcare settings
- Skin abscess and cellulitis in adults
- Clinical manifestation, diagnosis, and epidemiology of yellow fever
- Transmission and epidemiology of measles
- Role of untreated inflammation of genital tract in HIV transmission
- Racial inequities of COVID-19 and HIV in black communities
- Community-acquired pneumonia overview in adults
- The use of procalcitonin in the infections of lower respiratory tract
- Herpes simplex virus prevention and treatment
- Uncomplicated Neisseria gonorrhea treatment
- Society guidelines for COVID-19
- Why public education is crucial in fighting COVID-19
- Overview of Ebola over the last two decades
- Investigations into the use of monoclonal antibody in treating Ebola
This category also has some of the best infectious disease presentation topics. Nevertheless, learners should prepare to research extensively before writing academic papers on these topics.
Interesting Disease Topics
Maybe you want to research and write a research paper on a topic that most people find interesting. In that case, consider these disease topics for research paper.
- Discuss bulimia as a common eating disorder
- Why are so many young people suffering from anorexia?
- What causes most eating disorders
- How serious are sleep disorders
- Discuss rabies treatment- The Milwaukee protocol
- Is assisted suicide a way to treat terminal diseases?
- What are the effects of brain injuries?
- What are professional diseases?
- Is autism a norm variant or a disease?
- The history of pandemics and epidemics
- The role of antibiotics in treating diseases
- What causes insomnia?
- What are the effects of insomnia?
- How to cope with insomnia
- Can sleeping pills cure insomnia?
- Explain what causes long-term insomnia
- Using traditional medicine to fight insomnia
- How to deal with bulimia and nervosa
- How eating disorders affect self-harm behavior
- How feminism affect anorexic women phenomenon
This is a list of easy disease topics for papers. What’s more, most people will find these research paper disease topics interesting to read about. Nevertheless, students should take time to research their preferred topics to come up with brilliant papers on any of these human disease research paper topics.
Cardiovascular Disease Research Topics
Maybe you’re interested in topic ideas on heart disease. Perhaps, you want to write about an illness of the respiratory system. In that case, consider these heart disease research topics.
- An investigation of hypertrophic cardiomyopathy
- A research of the causes of coronary artery disease
- Antithrombotic therapy in surgical valve and prosthetic heart valve repair
- Intervention choice for severe cases of calcific aortic stenosis
- Prognosis and treatment of heart failure using preserved fraction of injection
- Infective endocarditis management in adults
- Risk assessment for cardiovascular disease for primary prevention
- Prognosis and treatment of acute pericarditis
- Treatment of reflex syncope in adolescents and adults
- Anticoagulant therapy for preventing thromboembolism in atrial fibrillation
- Cardiac manifestations of COVID-19 in adults
- Acute decompensated heart failure treatment
- What is hypertriglyceridemia?
- How to manage elevated low-density lipoprotein-cholesterol in cardiovascular disease
- Management and evaluation of cardiac disease
- Conduction system and arrhythmias disease and COVID-19
- Myocardial infarction in COVID-19
- Can somebody inherit a cardiac disease?
- How effective are treatments for irregular heartbeat?
- How to determine the risk for a sudden cardiac death
This list comprises some of the best special disease topics. That’s because most people reading about these topics might not have heard about them before. Nevertheless, this category also has interesting research topics for disease control that may help individuals that want to avoid or manage some illnesses.
Research Topics for Chronic Disease
You probably know somebody living with a chronic illness. Unlike controversial topics in infectious disease, people don’t talk much about chronic illnesses. And for this reason, some people don’t know about these illnesses. When writing about non-communicable illnesses, you can settle for human genetic disease topics or even research topics for sickle cell disease. Here are some of the topics about non-communicable diseases that you can write about.
- The risk of breast cancer after childbirth
- Postpartum PTSD- Effective preventative measures
- Experiences of females suffering from cardiac disease during pregnancy- A systematic review
- Husbands attendance and knowledge of wives’ postpartum care in rural areas
- Postpartum depression screening by perinatal nurses in hospitals
- Gestational diabetes mellitus screening from the rural perspective
- Maternal mortality- How to help cardiac and pregnant patients
- Sex differences in cardio metabolic disorders and major depression- Effect of immune exposures and prenatal stress
- Determinants and prevalence of anxiety and antepartum depressive symptoms in fathers and expectant mothers- Outcomes from perinatal psychiatric morbidity
- Evaluating the effect of community health workers on non-communicable diseases, tuberculosis, malnutrition, antenatal care, and family planning
- History of women with postpartum affective disorder and the risk of future pregnancies recurrence
- New self-care guide package and its effect on neonatal and maternal results in gestational diabetes
- Depressive symptoms and life events in pregnant women- Moderating the resilience role and social support
- Gestational diabetes and ethnic disparities
- Pregnancy and diabetes- Opportunities and risks
- Cardiovascular disease maternal death reduction- A pragmatic investigation
- Meta-analysis and systematic review of gestational diabetes mellitus diagnosis with a two-step or one-step associations and approaches with negative pregnancy outcomes
- Gestational diabetes mellitus treatment in women- A Cochrane systematic overview
- Research in non-communicable diseases in Africa- A strategic investment
- How to finance the national response to non-communicable diseases
Whether you opt to write about research paper topics in Huntington’s disease or non-communicable liver disease topics, you have to engage in extensive research to come up with a brilliant paper. We have more health research topics for you, so don’t hesitate to check them. Therefore, select an idea you will be comfortable researching and writing about. That way, you will avoid enduring a boring process of investing your topic and writing the paper. If you want to hire someone to help you with your assignment, just c ontact us with a “ do my research paper now ” request and we’ll get your papers done.

You are here
Nih research matters.
April 23, 2024
Research in Context: Treating depression
Finding better approaches.
While effective treatments for major depression are available, there is still room for improvement. This special Research in Context feature explores the development of more effective ways to treat depression, including personalized treatment approaches and both old and new drugs.

Everyone has a bad day sometimes. People experience various types of stress in the course of everyday life. These stressors can cause sadness, anxiety, hopelessness, frustration, or guilt. You may not enjoy the activities you usually do. These feelings tend to be only temporary. Once circumstances change, and the source of stress goes away, your mood usually improves. But sometimes, these feelings don’t go away. When these feelings stick around for at least two weeks and interfere with your daily activities, it’s called major depression, or clinical depression.
In 2021, 8.3% of U.S. adults experienced major depression. That’s about 21 million people. Among adolescents, the prevalence was much greater—more than 20%. Major depression can bring decreased energy, difficulty thinking straight, sleep problems, loss of appetite, and even physical pain. People with major depression may become unable to meet their responsibilities at work or home. Depression can also lead people to use alcohol or drugs or engage in high-risk activities. In the most extreme cases, depression can drive people to self-harm or even suicide.
The good news is that effective treatments are available. But current treatments have limitations. That’s why NIH-funded researchers have been working to develop more effective ways to treat depression. These include finding ways to predict whether certain treatments will help a given patient. They're also trying to develop more effective drugs or, in some cases, find new uses for existing drugs.
Finding the right treatments
The most common treatments for depression include psychotherapy, medications, or a combination. Mild depression may be treated with psychotherapy. Moderate to severe depression often requires the addition of medication.
Several types of psychotherapy have been shown to help relieve depression symptoms. For example, cognitive behavioral therapy helps people to recognize harmful ways of thinking and teaches them how to change these. Some researchers are working to develop new therapies to enhance people’s positive emotions. But good psychotherapy can be hard to access due to the cost, scheduling difficulties, or lack of available providers. The recent growth of telehealth services for mental health has improved access in some cases.
There are many antidepressant drugs on the market. Different drugs will work best on different patients. But it can be challenging to predict which drugs will work for a given patient. And it can take anywhere from 6 to 12 weeks to know whether a drug is working. Finding an effective drug can involve a long period of trial and error, with no guarantee of results.
If depression doesn’t improve with psychotherapy or medications, brain stimulation therapies could be used. Electroconvulsive therapy, or ECT, uses electrodes to send electric current into the brain. A newer technique, transcranial magnetic stimulation (TMS), stimulates the brain using magnetic fields. These treatments must be administered by specially trained health professionals.
“A lot of patients, they kind of muddle along, treatment after treatment, with little idea whether something’s going to work,” says psychiatric researcher Dr. Amit Etkin.
One reason it’s difficult to know which antidepressant medications will work is that there are likely different biological mechanisms that can cause depression. Two people with similar symptoms may both be diagnosed with depression, but the causes of their symptoms could be different. As NIH depression researcher Dr. Carlos Zarate explains, “we believe that there’s not one depression, but hundreds of depressions.”
Depression may be due to many factors. Genetics can put certain people at risk for depression. Stressful situations, physical health conditions, and medications may contribute. And depression can also be part of a more complicated mental disorder, such as bipolar disorder. All of these can affect which treatment would be best to use.
Etkin has been developing methods to distinguish patients with different types of depression based on measurable biological features, or biomarkers. The idea is that different types of patients would respond differently to various treatments. Etkin calls this approach “precision psychiatry.”
One such type of biomarker is electrical activity in the brain. A technique called electroencephalography, or EEG, measures electrical activity using electrodes placed on the scalp. When Etkin was at Stanford University, he led a research team that developed a machine-learning algorithm to predict treatment response based on EEG signals. The team applied the algorithm to data from a clinical trial of the antidepressant sertraline (Zoloft) involving more than 300 people.

EEG data for the participants were collected at the outset. Participants were then randomly assigned to take either sertraline or an inactive placebo for eight weeks. The team found a specific set of signals that predicted the participants’ responses to sertraline. The same neural “signature” also predicted which patients with depression responded to medication in a separate group.
Etkin’s team also examined this neural signature in a set of patients who were treated with TMS and psychotherapy. People who were predicted to respond less to sertraline had a greater response to the TMS/psychotherapy combination.
Etkin continues to develop methods for personalized depression treatment through his company, Alto Neuroscience. He notes that EEG has the advantage of being low-cost and accessible; data can even be collected in a patient’s home. That’s important for being able to get personalized treatments to the large number of people they could help. He’s also working on developing antidepressant drugs targeted to specific EEG profiles. Candidate drugs are in clinical trials now.
“It’s not like a pie-in-the-sky future thing, 20-30 years from now,” Etkin explains. “This is something that could be in people's hands within the next five years.”
New tricks for old drugs
While some researchers focus on matching patients with their optimal treatments, others aim to find treatments that can work for many different patients. It turns out that some drugs we’ve known about for decades might be very effective antidepressants, but we didn’t recognize their antidepressant properties until recently.
One such drug is ketamine. Ketamine has been used as an anesthetic for more than 50 years. Around the turn of this century, researchers started to discover its potential as an antidepressant. Zarate and others have found that, unlike traditional antidepressants that can take weeks to take effect, ketamine can improve depression in as little as one day. And a single dose can have an effect for a week or more. In 2019, the FDA approved a form of ketamine for treating depression that is resistant to other treatments.
But ketamine has drawbacks of its own. It’s a dissociative drug, meaning that it can make people feel disconnected from their body and environment. It also has the potential for addiction and misuse. For these reasons, it’s a controlled substance and can only be administered in a doctor’s office or clinic.
Another class of drugs being studied as possible antidepressants are psychedelics. These include lysergic acid diethylamide (LSD) and psilocybin, the active ingredient in magic mushrooms. These drugs can temporarily alter a person’s mood, thoughts, and perceptions of reality. Some have historically been used for religious rituals, but they are also used recreationally.
In clinical studies, psychedelics are typically administered in combination with psychotherapy. This includes several preparatory sessions with a therapist in the weeks before getting the drug, and several sessions in the weeks following to help people process their experiences. The drugs are administered in a controlled setting.
Dr. Stephen Ross, co-director of the New York University Langone Health Center for Psychedelic Medicine, describes a typical session: “It takes place in a living room-like setting. The person is prepared, and they state their intention. They take the drug, they lie supine, they put on eye shades and preselected music, and two therapists monitor them.” Sessions last for as long as the acute effects of the drug last, which is typically several hours. This is a healthcare-intensive intervention given the time and personnel needed.
In 2016, Ross led a clinical trial examining whether psilocybin-assisted therapy could reduce depression and anxiety in people with cancer. According to Ross, as many as 40% of people with cancer have clinically significant anxiety and depression. The study showed that a single psilocybin session led to substantial reductions in anxiety and depression compared with a placebo. These reductions were evident as soon as one day after psilocybin administration. Six months later, 60-80% of participants still had reduced depression and anxiety.
Psychedelic drugs frequently trigger mystical experiences in the people who take them. “People can feel a sense…that their consciousness is part of a greater consciousness or that all energy is one,” Ross explains. “People can have an experience that for them feels more ‘real’ than regular reality. They can feel transported to a different dimension of reality.”
About three out of four participants in Ross’s study said it was among the most meaningful experiences of their lives. And the degree of mystical experience correlated with the drug’s therapeutic effect. A long-term follow-up study found that the effects of the treatment continued more than four years later.
If these results seem too good to be true, Ross is quick to point out that it was a small study, with only 29 participants, although similar studies from other groups have yielded similar results. Psychedelics haven’t yet been shown to be effective in a large, controlled clinical trial. Ross is now conducting a trial with 200 people to see if the results of his earlier study pan out in this larger group. For now, though, psychedelics remain experimental drugs—approved for testing, but not for routine medical use.
Unlike ketamine, psychedelics aren’t considered addictive. But they, too, carry risks, which certain conditions may increase. Psychedelics can cause cardiovascular complications. They can cause psychosis in people who are predisposed to it. In uncontrolled settings, they have the risk of causing anxiety, confusion, and paranoia—a so-called “bad trip”—that can lead the person taking the drug to harm themself or others. This is why psychedelic-assisted therapy takes place in such tightly controlled settings. That increases the cost and complexity of the therapy, which may prevent many people from having access to it.
Better, safer drugs
Despite the promise of ketamine or psychedelics, their drawbacks have led some researchers to look for drugs that work like them but with fewer side effects.
Depression is thought to be caused by the loss of connections between nerve cells, or neurons, in certain regions of the brain. Ketamine and psychedelics both promote the brain’s ability to repair these connections, a quality called plasticity. If we could understand how these drugs encourage plasticity, we might be able to design drugs that can do so without the side effects.

Dr. David Olson at the University of California, Davis studies how psychedelics work at the cellular and molecular levels. The drugs appear to promote plasticity by binding to a receptor in cells called the 5-hydroxytryptamine 2A receptor (5-HT2AR). But many other compounds also bind 5-HT2AR without promoting plasticity. In a recent NIH-funded study, Olson showed that 5-HT2AR can be found both inside and on the surface of the cell. Only compounds that bound to the receptor inside the cells promoted plasticity. This suggests that a drug has to be able to get into the cell to promote plasticity.
Moreover, not all drugs that bind 5-HT2AR have psychedelic effects. Olson’s team has developed a molecular sensor, called psychLight, that can identify which compounds that bind 5-HT2AR have psychedelic effects. Using psychLight, they identified compounds that are not psychedelic but still have rapid and long-lasting antidepressant effects in animal models. He’s founded a company, Delix Therapeutics, to further develop drugs that promote plasticity.
Meanwhile, Zarate and his colleagues have been investigating a compound related to ketamine called hydroxynorketamine (HNK). Ketamine is converted to HNK in the body, and this process appears to be required for ketamine’s antidepressant effects. Administering HNK directly produced antidepressant-like effects in mice. At the same time, it did not cause the dissociative side effects and addiction caused by ketamine. Zarate’s team has already completed phase I trials of HNK in people showing that it’s safe. Phase II trials to find out whether it’s effective are scheduled to begin soon.
“What [ketamine and psychedelics] are doing for the field is they’re helping us realize that it is possible to move toward a repair model versus a symptom mitigation model,” Olson says. Unlike existing antidepressants, which just relieve the symptoms of depression, these drugs appear to fix the underlying causes. That’s likely why they work faster and produce longer-lasting effects. This research is bringing us closer to having safer antidepressants that only need to be taken once in a while, instead of every day.
—by Brian Doctrow, Ph.D.
Related Links
- How Psychedelic Drugs May Help with Depression
- Biosensor Advances Drug Discovery
- Neural Signature Predicts Antidepressant Response
- How Ketamine Relieves Symptoms of Depression
- Protein Structure Reveals How LSD Affects the Brain
- Predicting The Usefulness of Antidepressants
- Depression Screening and Treatment in Adults
- Serotonin Transporter Structure Revealed
- Placebo Effect in Depression Treatment
- When Sadness Lingers: Understanding and Treating Depression
- Psychedelic and Dissociative Drugs
References: An electroencephalographic signature predicts antidepressant response in major depression. Wu W, Zhang Y, Jiang J, Lucas MV, Fonzo GA, Rolle CE, Cooper C, Chin-Fatt C, Krepel N, Cornelssen CA, Wright R, Toll RT, Trivedi HM, Monuszko K, Caudle TL, Sarhadi K, Jha MK, Trombello JM, Deckersbach T, Adams P, McGrath PJ, Weissman MM, Fava M, Pizzagalli DA, Arns M, Trivedi MH, Etkin A. Nat Biotechnol. 2020 Feb 10. doi: 10.1038/s41587-019-0397-3. Epub 2020 Feb 10. PMID: 32042166. Rapid and sustained symptom reduction following psilocybin treatment for anxiety and depression in patients with life-threatening cancer: a randomized controlled trial. Ross S, Bossis A, Guss J, Agin-Liebes G, Malone T, Cohen B, Mennenga SE, Belser A, Kalliontzi K, Babb J, Su Z, Corby P, Schmidt BL. J Psychopharmacol . 2016 Dec;30(12):1165-1180. doi: 10.1177/0269881116675512. PMID: 27909164. Long-term follow-up of psilocybin-assisted psychotherapy for psychiatric and existential distress in patients with life-threatening cancer. Agin-Liebes GI, Malone T, Yalch MM, Mennenga SE, Ponté KL, Guss J, Bossis AP, Grigsby J, Fischer S, Ross S. J Psychopharmacol . 2020 Feb;34(2):155-166. doi: 10.1177/0269881119897615. Epub 2020 Jan 9. PMID: 31916890. Psychedelics promote neuroplasticity through the activation of intracellular 5-HT2A receptors. Vargas MV, Dunlap LE, Dong C, Carter SJ, Tombari RJ, Jami SA, Cameron LP, Patel SD, Hennessey JJ, Saeger HN, McCorvy JD, Gray JA, Tian L, Olson DE. Science . 2023 Feb 17;379(6633):700-706. doi: 10.1126/science.adf0435. Epub 2023 Feb 16. PMID: 36795823. Psychedelic-inspired drug discovery using an engineered biosensor. Dong C, Ly C, Dunlap LE, Vargas MV, Sun J, Hwang IW, Azinfar A, Oh WC, Wetsel WC, Olson DE, Tian L. Cell . 2021 Apr 8: S0092-8674(21)00374-3. doi: 10.1016/j.cell.2021.03.043. Epub 2021 Apr 28. PMID: 33915107. NMDAR inhibition-independent antidepressant actions of ketamine metabolites. Zanos P, Moaddel R, Morris PJ, Georgiou P, Fischell J, Elmer GI, Alkondon M, Yuan P, Pribut HJ, Singh NS, Dossou KS, Fang Y, Huang XP, Mayo CL, Wainer IW, Albuquerque EX, Thompson SM, Thomas CJ, Zarate CA Jr, Gould TD. Nature . 2016 May 26;533(7604):481-6. doi: 10.1038/nature17998. Epub 2016 May 4. PMID: 27144355.
Connect with Us
- More Social Media from NIH
- Open access
- Published: 18 November 2021
Scientific evidence based rare disease research discovery with research funding data in knowledge graph
- Qian Zhu ORCID: orcid.org/0000-0002-4858-6333 1 ,
- Ðắc-Trung Nguyễn 1 ,
- Timothy Sheils 1 ,
- Gioconda Alyea 2 ,
- Eric Sid 3 ,
- Yanji Xu 3 ,
- James Dickens 3 ,
- Ewy A. Mathé 1 &
- Anne Pariser 3
Orphanet Journal of Rare Diseases volume 16 , Article number: 483 ( 2021 ) Cite this article
3288 Accesses
7 Citations
Metrics details
Limited knowledge and unclear underlying biology of many rare diseases pose significant challenges to patients, clinicians, and scientists. To address these challenges, there is an urgent need to inspire and encourage scientists to propose and pursue innovative research studies that aim to uncover the genetic and molecular causes of more rare diseases and ultimately to identify effective therapeutic solutions. A clear understanding of current research efforts, knowledge/research gaps, and funding patterns as scientific evidence is crucial to systematically accelerate the pace of research discovery in rare diseases, which is an overarching goal of this study.
To semantically represent NIH funding data for rare diseases and advance its use of effectively promoting rare disease research, we identified NIH funded projects for rare diseases by mapping GARD diseases to the project based on project titles; subsequently we presented and managed those identified projects in a knowledge graph using Neo4j software, hosted at NCATS, based on a pre-defined data model that captures semantics among the data. With this developed knowledge graph, we were able to perform several case studies to demonstrate scientific evidence generation for supporting rare disease research discovery.
Of 5001 rare diseases belonging to 32 distinct disease categories, we identified 1294 diseases that are mapped to 45,647 distinct, NIH-funded projects obtained from the NIH ExPORTER by implementing semantic annotation of project titles. To capture semantic relationships presenting amongst mapped research funding data, we defined a data model comprised of seven primary classes and corresponding object and data properties. A Neo4j knowledge graph based on this predefined data model has been developed, and we performed multiple case studies over this knowledge graph to demonstrate its use in directing and promoting rare disease research.
We developed an integrative knowledge graph with rare disease funding data and demonstrated its use as a source from where we can effectively identify and generate scientific evidence to support rare disease research. With the success of this preliminary study, we plan to implement advanced computational approaches for analyzing more funding related data, e.g., project abstracts and PubMed article abstracts, and linking to other types of biomedical data to perform more sophisticated research gap analysis and identify opportunities for future research in rare diseases.
A rare disease is defined as any disease that affects fewer than 200,000 individuals in the United States. There are an estimated 25–30 million Americans that are affected by one of approximately 7000 different rare diseases, most of which are poorly understood with unclear underlying biological mechanisms. This knowledge gap leads to challenges for patients, clinicians, and investigators. Patients affected by a rare disease experience delays in diagnosis, as well as a lack of available treatments, clinicians often have limited clinical knowledge and experience impedes their clinical decision making, and investigators struggle with limited patient data and sparse funding for research across most rare diseases [ 1 ]. To help address these challenges, we proposed a detailed analysis of research funding data to (1) enhance understanding of the current funding situation and potential funding opportunities in rare diseases, and (2) identify gaps among current research activities in rare diseases that may be primed for new research.
Compared to common diseases that are more highly prevalent in the population, such as depression or heart disease, research funding is often scarce for rare diseases, in part due to the relatively small number of people affected, and lower prioritization of funding based on the perceived burden of the disease [ 2 ]. In fiscal year 2019, the National Institutes of Health (NIH) were appropriated $39 billion [ 3 ], of which only $38 million (0.1%) was awarded to study a wide range of rare diseases [ 4 ]. Similarly, in the UK, less than 1% of the annual funding budget from three out of the top four UK funders were directed towards rare disease research [ 5 ]. A lack of funding results in less research aiming to understand disease etiology, identify biomarkers for disease diagnosis, develop of novel medications and associated clinical trials, and ultimately, absent treatment options. To solicit and attract more funding for innovative research in rare diseases, there is an urgent need to better understand and assess the current funding situation/trend and address gaps found to persist from retrospectively tracing funding history.
To review the funding landscape, Stehr et al. examined funding circumstances for Batten Disease, a group of rare nervous system disorders, by extracting funding information from publications. Interestingly they discovered 193 funding agencies had supported Batten Disease research to date, which might encourage researchers to continue their pursuits and expand their studies, moving key findings from discovery to application phases [ 6 ]. Franceschi et al. led a study to characterize recent NIH funding for diagnostic radiology departments at US medical schools [ 7 ]. To inform decisions on research direction, Ma et al. examined over 43,000 scientific projects funded over the past three decades and established collaboration networks that revealed major ramifications on future research strategy and government policy [ 8 ]. Packalen et al. performed an analysis on a comprehensive corpus of published biomedical research articles, and found that edge science framed with novel basic science ideas is more often funded by the NIH than less novel science [ 9 ]. These studies either limited their review of the funding landscape to a few specific diseases or diagnostic protocols, or assessed research direction globally. In our study, we aimed to develop an approach to systematically overview funding trend across different disease categories or individual diseases, and identify research gaps globally or locally (i.e., for individual disease category or disease) to further support rare disease research.
To overcome the challenge of handling large amounts of data accumulated given scientific advancements, knowledge graphs have attracted a lot of interest in the biomedical domain, as they can be leveraged to semantically represent relationships among large-scale data [ 10 ]. Ding, et al. constructed a PubMed knowledge graph (PKG) by extracting bio-entities from 29 million PubMed abstracts with integrated funding data through the NIH ExPORTER, in order to measure scholarly impact, knowledge usage and transfer, and profile authors and organizations based on their connections with bio-entities [ 11 ]. In our previous work, we developed an integrative knowledge graph in Neo4j [ 12 ], named NCATS GARD Knowledge Graph (NGKG) that contained a large volume of biomedical and research data pertinent to rare diseases [ 13 ]. Inspired by these published studies, we proposed to aggregate and represent funding data for rare diseases in a semantic manner as a knowledge graph. While the PKG incorporates publications and funding to gain insights and approaches to connect researchers with common research interests, our primary goal is to not only assess the funding landscape of rare diseases, but also identify research status and knowledge gaps, which can be applied to promote novel research for rare diseases.
Rare disease resources
In this study, we incorporated rare disease information from the Genetic and Rare Diseases (GARD) [ 14 ] and Monarch Disease Ontology (MONDO) [ 15 ]. GARD is a public health information center managed by the Office of Rare Diseases Research (ORDR) within the National Center for Advancing Translational Sciences (NCATS), and retains curated disease information for about 7000 rare diseases. MONDO is a semi-automatically constructed ontology that merges multiple disease resources to yield a single coherent merged ontology [ 15 ]. We accessed GARD and MONDO from our previously developed NCATS GARD Knowledge Graph (NGKG) in Neo4j [ 13 , 16 ].
NIH funding resource
Research Portfolio Online Reporting Tools Expenditures and Results (RePORTER) is a key component of the NIH’s “open government” initiative to provide more transparency into NIH activities, including information on NIH expenditures and the results of NIH supported research [ 17 ]. ExPORTER provides bulk administrative data found in RePORTER to the public for detailed analyses or to load into their own data systems [ 18 ]. ExPORTER provides downloadable versions of the data accessed through the RePORTER interface, and includes information about projects, publications, patents, and clinical studies. In this study, we downloaded and cleaned the funded projects and associated publications from ExPORTER, and stored the data in a MySQL database, from where we obtained data for the analysis described in this study.
Rare disease data preparation
We extracted 6305 GARD rare diseases from the NGKG in Neo4j [ 13 , 16 ]. In order to adopt disease categories from MONDO to organize these extracted rare diseases, we only included 5001 GARD rare diseases that have one-to-one exact mapping to MONDO based on one MONDO property, “MONDO:equivalentTo”. As a proof-of-concept with minimized manual validation, we did not include one-to-many, many-to-many or any other partial mappings between GARD and MONDO concepts, which will be included in a future study.
To enable review and analysis of research funding by disease categories, we mapped GARD diseases to MONDO disease categories. MONDO contains three main branches in its disease classification tree, namely, “Disease Characteristic”, “Disease or Disorder” and “Disease Susceptibility”. In this study, we focused on the branch of “Disease or Disorder” (MONDO: 0000001) in MONDO obo file [ 19 ], from where we extracted 32 root disease categories, including congenital abnormality, acute disease, disorder involving pain, serpinopathy, psychiatric disorder, visceral myopathy, and post-infectious disorder, etc. (A complete list of 32 root disease categories can be found in Additional file 1 ) We mapped those 5001 GARD diseases to the 32 root categories accordingly by iteratively searching the MONDO disease hieratical tree. It is worthy to note that most GARD diseases map to more than one MONDO disease categories.
NIH funded project identification for rare diseases
NIH ExPORTER provides detailed information about funded projects, including project titles and project abstracts in free text. We assumed that if the disease name is mentioned in the project title, it is likely that the project was proposed to conduct research investigation on this disease. Hence, we proposed to map GARD disease names to project titles, to identify a list of funded projects for each individual GARD disease via two steps as described below. Before mapping, we excluded projects with invalid project titles, such as, “13.358”, “CFDA NO. 13-299”.
Mapping based on name match
We executed ‘LIKE’ SQL operator as exact string match to identify projects with disease names mentioned in the project titles from the MySQL database, which stores the cleaned funding data. To avoid any mis-mappings, we applied not only full disease names but also alternative disease names in the ‘LIKE’ operator. Since abbreviations occurring in disease names and/or synonyms might cause incorrect mappings, disease names and synonyms with less than 4 characters were excluded for mapping.
Mapping based on semantic annotation.
As a complementary step, we semantically annotated project titles in free text by using MetaMap annotator [ 20 ], and then mapped GARD diseases to those generated annotations. MetaMap annotator produces a list of annotations in the Unified Medical Language System (UMLS), including UMLS semantic types, its preferred names, etc. Figure 1 shows a snapshot of annotation results generated for a project entitled “The Natural History of Mucolipidosis Type IV”. To avoid any incorrect mappings, we excluded those annotated concepts with less than 4 characters for further analysis, for example: “RNS (UMLS: C1850106)” as one annotation for the project title of “HAMPTON INSTITUTE'S CONTINUING EDUCATION PROGRAM FOR RNS”.

Annotation results generated by MetaMap (The fields in bold were extracted and applied to map to GARD diseases, “C0238386” is UMLS identifier, “Mucolipidosis Type IV” is UMLS preferred name, “[dsyn]” is one UMLS semantic type, “Disease or Syndrome”)
In order to establish the mappings between funded projects and GARD diseases, we mapped annotations generated from each project title to GARD diseases based on UMLS mappings since MetaMap output is in the UMLS, as shown in Fig. 1 . We retrieved mappings between GARD diseases and the UMLS via two steps. First, we obtained the UMLS mappings that were curated by GARD. Next, we obtained the UMLS mapping from MONDO for the GARD disease if the GARD disease concept was exactly matched to the MONDO concept and this MONDO concept had an external mapping to the UMLS. For instance, Bloom syndrome (GARD:0000915) is exactly matched to one MONDO concept of Bloom syndrome (MONDO:0008876) that is mapped to one UMLS concept (UMLS:C0005859). Thus, with UMLS:C0005859, we were able to map this GARD disease to one project entitled “BLOOM'S SYNDROME--DNA LIGASE AND IMMUNODEFICIENCY” with one annotation of Bloom Syndrome (UMLS:C0005859).
Once we established the connections between GARD diseases and funded projects through the above steps, we designed a data model to semantically capture and represent different types of data extracted from those funded projects and their associated data, such as, publications or principal investigators.
Primary class definition
We defined seven primary classes, namely, Disease Category, Disease, Funded Project, Funding Agent, Principal Investigator, Publication, and Journal. These classes capture a full spectrum of information present in NIH funding data and enable linkages to other different types of data for directing more sophisticated research on rare diseases, which will be described in the “ Discussion ” section.
Object property definition
To capture semantic relationships among those primary classes, we defined object properties as shown in Table 1 .
Data property definition
We defined a list of data properties shown in Table 2 to link data values for each individual concept.
NIH funding knowledge graph
Based on the data model we described above, we loaded the mapped funding data to a knowledge graph hosted in Neo4j. To be specific, different types of data have been loaded and represented with those seven primary classes as nodes accordingly; object properties were applied to establish semantic connections between different nodes as edges, and data properties were attached to corresponding nodes as node properties. The knowledge graph is publicly assessable without login requirement at http://grants4rd.ncats.io:7474/browser/ .
Results of rare disease data preparation
A total of 5001 unique GARD rare diseases were categorized based on the MONDO disease classes. Table 3 shows the categorization results. Only 799 GARD diseases belonged to a single MONDO category, while most GARD diseases were mapped to multiple MONDO disease categories. For example, GARD:0006735 (Hypophosphatemic rickets) is mapped to three different MONDO disease categories: MONDO:0003847 (Mendelian disease), MONDO:0003900 (connective tissue disease), and MONDO:0021199 (disease by anatomical system). There are 52 GARD diseases that were not grouped into any of MONDO disease categories, because they were either mapped to obsolete MONDO diseases or another two MONDO disease category branches, “Disease Characteristic” and “Disease Susceptibility”, which were excluded from this study.
Results of NIH funding data mapping
Results of nih funding data retrieval.
We downloaded the funding data with funding year spanning from 1985 to 2019 from NIH ExPORTER [ 18 ]. A total of 2,457,303 distinct applications with 654,347 unique project titles, 886,895 unique project abstracts, and 2,555,300 publications are cleaned and stored in a MySQL database.
Results of NIH funding data mapped to GARD
Two types of mapping results have been generated via exact name (i.e., String) match and MetaMap annotations.
Disease name mapping results
Both GARD disease names and synonyms have been applied to map project titles. 1104 GARD diseases were mapped to 21,027 project titles, which correspond to 63,692 NIH funded applications. Since one project can be funded for multiple years as multiple applications with the same project title, the number of mapped applications is larger than the number of project titles.
MetaMap annotation results
652,975 unique project titles were annotated by the MetaMap annotator and 5,039,735 annotations were generated. To map GARD diseases to those annotations based on UMLS mappings, we first retrieved UMLS mappings for GARD diseases from GARD and MONDO. Specifically, 3468 GARD diseases with UMLS mappings were extracted from GARD, and out of 15,629 MONDO concepts with UMLS mappings, 3980 MONDO entries were mapped to 4032 GARD diseases and corresponding UMLS mappings, which were assigned to those GARD diseases. Together, 1146 GARD diseases were mapped to 13,695 project titles via UMLS mappings.
By merging mapping results from the above two steps, 1294 GARD diseases were successfully mapped to 72,577 funded applications, which corresponds to 45,647 distinct projects.
Statistical results of NIH rare disease funding data in the Neo4j knowledge graph
Summarized statistical results of individual concepts belonging to each primary class are shown in Fig. 2 .

Statistics of rare disease funding Neo4j knowledge graph
Case studies
To demonstrate the use of this integrated knowledge graph with rare disease funding data, we performed two types of case studies, (1) funding landscape assessments for an overview of the current funding landscape; (2) evidence-based research opportunity identification for supporting research in rare diseases. Cypher Queries have been composed and executed to perform case studies described in this section, and more details about those Cypher Queries are included in the Additional file 2 .
Current funding landscape
To review NIH funding scenario in rare diseases, we composed several queries using Cypher, which is Neo4j’s graph query language that allows users to store and retrieve data from the graph database [ 21 ], to search against funding data in our Neo4j. Cypher Query 1 was constructed to access funding circumstances by disease categories and the result is listed in Table 4 . Since one disease might be grouped into multiple disease categories, duplicates occurred when the number of GARD diseases, number of projects and total cost by each category were summed. Regardless, the numbers listed in Table 4 consistently reflect funding priorities with the consideration of disease burden applied by NIH. In addition, we retrieved funding amounts in the last twenty years for the top five most funded disease category, which is shown in Fig. 3 . It is worthy to note that no funding cost data is available before the year of 2000 in our downloaded data. From Fig. 3 , besides infectious diseases, big jumps were present due to the Ebola and Zika outbreaks that occurred during that time frame, the increasing funding trends are observed for other categories.

Funding trend by year for the top five most funded disease categories
Cypher Query 1
MATCH p = (n:Project)<-[:isInvestigatedBy]-(d:Disease)-[:isClassOf]-(c:DiseaseCategory) RETURN c.name AS Disease_Category, COUNT(DISTINCT d.gard_id) AS NumOfGARD, COUNT(n.application_id) AS NumOfProjects, SUM(TOINTEGER(n.total_cost)) AS Total_Funding_Amount ORDER BY Total_Funding_Amount DESC
We also evaluated the top 10 funded individual diseases (via Cypher Query 2). The top four funded diseases shown in Table 5 are infectious diseases. Poliomyelitis is considered a global public health emergency and the U.S. is a partner of the Global Polio Eradication Initiative [ 22 ]. Particularly, the CDC and the U.S. Agency for International Development (USAID) work to eradicate polio and have signed onto the Polio Endgame Strategy 2019–2023 [ 23 ]. About half of the world population is at risk for Malaria and the U.S. is the largest donor to the Global Fund to Fight AIDS, Tuberculosis, and Malaria (Global Fund) [ 24 ]. A large amount of research funds are being distributed on research for effective vaccines for Anthrax and Measles. In comparison to other rare diseases, the rest of diseases listed in Table 5 , such as sickle cell disease with about 100,000 affected people in the US, both of cystic fibrosis and Huntington disease with more than 30,000 affected people in the US, are diseases that are closer to finding a cure or effective treatment, in part because they receive more research funding.
Cyper Query 2
MATCH p = (d:Disease)-[:isInvestigatedBy]-(n:Project) RETURN d.gard_id AS GARD_ID, d.name AS GARD_Name, SUM(toInteger(n.total_cost)) AS Total_Funding_Amount ORDER BY total_cost DESC LIMIT 10
Evidence-based rare disease research discovery
We aggregated funded projects and their publications into an integrated knowledge graph in Neo4j, which offers opportunities to programmatically support new research for rare diseases.
Research landscape assessment
Funded projects along with their publications show snapshots of their research goals and outcomes, which provides an opportunity to systematically assess the current research status and gaps, and consequently direct future areas for investigation. We enumerated two types of assessment for Neuronal ceroid lipofuscinosis (GARD: 0010739) and Duchenne Muscular Dystrophy (GARD:0007922) as examples.
Research status assessment for neuronal ceroid lipofuscinosis (NCL)
NCLs are classified by their causal gene of CLN (ceroid lipofuscinosis, neuronal), which is given a different number designation as its subtype. Signs and symptoms range in severity and progress at different rates given different gene mutations. The disorders generally include a combination of vision loss, epilepsy, and dementia. Some forms of the NCLs are: CLN1 disease, infantile onset; CLN2 disease, later-onset and so on [ 25 ]. Scientific investigations have been performed for each subtype of NCL (via Cypher Query 3). By manually examining the funded projects and their published studies for NCL, we grouped them based on their studied NCL forms (Fig. 4 ). Noticeably, these funded projects aim to better understand the molecular mechanism of NCL and discover therapeutic solutions. In particular, several subtypes (CLN2, CLN3 and CLN6) of NCL are more extensively studied than others. There is an Food and Drug Administration (FDA) approved enzyme replacement therapy for CLN2 disease (TTP1 deficiency) called cerliponase alfa (Brineura®) that has been shown to slow or halt the progression of symptoms [ 26 ]. With the exception of CLN2, which is highlighted as “CLN2” in Fig. 4 , there are no approved treatments that can slow or stop disease progression for other forms of NCL disorder. As NCL affects the brain and nervous system, treatments must reach the brain to be effective, but getting the proper enzyme to cross the blood brain barrier can be difficult. For this reason, enzyme replacement therapy can only be used in NCL forms where the affected enzyme is soluble. This includes the subtypes known as CLN1, CLN2, CLN5 and CLN10 [ 27 ]. Thus, learning from the success of Brineura for CLN2 enhances the necessary scientific evidence and understanding of what existing research has been performed in other forms of NCL, and may better inform the direction of further research investigation on NCL.

Research landscape of Neuronal ceroid lipofuscinosis (Light blue nodes denote diseases, orange nodes denote funded projects, magenta nodes denote publications, Dark blue nodes denote principal investigators. CLN1, CLN2, CLN3, CLN4, CLN6 and ACLN are different forms of NCL)
Cypher Query 3
MATCH p = (d:Disease)-[:isInvestigatedBy]->(n:Project)<-[:hasFundedProjectOf]-(m:PrincipalInvestigator) WHERE d.gard_id = 'GARD:0010739' RETURN p
Research study clustering for Duchenne Muscular Dystrophy
Publications introduce novel approaches and/or findings that were proposed and generated from the funded projects. For example, a project entitled “LOCALIZATION OF X-LINKED HYPOPHOSPHATEMIC RICKETS GENE” (APPLICATION ID = “3087091”), has reported two publications, “Mutational analysis and genotype-phenotype correlation of the PHEX gene in X-linked hypophosphatemic rickets.” (PMID: 11502829) and “Mutational analysis of the PEX gene in patients with X-linked hypophosphatemic rickets.” (PMID: 9106524) These two publications specifically reported their investigation on genes for X-linked hypophosphatemic rickets. For a given disease, we clustered research studies by a project or a list of projects with similar research topics, which allows tracking research trajectory, identifying research gaps, and preparing necessary training data for future study. In this case study, we executed Cypher Query 4 to cluster publications associated with the funded projects for Duchenne Muscular Dystrophy (GARD:0006291), a lethal muscle wasting disease caused by the lack of dystrophin, which eventually leads to apoptosis of muscle cells and impaired muscle contractility. Four projects, along with their publications, are shown in Fig. 5 . Based on the project titles shown in gray boxes in Fig. 5 , we deduced that their objectives are all tied to breaching the major barriers to successful therapeutic solutions for Duchenne Muscular Dystrophy respectively via iPSCs, Cas9 and Cx43.

Publications clustered by funded projects for Duchenne Muscular Dystrophy (Blue nodes denote diseases, orange nodes denote funded projects, magenta nodes denote publications. Project titles are shown in the gray boxes)
Cypher Query 4
MATCH p =(d:Disease)-[:isInvestigatedBy]-(n:Project)-[:hasPublication]-(m:Publication) WHERE d.gard_id = 'GARD:0006291' RETURN p
Identify new research opportunities
In this case study, we proposed to gain research insights systematically by analyzing project titles. For instance, given one project entitled “USE OF LEUPROLIDE ACETATE FOR TREATMENT OF PRECOCIOUS PUBERTY”, we know this project was studying leuprolide acetate (Drug) for precocious puberty [ 28 ]. With the disease annotations generated for project titles (described in the “ Identify new research opportunities ” section), we were able to identify potential disease associations via projects, and furthermore to identify new avenues for research. Fig. 6 demonstrates an example of looking for potentially relevant diseases to Measles (GARD:0003434) via Cypher Query 5. Obviously multiple rare infectious diseases, including Poliomyelitis, Rubella, Congenital rubella, and Malaria are grouped together, and interestingly Measles and Glioblastoma is linked via one project entitled “Measles Virotherapy for Glioblastoma Multiforme”, highlighted in the red circle shown in Fig. 6 . According to one recently published review paper written by Zhang et al. [ 29 ], “advances and potential pitfalls of oncolytic viruses expressing immunomodulatory transgene therapy for malignant gliomas”, the authors emphasized that the therapeutic efficacy of oncolytic viruses alone is limited, which might motivate novel research to better understand and assess the therapeutic efficacy. Five related publications produced by this project provide additional information to direct future investigation.

Identifying possible research opportunities for Measles via funded projects (Orange nodes denote funded projects, blue nodes denote rare diseases, magenta nodes denote publications)
Cypher Query 5
MATCH p =(d:Disease)-[:isInvestigatedBy]-(n:Project)-[:isInvestigatedBy]-(d1:Disease) WHERE d.gard_id = 'GARD:0003434' RETURN p
In this study, we extracted NIH funding data for rare diseases and semantically represented it as a knowledge graph, which provides an effective way to not only assess the funding landscape in rare diseases, and systematically identify new research gaps/opportunities in rare diseases, but also share identified scientific findings/evidence with funding agencies for recommending their research fund distribution in rare diseases.
Scientific observations from data preparation
Given various representations of disease names applied in the project titles, to accurately map diseases to projects via project titles and avoid any mis-mapping, we applied a complementary mapping strategy using string match and semantic annotation. For instance, one project entitled “Discovering Novel Treatments for Batten Disease” could only be mapped to “Batten Disease (GARD:0010739)” via string match based on the disease name, instead of semantic annotation. The MetaMap annotations generated from the project title is “Juvenile Neuronal Ceroid Lipofuscinosis (UMLS: C0751383)”, which is different from the UMLS mapping (UMLS:C0027877) associated with this GARD disease. Another project entitled “TOXIC METALS, MEMBRANE SIGNALING, AND CELL GROWTH” is mapped to “Heavy metal poisoning (GARD:0006577)” via semantic annotation instead of string match, since the MetaMap annotator generates one annotation of “toxic metals (UMLS: C0274869)”, which is mapped to the UMLS associated with that GARD disease. Clearly, even though we applied this complementary strategy to establish mappings between projects and diseases, we may miss relevant projects with the disease mentioned in the project abstract, instead of in the project title. To avoid any missing data, several additional steps have been proposed and described in the “ Future work ” section.
Scientific insights derived from the case studies
We performed two types of case studies, funding landscape and research landscape analysis respectively to demonstrate the use of our funding knowledge graph for evidence-based rare disease research discovery.
Funding landscape assessment
Accessing funding data allows researchers to examine funding situations and funding opportunities in rare diseases. Our case studies illustrate that the funding trend consistently reflects the disease burden to the public health, e.g., infectious diseases received the most amount of funding support over years. A big jump regarding the total funding amount for infectious diseases between 2013 and 2017, coincides with the Ebola and Zika outbreaks that occurred during that timeframe. Another inspiring message derived from our analysis is that the amount of funding for supporting rare disease research has been increasing yearly, which might encourage and motivate more scientists to devote more of their research to rare diseases.
Scientific evidence-based rare disease research discovery
Analysis of funding data not only provides a systematic way to outline a complete research spectrum for an interested disease (category), but also generates scientific evidence supporting rare disease research discovery. For instance, the case study of Neuronal Ceroid Lipofuscinosis (NCL) illustrates that several different types of NCL have been investigated intensively and one therapeutic success on one type of NCL, namely, CLN2, which will enable us to dive into it and derive insight and knowledge about the status and gaps of research on NCL in further investigation. In addition, we demonstrated the power of aligning funded projects with their publications to direct research. As shown in the case study of Duchenne Muscular Dystrophy, it becomes feasible to cluster research papers based on a funded project or a list of projects with a similar research topic, which enables researchers to systematically track research pathway and programmatically prepare training data for future study. In this study, publication clusters were solely based on single projects; we propose to cluster publications with multiple projects with similar research topics by implementing Natural Language Processing (NLP) algorithms to analyze project abstracts.
Limitations and future work
By reviewing the MONDO categories applied to organize rare diseases, some categories, for instance, “Mendelian disease”, “disease by anatomical system”, are broad categories consisted of many individual diseases; In addition, as shown in Table 3 , most rare diseases are grouped into multiple MONDO categories. We propose to extend our disease category mapping to a higher granularity level as the next step, to precisely reflect funding distribution and assess research landscape by disease categories.
In this study, mappings between rare diseases and funded projects were established based on project titles. To avoid any mis-mappings with rare diseases that are mentioned in the project abstracts instead of project titles, we propose to expand our analysis with project abstracts. In addition, analyzing funding data from other resources, such as “funding” or “Acknowledgements” sections included in the publications to introduce the funding sources supporting their research, is another proposed extension task. Although the aforementioned extensions have been proposed as future work by aligning with our current project plan, we anticipated that we will still miss some data, such as, (1) projects without project titles and/or abstracts, (2) non-US government funded projects; (3) projects with only a single funding source (not all) was acknowledged in the publications. These are beyond the scope of this project and will be planned in the future study.
Insights and lessons drawn from the case studies were heavily relied on manual interpretation in this preliminary study, and we propose to transform currently manual processes into automated processes by implementing NLP and advanced machine learning techniques. Given the nature of rare diseases, limited data and knowledge about those diseases compared to common diseases, collaborative efforts seem more important and critical. We propose to discover methods to better promote research collaboration by connecting investigators with the requisite expertise and shared research interest from our funding knowledge graph. To that end, scientists can work collaboratively to pool patients, data, experience and resources together to support more innovative research in rare diseases. We are also interested in investigating the relationship between medical cost using information from datasets such as the AHRQ’s Healthcare Cost and Utilization Project (HCUP) [ 30 ] and research cost (i.e., NIH funding) in rare diseases, with the hypothesis that higher research funding should lead to improvements in earlier diagnosis of a rare disease and lower medical costs. Identifying overlaps and discrepancies between research status and medical situation will guide both further investigation and better inform decision makers on how to stimulate and advance research across more rare diseases.
In this preliminary study, we developed an integrative knowledge graph to semantically represent NIH research funding data for rare diseases and successfully demonstrated its use of directing and promoting scientific evidence based rare disease research discovery. With the success and lessons learned from this study, we propose multiple improvements/extensions as the next step, to fully utilize funding data to accelerate the pace of rare disease research.
Availability of data and materials
The data applied in this study can be accessed at http://grants4rd.ncats.io:7474/browser/ .
Abbreviations
Genetic and Rare Disease Information Center
Mondo Disease Ontology
NCATS GARD Knowledge Graph
Unified Medical Language System
Open Biological and Biomedical Ontologies
Natural Language Processing
Stoller JK. The challenge of rare diseases. Chest. 2018;153(6):1309–14.
Article Google Scholar
Gross CP, Anderson GF, Powe NR. The relation between funding by the National Institutes of Health and the burden of disease. N Engl J Med. 1999;340(24):1881–7.
Article CAS Google Scholar
We have a budget for FY 2019! https://www.nia.nih.gov/research/blog/2018/10/we-have-budget-fy-2019#:~:text=The%20total%20NIH%20appropriation%20for,Alzheimer's%20and%20related%20dementias%20research .
NIH funding bolsters rare diseases research collaborations. https://www.nih.gov/news-events/news-releases/nih-funding-bolsters-rare-diseases-research-collaborations .
Why is rare disease funding rare? https://pharmaphorum.com/views-and-analysis/why-is-rare-disease-funding-rare/ .
Stehr F, Forkel M. Funding resources for rare disease research. Biochim Biophys Acta: BBA Mol Basis Dis. 2013;1832(11):1910–2.
Franceschi AM, Rosenkrantz AB. Patterns of recent National Institutes of Health (NIH) funding to diagnostic radiology departments: analysis using the NIH RePORTER system. Acad Radiol. 2017;24(9):1162–8.
Ma A, Mondragón RJ, Latora V. Anatomy of funded research in science. Proc Natl Acad Sci. 2015;112(48):14760–5.
Packalen M, Bhattacharya J. NIH funding and the pursuit of edge science. Proc Natl Acad Sci. 2020;117(22):12011–6.
Yoon B-H, Kim S-K, Kim S-Y. Use of graph database for the integration of heterogeneous biological data. Genomics Inform. 2017;15(1):19.
Xu J, Kim S, Song M, Jeong M, Kim D, Kang J, et al. Building a PubMed knowledge graph. Sci Data. 2020;7(1):1–15.
Lal M. Neo4j graph data modeling. Birmingham: Packt Publishing Ltd; 2015.
Google Scholar
Zhu Q, Nguyen D-T, Grishagin I, Southall N, Sid E, Pariser A. An integrative knowledge graph for rare diseases, derived from the Genetic and Rare Diseases Information Center (GARD). J Biomed Semant. 2020;11(1):1–13.
The Genetic and Rare Diseases Information Center (GARD). https://rarediseases.info.nih.gov/ .
Mondo Disease Ontology. https://mondo.monarchinitiative.org/ .
NCATS Integrated Disease Ontologies. https://disease.ncats.io/browser/ .
NIH RePORT. https://report.nih.gov/ .
NIH ExPORTER. https://exporter.nih.gov/default.aspx .
Mondo Disease Ontology. http://www.obofoundry.org/ontology/mondo.html .
MetaMap. https://metamap.nlm.nih.gov/ .
Cypher Query Language - Developer Guides - Neo4j. https://neo4j.com/developer/cypher/ .
Global Polio Eradication Initiative (GPEI). https://polioeradication.org/ .
Polio Endgame Strategy. https://polioeradication.org/who-we-are/polio-endgame-strategy-2019-2023/#:~:text=The%20GPEI%20Polio%20Endgame%20Strategy,world%20free%20of%20all%20polioviruses.&text=The%20GPEI%20Polio%20Endgame%20Strategy%202019%2D2023%20was%20developed%20in,stakeholders%20from%20around%20the%20world .
TheGlobalFund. https://www.theglobalfund.org/en/ .
Batten Disease Fact Sheet. https://www.ninds.nih.gov/Disorders/Patient-Caregiver-Education/Fact-Sheets/Batten-Disease-Fact-Sheet .
Markham A. Cerliponase alfa: first global approval. Drugs. 2017;77(11):1247–9.
Enzyme Replacement Therapy. https://battendiseasenews.com/enzyme-replacement-therapy/ .
FDA approves twice-yearly leuprolide injection for central precocious puberty. https://www.healio.com/news/endocrinology/20200504/fda-approves-twiceyearly-leuprolide-injection-for-central-precocious-puberty#:~:text=A%20leuprolide%20acetate%20suspension%20to,in%20a%20polymeric%20gel%20form .
Zhang Q, Liu F. Advances and potential pitfalls of oncolytic viruses expressing immunomodulatory transgene therapy for malignant gliomas. Cell Death Dis. 2020;11(6):1–11.
AHRQ’s Healthcare Cost and Utilization Project (HCUP). https://www.ahrq.gov/data/hcup/index.html .
Download references
Open Access funding provided by the National Institutes of Health (NIH). This research was supported by the Intramural and Extramural research program of the NCATS, NIH.
Author information
Authors and affiliations.
Division of Pre-Clinical Innovation, National Center for Advancing Translational Sciences (NCATS), National Institutes of Health (NIH), Rockville, MD, 20850, USA
Qian Zhu, Ðắc-Trung Nguyễn, Timothy Sheils & Ewy A. Mathé
ICF International Inc, Rockville, MD, USA
Gioconda Alyea
Office of Rare Diseases Research, National Center for Advancing Translational Sciences (NCATS), National Institutes of Health (NIH), Bethesda, MD, 20892, USA
Eric Sid, Yanji Xu, James Dickens & Anne Pariser
You can also search for this author in PubMed Google Scholar
Contributions
The work was conceived by QZ, who designed and performed data analysis and drafted the manuscript; TN helped on Neo4j development; GA helped on case studies with funding landscape assessment; ES, EAM helped on case studies with research landscape assessment and manuscript edition; TS, YX, JD and AP participated in the project discussion and edited the manuscript. All authors read and approved the final manuscript.
Corresponding author
Correspondence to Qian Zhu .
Ethics declarations
Ethics approval and consent to participate.
Not applicable.
Consent for publication
Competing interests.
None declared.
Additional information
Publisher's note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
. 32 root disease categories from MONDO.
Additional file 2
. Cypher queries from the case studies.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Zhu, Q., Nguyễn, ÐT., Sheils, T. et al. Scientific evidence based rare disease research discovery with research funding data in knowledge graph. Orphanet J Rare Dis 16 , 483 (2021). https://doi.org/10.1186/s13023-021-02120-9
Download citation
Received : 13 May 2021
Accepted : 06 November 2021
Published : 18 November 2021
DOI : https://doi.org/10.1186/s13023-021-02120-9
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
Orphanet Journal of Rare Diseases
ISSN: 1750-1172
- Submission enquiries: Access here and click Contact Us
- General enquiries: [email protected]
- Program Finder
- Admissions Services
- Course Directory
- Academic Calendar
- Hybrid Campus
- Lecture Series
- Convocation
- Strategy and Development
- Implementation and Impact
- Integrity and Oversight
- In the School
- In the Field
- In Baltimore
- Resources for Practitioners
- Articles & News Releases
- In The News
- Statements & Announcements
- At a Glance
- Student Life
- Strategic Priorities
- Inclusion, Diversity, Anti-Racism, and Equity (IDARE)
- What is Public Health?
Research Gaps Around Type 1 Diabetes
A large body of research on Type 2 diabetes has helped to develop guidance, informing how patients are diagnosed, treated, and manage their lifestyle. In contrast, Type 1 diabetes, often mistakenly associated only with childhood, has received less attention.
In this Q&A, adapted from the April 17 episode of Public Health On Call , Stephanie Desmon speaks to Johns Hopkins epidemiologists Elizabeth Selvin , PhD '04, MPH, and Michael Fang , PhD, professor and assistant professor, respectively, in the Department of Epidemiology, about recent findings that challenge common beliefs about type 1 diabetes. Their conversation touches on the misconception that it’s solely a childhood condition, the rise of adult-onset cases linked to obesity, and the necessity for tailored approaches to diagnosis and care. They also discuss insulin prices and why further research is needed on medications like Ozempic in treating Type 1 diabetes.
I want to hear about some of your research that challenges what we have long understood about Type 1 diabetes, which is no longer called childhood diabetes.
MF: Type 1 diabetes was called juvenile diabetes for the longest time, and it was thought to be a disease that had a childhood onset. When diabetes occurred in adulthood it would be type 2 diabetes. But it turns out that approximately half of the cases of Type 1 diabetes may occur during adulthood right past the age of 20 or past the age of 30.
The limitations of these initial studies are that they've been in small clinics or one health system. So, it's unclear whether it's just that particular clinic or whether it applies to the general population more broadly.
We were fortunate because the CDC has collected new data that explores Type 1 diabetes in the U.S. Some of the questions they included in their national data were, “Do you have diabetes? If you do, do you have Type 1 or Type 2? And, at what age were you diagnosed?”
With these pieces of information, we were able to characterize how the age of diagnosis of Type 1 diabetes differs in the entire U.S. population.
Are Type 1 and Type 2 diabetes different diseases?
ES: They are very different diseases and have a very different burden. My whole career I have been a Type 2 diabetes epidemiologist, and I’ve been very excited to expand work with Type 1 diabetes.
There are about 1.5 million adults with Type 1 diabetes in the U.S., compared to 21 million adults with Type 2 diabetes. In terms of the total cases of diabetes, only 5 to 10 percent have Type 1 diabetes. Even in our largest epidemiologic cohorts, only a small percentage of people have Type 1 diabetes. So, we just don't have the same national data, the same epidemiologic evidence for Type 1 diabetes that we have for Type 2. The focus of our research has been trying to understand and characterize the general epidemiology and the population burden of Type 1 diabetes.
What is it about Type 1 that makes it so hard to diagnose?
MF: The presentation of symptoms varies by age of diagnosis. When it occurs in children, it tends to have a very acute presentation and the diagnosis is easier to make. When it happens in adulthood, the symptoms are often milder and it’s often misconstrued as Type 2 diabetes.
Some studies have suggested that when Type 1 diabetes occurs in adulthood, about 40% of those cases are misdiagnosed initially as Type 2 cases. Understanding how often people get diagnosed later in life is important to correctly diagnose and treat patients.
Can you talk about the different treatments?
MF: Patients with Type 1 diabetes are going to require insulin. Type 2 diabetes patients can require insulin, but that often occurs later in the disease, as oral medications become less and less effective.
ES: Because of the epidemic of overweight and obese in the general population, we’re seeing a lot of people with Type 1 diabetes who are overweight and have obesity. This can contribute to issues around misdiagnosis because people with Type 1 diabetes will have signs and will present similarly to Type 2 diabetes. They'll have insulin resistance potentially as a result of weight gain metabolic syndrome. Some people call it double diabetes—I don't like that term—but it’s this idea that if you have Type 1 diabetes, you can also have characteristics of Type 2 diabetes as well.
I understand that Type 1 used to be considered a thin person's disease, but that’s not the case anymore. MF: In a separate paper, we also explored the issue of overweight and obesity in persons with Type 1 diabetes. We found that approximately 62% of adults with Type 1 diabetes were either overweight or obese, which is comparable to the general U.S. population.
But an important disclaimer is that weight management in this population [with Type 1 diabetes] is very different. They can't just decide to go on a diet, start jogging, or engage in rigorous exercise. It can be a very, very dangerous thing to do.
Everybody's talking about Ozempic and Mounjaro—the GLP-1 drugs—for diabetes or people who are overweight to lose weight and to solve their diabetes. Where does that fit in with this population?
ES: These medications are used to treat Type 2 diabetes in the setting of obesity. Ozempic and Mounjaro are incretin hormones. They mediate satiation, reduce appetite, slow gastric emptying, and lower energy intake. They're really powerful drugs that may be helpful in Type 1 diabetes, but they're not approved for the management of obesity and Type 1 diabetes. At the moment, there aren't data to help guide their use in people with Type 1 diabetes, but I suspect they're going to be increasingly used in people with Type 1 diabetes.
MF: The other piece of managing weight—and it's thought to be foundational for Type 1 or Type 2—is dieting and exercising. However, there isn’t good guidance on how to do this in persons with Type 1 diabetes, whereas there are large and rigorous trials in Type 2 patients. We’re really just starting to figure out how to safely and effectively manage weight with lifestyle changes for Type 1 diabetics, and I think that's an important area of research that should continue moving forward.
ES: Weight management in Type 1 diabetes is complicated by insulin use and the risk of hypoglycemia, or your glucose going too low, which can be an acute complication of exercise. In people with Type 2 diabetes, we have a strong evidence base for what works. We know modest weight loss can help prevent the progression and development of Type 2 diabetes, as well as weight gain. In Type 1, we just don't have that evidence base.
Is there a concern about misdiagnosis and mistreatment? Is it possible to think a patient has Type 2 but they actually have Type 1?
MF: I think so. Insulin is the overriding concern. In the obesity paper, we looked at the percentage of people who said their doctors recommended engaging in more exercise and dieting. We found that people with Type 1 diabetes were less likely to receive the same guidance from their doctor. I think providers may be hesitant to say, “Look, just go engage in an active lifestyle.”
This is why it's important to have those studies and have that guidance so that patients and providers can be comfortable in improving lifestyle management.
Where is this research going next?
ES: What's clear from these studies is that the burden of overweight and obesity is substantial in people with Type 1 diabetes and it's not adequately managed. Going forward, I think we're going to need clinical trials, clear clinical guidelines, and patient education that addresses how best to tackle obesity in the setting of Type 1 diabetes.
It must be confusing for people with Type 1 diabetes who are hearing about people losing all this weight on these drugs, but they go to their doctor who says, “Yeah, but that's not for you.”
ES: I hope it's being handled more sensitively. These drugs are being used by all sorts of people for whom they are not indicated, and I'm sure that people with Type 1 diabetes are accessing these drugs. I think the question is, are there real safety issues? We need thoughtful discussion about this and some real evidence to make sure that we're doing more good than harm.
MF: Dr. Selvin’s group has published a paper, estimating that about 15% of people with Type 1 diabetes are on a GLP-1. But we don't have great data on what potentially can happen to individuals.
The other big part of diabetes that we hear a lot about is insulin and its price. Can you talk about your research on this topic?
MF: There was a survey that asked, “Has there been a point during the year when you were not using insulin because you couldn’t afford it?” About 20% of adults under the age of 65 said that at some point during the year, they couldn't afford their insulin and that they did engage in what sometimes is called “cost-saving rationing” [of insulin].
Medicare is now covering cheaper insulin for those over 65, but there are a lot of people for whom affordability is an issue. Can you talk more about that?
MF: The fight is not over. Just because there are national and state policies, and now manufacturers have been implementing price caps, doesn't necessarily mean that the people who need insulin the most are now able to afford it.
A recent study in the Annals of Internal Medicine looked at states that adopted or implemented out-of-pocket cost caps for insulin versus those that didn't and how that affected insulin use over time. They found that people were paying less for insulin, but the use of insulin didn't change over time. The $35 cap is an improvement, but we need to do more.
ES: There are still a lot of formulations of insulin that are very expensive. $35 a month is not cheap for someone who is on insulin for the rest of their lives.
- Overweight and Obesity in People With Type 1 Diabetes Nearly Same as General Population
- The Impacts of COVID-19 on Diabetes and Insulin
- Why Eli Lilly’s Insulin Price Cap Announcement Matters
Related Content

To Protect Human Health, We Must Protect the Earth’s Health

A South African Soup Kitchen Is Bringing Relief to Caregivers

New Grant Enables Johns Hopkins Researchers to Implement Community Health Worker-Led Health Interventions for Noncommunicable Diseases in Nepal

The Omnipresence of PFAS—and What We Can Do About Them

Summer Institute in Data to Policy
IMAGES
VIDEO
COMMENTS
News & Views 15 Apr 2024 Nature Reviews Clinical Oncology. P: 1-2. Kidney diseases. Metabolic disorders. Neurological disorders. Nutrition disorders. Oral diseases. Psychiatric disorders ...
Participants in clinical studies help current and future generations. Through these studies, researchers develop new diagnostic tests, more effective treatments, and better ways of managing diseases with genetic components. Participants in studies are actively involved in understanding their disorder and current research.
Developments in Alzheimer's disease research. One of the hallmarks of Alzheimer's is an abnormal buildup of amyloid-beta protein. A study in mice suggests that antibody therapies targeting amyloid-beta protein could be more effective after enhancing the brain's waste drainage system.In another study, irisin, an exercise-induced hormone, was found to improve cognitive performance in mice.
Research is strengthening surveillance, rapid diagnostics and development of vaccines and medicines. Public-private partnerships and other innovative mechanisms for research are concentrating on neglected diseases in order to stimulate the development of vaccines, drugs and diagnostics where market forces alone are insufficient.
Methods. To semantically represent NIH funding data for rare diseases and advance its use of effectively promoting rare disease research, we identified NIH funded projects for rare diseases by mapping GARD diseases to the project based on project titles; subsequently we presented and managed those identified projects in a knowledge graph using Neo4j software, hosted at NCATS, based on a pre ...
Abstract. As the 21st century unfolds, strategies to prevent and control infectious diseases remain an area of vital interest and concern. The burden of disease, disability, and death caused by infectious diseases is felt around the world in both developed and developing nations. Moreover, the ability of infectious agents to destabilize ...
Main Areas of Focus. Research projects will include surveillance studies to identify previously unknown viral causes of febrile illnesses in humans, the animal sources of viral or other disease-causing pathogens, and to determine what genetic or other changes make these pathogens capable of infecting humans.
Our research is focused on identifying molecular mechanisms that allow epidemic S. aureus strains such as USA300 to successfully disseminate. This project uses a combined approach of whole-genome comparative sequencing of longitudinally collected samples, genetic manipulation, and functional studies on bacterial adhesion and survival.
Research Projects. Infectious diseases, particularly emerging pathogens, are an important public health concern across the globe, as well as the institute's home state of South Carolina. ... The Institute for Infectious Disease Translational Research is a multi-primary investigator endeavor, with highly regarded experts in various fields ...
The Division of Infectious Diseases participates in graduate programs and research in microbiology and molecular genetics, immunology and molecular pathogenesis, as well as population biology, ecology, and evolution. Additional opportunities are available for basic science research in: Toxin-mediated infections. Intracellular pathogens. Influenza.
The United States should fund a new dedicated Disease X Medical Countermeasure Program that leverages technologies and vaccine platforms most suitable to the viral families that are likely to cause future catastrophic disease outbreaks. Medical countermeasures against 1 member of a viral family could easily be adapted to another member quickly ...
Proposed Solution: The Rare Disease and Research Engagement (RaRE) project will develop a Rare Disease Partnership Model and stakeholder-informed patient-centered outcomes research (PCOR) priorities at the intersection of rare disease and mental health. Objectives: Build national network of diverse rare disease stakeholders interested in PCOR ...
Explore the wide range of research subjects you can undertake with the guidance of dedicated, enthusiastic faculty. Topics for research projects with specific investigators include: Acinetobacter baumannii pathogenesis ( Thomas Russo) Bioinformatics ( Elaine Haase; Alan Lesse; Kedar Aras; Marc Halfon) Drug development ( Thomas Suchyna; Thomas ...
A comprehensive list of infectious diseases that CIDRAP covers. Our site is an authoritative, reliable, and timely source of science-based information about global, emerging infectious diseases.
It's important to note that the construction of models should be based on the type of disease, research objectives, and available data. In this section, models are categorized into data-driven models and mechanism-driven models. ... In some large projects, this step may be called "build a computational model for the model." ...
TDR, the Special Programme for Research and Training in Tropical Diseases, is a global programme of scientific collaboration that helps facilitate, support and influence efforts to combat diseases of poverty. It is co-sponsored by the United Nations Children's Fund (UNICEF), the United Nations Development Programme (UNDP), the World Bank and the World Health Organization (WHO).
Research Projects. Cardiovascular dysfunction accounts for some of the most common and devastating diseases in the country, as well in the institute's home state of South Carolina. This research promises to uncover new understandings and breakthroughs to reduce mortality and morbidity rates due to cardiovascular disease.
If yes, you will find this list interesting. This category comprises hot topics in infectious disease fields. Consider some of these ideas for your research paper. The virology, epidemiology, and prevention of COVID-19. The diagnosis of COVID-19. Prevention vaccines for SARS-CoV-2 infection.
Research Proposal: Hypertension and Chronic Kidney Disease. "The Bear Came Over the Mountain": True Love and Alzheimer's Disease. Prevention of Chronic Disease in the Modern Society. Chickenpox: Disease Control and Prevention. Peru - Globalization, Environment, Crime and Disease. Analysis of Alzheimer's Disease.
Pichard — a clinician and leader in rare diseases research — advocated for her daughter's diagnosis. She had recognized that her daughter showed signs of Rett syndrome — a neurodevelopmental condition that is often marked by loss of developmental abilities between 6 to 18 months of age. ... Project GIVE focuses on a community-based ...
Science Fair Project Idea. In a survey conducted from 2007 to 2010, the U.S. Centers for Disease Control and Prevention reported that about 49% of people in the United States had taken at least one prescription drug during the past month, and about 22% of people had taken three or more prescription drugs. People are prescribed drugs all the ...
Infectious Disease, Cancer/Oncology. 10/24/12. 8/13/24. An Observational Study to Assess the Prevalence and Outcomes of Primary Pulmonary Coccidioidomycosis in Persons Aged >14 years Presenting with Community Acquired Pneumonia (CAP) in Endemic Areas (SAnds-PPC) Mohamed Fayed, MD.
A genetic disorder is a disease caused in whole or in part by a change in the DNA sequence away from the normal sequence. Genetic disorders can be caused by a mutation in one gene (monogenic disorder), by mutations in multiple genes (multifactorial inheritance disorder), by a combination of gene mutations and environmental factors, or by damage to chromosomes (changes in the number or ...
Preventing Chronic Disease (PCD) is a peer-reviewed electronic journal established by the National Center for Chronic Disease Prevention and Health Promotion. PCD provides an open exchange of information and knowledge among researchers, practitioners, policy makers, and others who strive to improve the health of the public through chronic disease prevention.
This special Research in Context feature explores the development of more effective ways to treat depression, including personalized treatment approaches and both old and new drugs. ... Gum disease-related bacteria tied to colorectal cancer. Intermittent fasting for weight loss in people with type 2 diabetes. How SARS-CoV-2 contributes to heart ...
To semantically represent NIH funding data for rare diseases and advance its use of effectively promoting rare disease research, we identified NIH funded projects for rare diseases by mapping GARD diseases to the project based on project titles; subsequently we presented and managed those identified projects in a knowledge graph using Neo4j ...
The Patient-Centered Outcomes Research Institute (PCORI) intends to issue a Topical PCORI Funding Announcement (PFA) on May 7, 2024, seeking to fund high-quality, patient-centered comparative clinical effectiveness research (CER) projects that focus on rare diseases.
Our Research Priorities. Research Themes. Cancer Disparities; Hereditary Cancers; Immunotherapy; Population Health; Precision Medicine; Key Initiatives. ... 2024 Research Fellowship Awards to support three exciting disease intervention research projects | ScienceX.com | April 11, 2024 Read more at ScienceX.com. Footer. For Patients For ...
Recent research has highlighted disparities in research between Type 1 and Type 2 diabetes, with Type 1 long—and mistakenly—associated only with childhood onset. ... Type 1 diabetes was called juvenile diabetes for the longest time, and it was thought to be a disease that had a childhood onset. When diabetes occurred in adulthood it would ...