7.6 Transverse lie and shoulder presentation
A transverse lie constitutes an absolute foeto-pelvic disproportion, and vaginal delivery is impossible.
This is an obstetric emergency, because labour is obstructed and there is a risk of uterine rupture and foetal distress.

7.6.1 Diagnosis
- The uterus is very wide: the transverse axis is virtually equivalent to the longitudinal axis; fundal height is less than 30 cm near term.
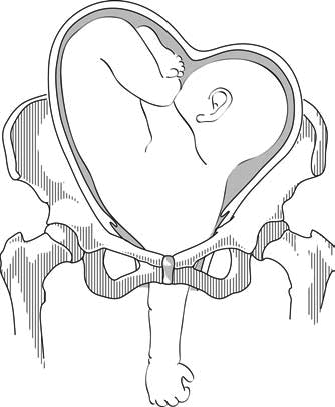
- On examination: head in one side, breech in the other (Figures 7.1a and 7.1b). Vaginal examination reveals a nearly empty true pelvis or a shoulder with—sometimes—an arm prolapsing from the vagina (Figure 7.1c).
Figures 7.1 - Transverse lie and shoulder presentation
| - Dorso-inferior (back down) left shoulder presentation |
- Dorso-superior (back up) left shoulder presentation |
7.6.2 Possible causes
- Grand multiparity (5 deliveries or more)
- Uterine malformation
Twin pregnancy
- Prematurity
- Placenta praevia
- Foeto-pelvic disproportion
7.6.3 Management
This diagnosis should be made before labour begins, at the last prenatal visit before the birth.
At the end of pregnancy
Singleton pregnancy.
- External version 4 to 6 weeks before delivery, in a CEmONC facility ( Section 7.7 ).
- If this fails, delivery should be carried out by caesarean section, either planned or at the beginning of labour (Chapter 6, Section 6.4.1 ).
- External version is contra-indicated.
- If the first twin is in a transverse lie (unusual): schedule a caesarean section.
- If the second twin is in a transverse lie: there is no indication for caesarean section, but plan delivery in a CEmONC facility so that it can be performed if necessary. Deliver the first twin and then, assess the foetal position and give a few minutes for the second twin to adopt a longitudinal lie. If the second twin stays in a transverse lie, and depending on the experience of the operator, perform external version ( Section 7.7 ) and/or internal version ( Section 7.8 ) on the second twin.
During labour, in a CEmONC facility
Foetus alive and membranes intact.
- Gentle external version, between two contractions, as early as possible, then proceed as with normal delivery.
- If this fails: caesarean section.
Foetus alive and membranes ruptured
- Multipara with relaxed uterus and mobile foetus, and an experienced operator: internal version and total breech extraction.
- Primipara, or tight uterus, or immobile foetus, or engaged arm, or scarred uterus or insufficiently-experienced operator: caesarean section.
- Incomplete dilation: caesarean section.
Caesarean section can be difficult due to uterine retraction. Vertical hysterotomy is preferable. To perform extraction, grasp a foot in the fundus (equivalent to a total breech extraction, but by caesarean section).
Foetus dead
Embryotomy for transverse lie (Chapter 9, Section 9.7.7 ).
During labour, in remote settings where surgery is not available
Try to refer the patient to a CEmONC facility. If not feasible:
- Attempt external version as early as possible.
- If this fails, wait for complete dilation.
- Perform an external version ( Section 7.7 ) combined with an internal version ( Section 7.8 ), possibly placing the woman in various positions (Trendelenburg or knee-chest).
- Put the woman into the knee-chest position.
- Between contractions, push the foetus back and try to engage his head.
- Vacuum extraction (Chapter 5, Section 5.6.1 ) and symphysiotomy (Chapter 5, Section 5.7 ) at the slightest difficulty.
- Incomplete dilation: Trendelenburg position and watchful waiting until complete dilation.
Try to refer the patient, even if referral takes some time. If not feasible, embryotomy for transverse lie (Chapter 9, Section 9.7.7 ).
- Search Please fill out this field.
- Newsletters
- Sweepstakes
What Is a Transverse Baby?
Although rare, a baby can be in a transverse lie position in the third trimester. Here's what that means and how it impacts delivery.
What Does Transverse Lie Mean?
What are the causes of a transverse lie position, what are the possible risks and complications, how can the transverse lie position affect pregnancy, what about delivery, can you turn a transverse baby.
Getty Images
During pregnancy, the fetus moves around into different fetal positions , but most end up in the optimal head down, face down (cephalic occiput anterior) position in the last few weeks. When the fetus doesn’t move into the cephalic position for birth, it’s called fetal malpresentation.
One of the rarest positions is the transverse lie, where the fetus lies horizontally, often with one shoulder down or pressing against the birth canal. If you have a transverse baby at term, the provider will intervene because a vaginal delivery is not possible.
Here’s all you need to know about transverse lie causes and how it may affect pregnancy and delivery.
The transverse lie position is when the fetus lies across the pregnant person’s abdomen horizontally. Because the shoulder is often in the pelvic inlet, it is also sometimes called shoulder presentation. But the fetus can also have its back facing the birth canal or with feet and hands facing it.
The chances of the baby being in the sideways position at term are only around 1 in 300. But before term, at 32 weeks gestation, it’s as high as 1 in 50.
“Transverse lie is normal in the first trimester, common in the second, unusual in the third, and it’s not a position where vaginal birth is possible,” says Gail Tully, CPM, creator of Spinning Babies, a website which offers ways to ease a baby’s rotation through the pelvis based on its position.
Often, a clear cause or risk factor for a transverse lie position is unknown. “But two of the most common risk factors for transverse lie at term include having extra amniotic fluid —often associated with diabetes but can be found on its own—and multiple gestation , such as twins or triplets,” says Layan Alrahmani, MD , maternal and fetal medicine specialist and assistant professor in obstetrics and gynecology at Loyola University Medical Center.
Other possible risk factors for transverse lie include:
- Multiparity (previous births may lead to lax abdominal muscles)
- Premature labor
- Low amniotic fluid
- Placenta previa (placenta is covering the pregnant person’s cervix)
- Pelvic, uterine, or fetal abnormalities (the latter is more common in primiparity, or first time births)
“Sometimes the baby is in the position for a reason,” says Karolyn Zambrotta, CNM , an obstetrics and gynecology specialist. “And after the doctor does the C-section you’ll find the problem, like a short or tight umbilical cord.”
Transverse lie at term can be risky for both the pregnant person and baby.
“The transverse lie is frequently found early in the pregnancy. But if the baby does not change position, then a vaginal delivery cannot occur and we have to plan differently,” says Carolina Bibbo, MD , maternal-fetal medicine specialist at Brigham and Women’s Hospital. “If the water were to break when the baby is in a transverse lie position, the cord could prolapse which is an obstetrical emergency.”
Other possible complications include:
- Obstructed labor
- Uterine rupture
- Birth trauma
- Postpartum hemorrhage
- Birth defects
Some pregnant people feel abdominal and back pain during pregnancy when the fetus is in the sideways position. This is related to the uterus being stretched in different ways and can cause tightening in the ribs and cramping lungs. If your health care provider approves, you can try deep breathing and gentle yoga exercises at home to help relieve pain and encourage the fetus to turn.
If the health care provider still suspects the fetus is lying horizontal at 36 weeks, an ultrasound will be performed to confirm. Because a baby in the transverse lie position cannot be delivered vaginally, your providers will develop an alternate birth plan which can include a procedure called external cephalic version (ECV) to try and turn the fetus for vaginal delivery, or a C-section.
In the case of multiples, triplets are almost always delivered via C-section. But for twins, if the first is head down, the second may drop into the cephalic position for normal delivery having more room after the first one comes out. “You could also try ECV or internal podalic version (IPV) on the second twin if needed,” says Dr. Alrahmani. “It’s really case by case and depends on the provider’s experience and preference too.”
After 34 weeks, it is very unlikely for a fetus in transverse lie to spontaneously change to the optimal head down position. But, in some cases, it is possible to turn a transverse baby.
Natural methods
If the fetus is not head down by 32 weeks, and there are no health concerns, midwives like Zambrotta might first recommend trying some natural techniques. As Dr. Bibbo notes, the data is limited for different approaches but yoga positions can help in some cases.
Low-risk methods to encourage transverse babies to turn include sound or light (putting music or a bright light near the bottom of the uterus), temperature (placing something cold like frozen peas behind the head and something warm like a rice-filled sock at the bottom of the stomach), and Traditional Chinese Medicine (TCM) like moxibustion , which involves heating acupuncture points with a stick of mugwort.
Small studies have shown that the Webster technique, a gentle chiropractic approach that aligns the pelvis, can help correct fetal malpresentation. And the forward leaning inversion, also developed by a chiropractor, is the most effective position for transverse lie babies, according to Tully, who trains labor and delivery nurses on body balance techniques.
Always speak with your health care professional before trying any methods to turn the fetus.
Intervention
If natural methods have not helped by 36 weeks, your provider will likely want to try an ECV in which they use their hands to put pressure on your belly to try and turn the fetus head down. This procedure should be done in a hospital setting to monitor the fetal heart rate, and for the rare case where an emergency C-section is needed. Possible complications include placental abruption, fetal heart rate abnormalities (FHR), premature rupture of the membranes , preterm labor, fetal distress, and vaginal bleeding.
ECV may not be safe if you have placenta previa, a low amount of amniotic fluid, a significant uterine abnormality, vaginal bleeding, high blood pressure, multiples (before delivery of the first twin), or fetal distress.
“In general, the success rate for external cephalic version is 60% of babies,” explains Dr. Bibbo. “But there’s a greater chance for ECV to turn a fetus in transverse lie than in a breech position.”
A baby in the transverse lie position cannot fit through the pregnant person’s pelvis. If gentle exercises, chiropractic techniques, or other natural methods don’t help your baby turn by 36 weeks, you may be a candidate for ECV to move the baby into the optimal head down position for birth. But if ECV doesn’t work, then the health care provider will schedule a C-section.
Whatever ends up being needed to ensure the safety of both parent and fetus, it's always important to ask any questions you may have. That includes information on postpartum recovery should you need a C-section.
Chapter 26: Transverse Lie . Oxorn-Foote Human Labor & Birth, 7e . 2023.
Effectiveness and Safety of Acupuncture and Moxibustion in Pregnant Women with Noncephalic Presentation: An Overview of Systematic Reviews . Evidence-Based Complementary and Alternative Medicine . 2019.
The Webster Technique: a chiropractic technique with obstetric implications . J Manipulative Physiol Ther . 2002.
External Cephalic Version . StatPearls. 2022.
External Cephalic Version . Obstetrics: Normal and Problem Pregnancies (Seventh Edition) , 2017.
External Cephalic Version: A Dying Art Worth Reviving . J Obstet Gynaecol India . 2018.
Related Articles
- Vishal's account
- Prenatal Care
Shoulder Presentation – All You Should Be Aware Of

When Does the Fetus Move in Birthing Position?
What is shoulder presentation, what is transverse lie, what is the frequency of shoulder presentation, what causes shoulder presentation, how is shoulder presentation diagnosed, complications of shoulder presentation, how is shoulder presentation managed.
Most doctors and midwives will recommend that you have a natural vaginal birth if you have a choice. However, there are certain complications that can sometimes present themselves and stop this from happening. Shoulder presentation is one such complication.
A baby will most likely begin to move into the birthing position latest by week 30 . She will have her head down and facing your spine, her body and face more inclined to one side and arms will be folded across the chest. Any other position is not normal.
This is an abnormal fetus position where the baby is in a transverse lie , causing the baby’s shoulder to be positioned to come out first if vaginal delivery is attempted. However, since this is very easy to diagnose, doctors will always recommend a C-Section and never even suggest attempting to deliver the child through normal vaginal delivery.
A transverse lie is a position where your baby is lying sideways with her head to one of your sides and her bottom at your other side. This position is considered normal before 26 gestational weeks.

Shoulder presentation takes place in 1 out of every 300 births and is commonly seen in premature and macerated babies. It is five times more likely to happen in a woman who has had children before than it is to occur in a first-time mother. Mothers carrying twins are also 40% more likely to have at least one baby in shoulder position.
Here are some reasons why a shoulder presentation can take place:
1. Contracted Pelvis
A very narrow pelvis in the mother can cause a shoulder presentation to occur.
2. Placenta Previa
A condition where the placenta covers the uterus opening, either completely or partially. This makes it difficult for your baby’s head to enter the pelvic brim.
3. Intra-Uterine Fetal Death
There are times when the fetus dies inside the womb, and when this happens, the muscle tone starts to degenerate, which results in the fetus falling lower into the uterus.
4. Lax Abnormal Musculature
Women who have had multiple pregnancies may have more relaxed uterine and abdominal muscles. This will make their ability to keep the baby in a normal position very difficult.
5. Uterine Over Distension
There are many reasons why a uterus can become enlarged. Some of these include a large baby, polyhydramnios , multiple pregnancies and others. A uterus that is too large very often leads to shoulder presentation.
6. Polyhydramnios
A very large amount of amniotic fluid that is present in the uterus is known as polyhydramnios. This causes the fetus to be able to move very freely in the uterus and will lead to shoulder presentation.
7. Uterine Abnormalities
There are different abnormalities in the uterus that can cause your baby to move into shoulder presentation. Some of these are the bicornuate uterus, a sub-septate uterus and even a large fibroid uterus .
Here is how Shoulder presentation diagnosed:
- The top of the mother’s uterus to the top of the pelvic bone is called a fundus. The height of the fundus is an indicator of whether or not the baby is in the shoulder presentation.
- The uterus becomes broader.
- The mother can feel the baby’s head on one abdominal side.
- If shoulder presentation takes place, arms prolapse will cause the baby’s arm to be seen outside the vagina.
- During a vaginal examination, the doctor will be able to feel the babies ribs.
If your doctor identifies that you have shoulder presentation before you go into labour, he will opt for a C-Section instead. If there is a case of neglected shoulder presentation and it is only identified after you go into labour, it becomes very dangerous, and you face many complications. Here are some of the complications that can occur:
1. Cord Prolapse
When the umbilical cord comes out before the fetus does, it is called a cord prolapse and is very dangerous as it can cause the baby’s heart rate to drop, cause changes in blood pressure and even result in brain damage or death of the baby.
2. Ruptured Uterus
The myometrial wall is the middle layer of the wall of the uterine. The breach of this layer during childbirth is a rupture in the uterus, and it is very dangerous for both mother and child.
3. Fetal Hypoxia
When your baby doesn’t get enough oxygen, it will lead to suffocation, and if the necessary measures are not taken, it will result in death.
4. Obstructed Labour
Though contractions are taking place, the baby is not able to come through the birth canal as there is something blocking the way. Failure to diagnose and remedy this condition is a major reason why both mother and child die during childbirth.
5. Trauma to Prolapsed Arm
If there is a prolapsed arm, there is a higher chance that it will be injured or damaged. This injury may be severe and could last for a lifetime.
Here is how Shoulder presentation is managed:
1. C-Section
The first choice for doctors who have a case of shoulder presentation is a C-Section. This is the safest method that ensures the safety of both mother and child.
2. External Cephalic Version
In this procedure, your baby’s heartbeat will be monitored, and you will be given medication through an IV to ensure a relaxed uterus. Your doctor will then place her hands on the outside of your stomach and attempt to turn your baby into the correct position. This is done only before labour starts.
3. Internal Podalic Version
This is only used in the case of twins, where the second twin will need to be moved into a breech position and then extracted.
Though it sounds scary, if you keep a careful track of your baby’s position in the weeks before delivery, you will be able to identify and rectify the problem before it becomes serious. Exercising throughout your pregnancy will be very helpful in ensuring that your baby gets into the correct position for labour.
Also Read: When Does a Baby Turn Head Down During Pregnancy?

- RELATED ARTICLES
- MORE FROM AUTHOR

Consuming Ginger During Pregnancy

Tooth Extractions During Preganancy- Is It Safe?

5 Things You Didn't Know Your Baby Could Do In The Womb

Baby Shower Thank You Notes - What You Should Write

Consuming Antacids During Pregnancy

6 Effective Ways to Prevent Gestational Diabetes
Popular on parenting.

245 Rare Boy & Girl Names with Meanings

Top 22 Short Moral Stories For Kids

170 Boy & Girl Names That Mean 'Gift from God'

800+ Unique & Cute Nicknames for Boys & Girls
Latest posts.

Cholera Disease: Causes, Symptoms, Treatment and Vaccination

4th of July Coloring Pages - Free Printable Pages For Kids
Happy 4th of july gifs to share and celebrate us independence day.

Father's Day Coloring Pages - Free Printables For Kids

Shoulder presentation
October 14, 2016
A shoulder presentation refers to a malpresentation at childbirth where the baby is in a transverse lie (its vertebral column is perpendicular to that of the mother), thus the leading part (the part that enters first the birth canal) is an arm, shoulder, or the trunk. While a baby can be delivered vaginally when either the head or the feet/buttocks are the leading part, it usually cannot be expected to be delivered successfully with a shoulder presentation unless a cesarean section (C/S) is performed.
Shoulder presentations are uncommon (about 0.5% of births) as usually towards the end of gestation either the head or the buttocks start to enter the upper part of the pelvis anchoring the fetus in a longitudinal lie. It is not known in all cases of shoulder presentation why the longitudinal lie is not reached, but possible causes include bony abnormalities of the pelvis, uterine abnormalities such as malformations or tumors (fibroids), and other tumors in the pelvis or abdomen can also lead to a shoulder presentation. Other factors are a lax abdominal musculature, uterine overdistension (i.e. polyhydramnios), multiple gestation, placenta previa, a small fetus, or a fetus with some abnormality. Further, if the amniotic fluid sac ruptures the shoulder or arm may become wedged as a shoulder presentation.
Inspection of the abdomen may already give a clue as it is wide from side to side. Usually performing the Leopold’s maneuvers will demonstrate the transverse lie of the fetus. Ultrasound examination delivers the diagnosis and may indicate possible causes such as multiple gestation or a tumor. On vaginal examination, the absence of a head or feet/breech is apparent.
Shoulder presentations are classified into four types, based on the location of the scapula:
Left scapula-anterior (LSA) Right scapula-anterior (RSA) Left scapula-posterior (LSP) Right scapula-posterior (RSP)
William Smellie – Shoulder presentation Public Domain Image
Shoulder presentation. (2016, May 28). In Wikipedia, The Free Encyclopedia . Retrieved 04:07, May 28, 2016, from https://en.wikipedia.org/w/index.php?title=Shoulder_presentation&oldid=722440427
Insert/edit link
Enter the destination URL
Or link to existing content
Fetal Presentation, Position, and Lie (Including Breech Presentation)
- Key Points |
Abnormal fetal lie or presentation may occur due to fetal size, fetal anomalies, uterine structural abnormalities, multiple gestation, or other factors. Diagnosis is by examination or ultrasonography. Management is with physical maneuvers to reposition the fetus, operative vaginal delivery , or cesarean delivery .
Terms that describe the fetus in relation to the uterus, cervix, and maternal pelvis are
Fetal presentation: Fetal part that overlies the maternal pelvic inlet; vertex (cephalic), face, brow, breech, shoulder, funic (umbilical cord), or compound (more than one part, eg, shoulder and hand)
Fetal position: Relation of the presenting part to an anatomic axis; for vertex presentation, occiput anterior, occiput posterior, occiput transverse
Fetal lie: Relation of the fetus to the long axis of the uterus; longitudinal, oblique, or transverse
Normal fetal lie is longitudinal, normal presentation is vertex, and occiput anterior is the most common position.
Abnormal fetal lie, presentation, or position may occur with
Fetopelvic disproportion (fetus too large for the pelvic inlet)
Fetal congenital anomalies
Uterine structural abnormalities (eg, fibroids, synechiae)
Multiple gestation
Several common types of abnormal lie or presentation are discussed here.

Transverse lie
Fetal position is transverse, with the fetal long axis oblique or perpendicular rather than parallel to the maternal long axis. Transverse lie is often accompanied by shoulder presentation, which requires cesarean delivery.
Breech presentation
There are several types of breech presentation.
Frank breech: The fetal hips are flexed, and the knees extended (pike position).
Complete breech: The fetus seems to be sitting with hips and knees flexed.
Single or double footling presentation: One or both legs are completely extended and present before the buttocks.
Types of breech presentations
|
Breech presentation makes delivery difficult ,primarily because the presenting part is a poor dilating wedge. Having a poor dilating wedge can lead to incomplete cervical dilation, because the presenting part is narrower than the head that follows. The head, which is the part with the largest diameter, can then be trapped during delivery.
Additionally, the trapped fetal head can compress the umbilical cord if the fetal umbilicus is visible at the introitus, particularly in primiparas whose pelvic tissues have not been dilated by previous deliveries. Umbilical cord compression may cause fetal hypoxemia.

Predisposing factors for breech presentation include
Preterm labor
Uterine abnormalities
Fetal anomalies
If delivery is vaginal, breech presentation may increase risk of
Umbilical cord prolapse
Birth trauma
Perinatal death

Face or brow presentation
In face presentation, the head is hyperextended, and position is designated by the position of the chin (mentum). When the chin is posterior, the head is less likely to rotate and less likely to deliver vaginally, necessitating cesarean delivery.
Brow presentation usually converts spontaneously to vertex or face presentation.
Occiput posterior position
The most common abnormal position is occiput posterior.
The fetal neck is usually somewhat deflexed; thus, a larger diameter of the head must pass through the pelvis.
Progress may arrest in the second phase of labor. Operative vaginal delivery or cesarean delivery is often required.
Position and Presentation of the Fetus
Toward the end of pregnancy, the fetus moves into position for delivery. Normally, the presentation is vertex (head first), and the position is occiput anterior (facing toward the pregnant patient's spine) with the face and body angled to one side and the neck flexed. Abnormal presentations include face, brow, breech, and shoulder. Occiput posterior position (facing toward the pregnant patient's pubic bone) is less common than occiput anterior position. |
If a fetus is in the occiput posterior position, operative vaginal delivery or cesarean delivery is often required.
In breech presentation, the presenting part is a poor dilating wedge, which can cause the head to be trapped during delivery, often compressing the umbilical cord.
For breech presentation, usually do cesarean delivery at 39 weeks or during labor, but external cephalic version is sometimes successful before labor, usually at 37 or 38 weeks.

Copyright © 2024 Merck & Co., Inc., Rahway, NJ, USA and its affiliates. All rights reserved.
- Cookie Preferences

GFMER Geneva Foundation for Medical Education and Research
- Annual reports
- GFMER members
- Country coordinators
- Obstetric fistula
- Cervical cancer
- Emergency and surgical care
- Picture of the week
- Social media
- Free medical journals
Obstetrics Simplified - Diaa M. EI-Mowafi
Shoulder Presentation (Transverse or Oblique lie)
- The longitudinal axis of the foetus does not coincide with that of the mother.
- These are the most hazardous malpresentations due to mechanical difficulties that occur during labour .
- The oblique lie which is deviation of the head or the breech to one iliac fossa, is less hazardous as correction to a longitudinal lie is more feasible.
3-4% during the last quarter of pregnancy but 0.5% by the time labour commences.
Factors that
- change the shape of pelvis, uterus or foetus,
- allow free mobility of the foetus or
- Contracted pelvis.
- Lax abdominal wall.
- Uterine causes as bicornuate, subseptate and fibroid uterus.
- Pelvic masses as ovarian tumours.
- Multiple pregnancy.
- Polyhydramnios.
- Placenta praevia.
- Prematurity.
- Intrauterine foetal death.
The scapula is the denominator
- Left scapulo-anterior.
- Right scapulo-anterior.
- Right scapulo-posterior.
- Left scapulo-posterior.
Scapulo-anterior are more common than scapulo-posterior as the concavity of the front of the foetus tends to fit with the convexity of the maternal spines.
During pregnancy
- The abdomen is broader from side to side.
- Fundal level: lower than that corresponds to the period of amenorrhoea.
- Fundal grip: The fundus feels empty.
- Umbilical grip: The head is felt on one side while the breech one the other. In transverse lie, they are at the same level, while in oblique lie one pole, usually the head as it is heavier, is in a lower level i.e. in the iliac fossa.
- First pelvic grip: Empty lower uterine segment.
- FHS are best heard on one side of the umbilicus towards the foetal head.
- Confirms the diagnosis and may identify the cause as multiple pregnancy or placenta praevia.
During labour
In addition to the previous findings, vaginal examination reveals:
- The presenting part is high.
- Membranes are bulging.
- Premature rupture of membranes with prolapsed arm or cord is common. The dorsum of the supinated hand points to the foetal back and the thumb towards the head. The right hand of the foetus can be shacked, correctly by the right hand of the obstetrician and the left hand by the left one.
- When the cervix is sufficiently dilated particularly after rupture of the membranes, the scapula, acromion, clavicle, ribs and axilla can be felt.
Mechanism of Labour
As a rule no mechanism of labour should be anticipated in transverse lie and labour is obstructed.
If a patient is allowed to progress in labour with a neglected or unrecognized transverse lie, one of the following may occur:
- This is the usual and most common outcome.
- The lower uterine segment thins and ultimately ruptures.
- The foetus becomes hyperflexed, placental circulation is impaired, cord is prolapsed and compressed leading to foetal asphyxia and death.
- Rarely the foetal lie may be corrected by the splinting effect of the contracted uterine muscles so that the head presents.
- Rarely, by similar process the breech may come to present.
- Very rarely, if the foetus is very small or dead and macerated, the shoulder may be forced through the pelvis followed by the head and trunk.
- Very rarely, the head is retained above the pelvic brim, the neck greatly elongates, the breech descends followed by the trunk and the after -coming head, i.e. spontaneous version occurs in the pelvic cavity.
External cephalic version
Can be done in late pregnancy or even early in labour if the membranes are intact and vaginal delivery is feasible. In early labour, if version succeeded apply abdominal binder and rupture the membranes as if there are uterine contractions.
Internal podalic version
It is mainly indicated in 2nd twin of transverse lie and followed by breech extraction.
Prerequisites:
- General or epidural anaesthesia.
- Fully dilated cervix.
- Intact membranes or just ruptured.
Caesarean section
- It is the best and safest method of management in nearly all cases of persistent transverse or oblique lie even if the baby is dead.
- As rupture of membranes carries the risk of cord prolapse, an elective caesarean section should be planned before labour commences.
Neglected (Impacted) shoulder
Clinical picture (impending rupture uterus)
- Exhaustion and distress of the mother.
- Shoulder is impacted may be with prolapsed arm and / or cord.
- Membranes are ruptured since a time.
- Liquor is drained.
- The uterus is tonically contracted.
- The foetus is severely distressed or dead.
- Caesarean section is the safest procedure even if the baby is dead. A classical or low vertical incision in the uterus facilitates extraction of the foetus as a breech in such a condition.
- Any other manipulations will lead eventually to rupture uterus so they are contraindicated.
UNSTABLE LIE
A foetus which changes its lie frequently from transverse to oblique to longitudinal.
- Polyhydramnios.
- Prematurity and IUFD.
- Contracted pelvis.
- Placenta praevia.
- Pelvic tumours.
- Multiparae with a lax uterus and abdominal wall.
- Can be done whenever the woman is examined but in majority of cases it will recur so it is better to defer it until full term (37-40 weeks).
- After correcting the foetal lie to longitudinal, apply an abdominal binder, start oxytocin infusion and do amniotomy when the uterine contractions started and the presenting part is well settled into the pelvic brim.
- Failure of external version .
- Some do it selectively in cases discovered after 40 weeks’ gestation.
- Shoulder dystocia : Guidelines, reviews
Fastest Obstetric, Gynecology and Pediatric Insight Engine
- Abdominal Key
- Anesthesia Key
- Basicmedical Key
- Otolaryngology & Ophthalmology
- Musculoskeletal Key
- Obstetric, Gynecology and Pediatric
- Oncology & Hematology
- Plastic Surgery & Dermatology
- Clinical Dentistry
- Radiology Key
- Thoracic Key
- Veterinary Medicine
- Gold Membership
Malpresentation, Malposition, Cephalopelvic Disproportion and Obstetric Procedures
26 Malpresentation, Malposition, Cephalopelvic Disproportion and Obstetric Procedures Kim Hinshaw 1,2 and Sabaratnam Arulkumaran 3 1 Sunderland Royal Hospital, Sunderland, UK 2 University of Sunderland, Sunderland, UK 3 St George’s University of London, London, UK Malpresentation, malposition and cephalopelvic disproportion Definitions The vertex is a diamond‐shaped area on the fetal skull bounded by the anterior and posterior fontanelles and laterally by the parietal eminences. Vertex presentation is found in 95% of labours at term and is associated with flexion of the fetal head. Breech, brow, face and shoulder presentations constitute the remaining 5% and are collectively known as malpresentations . Their aetiology is usually unknown, but associations include macrosomia, multiparity, polyhydramnios, multiple pregnancy, placenta praevia, preterm labour, and anomalies of the uterus or pelvis (congenital or acquired, e.g. lower segment fibroids) and more rarely the fetus. The denominator is a laterally sited bony eminence on the presenting part (‘occiput’ for vertex presentation, ‘mentum’ for face, ‘acromium’ for shoulder and ‘sacrum’ for breech). The position of the presenting part is defined by the relationship of the denominator to the maternal bony pelvis. The vertex enters the pelvis in the occipito‐transverse (OT) position and during descent rotates to an occipito‐anterior (OA) position in 90% of cases. This position is associated with a well‐flexed head, allowing the smallest anteroposterior (suboccipito‐bregmatic) and lateral (biparietal) diameters to pass through the pelvis (both 9.5 cm). Malposition occurs when the occiput remains in a tranverse or posterior position as labour progresses. Persistent malposition results in deflexion with a larger anteroposterior diameter presenting (occipito‐frontal 11.5 cm). It is associated with increasing degrees of anterior or posterior asynclitism , with one of the parietal bones preceding the sagittal suture (in posterior asynclitism, the posterior parietal bone leads; Fig. 26.1 ). Significant degrees of asynclitism can result in labour dystocia and a higher risk of operative delivery [1] . Fig. 26.1 Posterior asynclitism of the vertex: posterior parietal bone presenting below the sagittal suture. In most cases, flexion occurs as the vertex descends onto the pelvic floor, leading to correction of the malposition and a high chance of spontaneous delivery. The level of the presenting part should be critically assessed as labour progresses. On abdominal examination, the head should descend until it is no more than 1/5 palpable in the late first stage. On vaginal examination the presenting part is assessed relative to the level of the ischial spines. Care must be taken to assess the level using the lowest bony part . Malposition is associated with increased moulding of the fetal skull and a large caput succedaneum, which may give false reassurance about the true degree of descent. In modern obstetric practice, operative vaginal delivery is not attempted if the leading edge of the skull is above the ischial spines (i.e. above ‘0’ station; Fig. 26.2 ). Fig. 26.2 Level of the presenting part relative to the ischial spines. Malpresentations Breech presentation The incidence of breech presentation varies according to gestation: 20% at 30 weeks falling to 4% by term. The aetiology of most breech presentations at term is unclear but known factors to consider include placenta praevia, polyhydramnios, bicornuate uterus, fibroids and, rarely, spina bifida or hydrocephaly. Types of breech presentation Between 50 and 70% of breech presentations manifest with hips flexed and knees extended (extended breech) Complete (or flexed) breech is more common in multiparous women and constitutes 5–10% at term (hips and knees flexed; Fig. 26.3 ). Incomplete or footling breech (10–30%) presents with one or both hips extended, or one or both feet presenting and is most strongly assoiated with cord prolapse (5–10%). Knee presentation is rare. Fig. 26.3 The common types of breech presentation. Clinical diagnosis may miss up to 20% of breech presentations, relying on identifying the head as a distinct hard spherical hard mass to one or other side under the hypochondrium which distinctly ‘ballots’. In such cases the breech is said to feel broader and an old adage reminds us: ‘Beware the deeply engaged head – it is probably a breech!’ Auscultation may locate the fetal heart above the maternal umbilicus and ultrasound confirmation should be considered. Antenatal management If breech presentation is suspected at 36 weeks, ultrasound assessment is recommended as it allows a comprehensive assessment of the type of breech, placental site, estimated fetal weight, confirmation of normality and exclusion of nuchal cord or hyperextension of the fetal neck. External cephalic version (ECV) is encouraged after 36 or more weeks as the chance of spontaneous version to cephalic presentation after 37 weeks is only 8%. Absolute contraindications are relatively few but include placenta praevia, bleeding within the last 7 days, abnormal cardiotocography (CTG), major uterine anomaly, ruptured membranes and multiple pregnancy [2] . Couples should receive counselling about the procedure and its success rates and complications, and the subsequent management of persistent breech presentation. Tocolysis increases the likelihood of success, with average rates of 50% (range 30–80%). Women should be made aware that even with a cephalic presentation following ECV, labour is still associated with a higher rate of obstetric intervention than when ECV has not been required. ECV should be performed in a setting where urgent caesarean section (CS) is available in case of fetal compromise during or soon after ECV. CTG for 30–40 min prior to and after ECV should provide confirmation of fetal health. The chance of success is greater with multiparity, flexed breech presentation and an adequate liquor volume. The use of moxibustion at 33–35 weeks, in combination with acupuncture, may reduce the numbers of births by CS. Training specialist midwives is potentially cost‐efficient with success rates comparable to consultant‐led services (51–66%) [3] . The first step in ECV involves disengaging the breech by moving the fetus up and away from the pelvis, shifting it to a sideways position, followed by a forward somersault to move the head to the lower pole; if this fails a backward somersault can be tried. The need for emergency delivery by CS because of suspected fetal compromise is estimated to be 0.5%. Mothers who are rhesus‐negative should have a Kleihauer–Betke test after the procedure and receive anti‐D. If ECV is unsuccessful, women who are keen to avoid CS may be offered a repeat attempt under neuraxial blockade. This increases the chances of success (58.4% vs. 43.1%; relative risk, RR 1.44, 95% CI 1.27–1.64) and reduces the incidence of CS (46.0% vs. 55.3%; RR 0.83, 95% CI 0.71–0.97) [4] . Otherwise appropriate counselling about the options of elective CS or assisted vaginal breech delivery should be offered. Deciding mode of delivery Despite increasing evidence supporting elective CS for breech delivery at term, controversy and debate continue among professional groups. Breech presentation at term diagnosed antenatally . The Term Breech Trial is the largest published randomized controlled trial where the primary outcome (serious perinatal morbidity and mortality) favoured planned CS over planned vaginal birth: 17/1039 (1.6%) versus 50/1039 (5.0%; RR 0.33, 95% CI 0.19–0.56; P <0.0001) [5] . The trial concluded that ‘planned CS is better than planned VB for the term fetus in the breech presentation; serious maternal complications are similar between the groups’. This has significantly changed practice in many countries despite continuing debate and criticism about the trial design and intepretation of outcomes. However, the latest systematic review has confirmed a significant increased perinatal risk associated with planned vaginal birth [6] . Breech at term diagnosed in labour and preterm breech delivery . Observational trials of term breech ‘undiagnosed’ until presentation in labour confirm that this group has a high vaginal delivery rate with relatively low perinatal morbidity. In a similar vein, the evidence to guide best practice for delivery of the preterm breech remains equivocal, decisions often being based on individual interpretation of the data and local custom and practice. Conducting a vaginal breech delivery For women who wish to deliver vaginally, antenatal selection aims to ensure optimal outcome for mother and baby but remains relatively subjective. Women with frank and complete breech presentations (fetal weight <4000 g) encounter minimal problems, while those with footling breech are advised elective CS because of the increased risk of cord prolapse. CT or X‐ray pelvimetry do not appear to improve outcome. Spontaneous onset of labour is preferred and labour management is similar to vertex presentation. Successful outcome depends on a normal rate of cervical dilatation, descent of the breech and a normal fetal heart rate (FHR) pattern. Where progress of labour is poor and uterine contractions are inadequate, oxytocin augmentation can be used juidiciously with early resort to emergency CS if progress remains slow (<0.5 cm/hour), particularly in the late first stage. Epidural anaesthesia prevents bearing down before the cervix is fully dilated and is particularly important for labour with a preterm breech, when there is a real risk of head entrapment in the incompletely dilated cervix if pushing commences too early. For all breech labours, the mother should be encouraged to avoid bearing down for as long as possible. It is best to wait until the anterior buttock and anus of the baby are in view over the mother’s perineum, with no retraction between contractions. Classically, the mother’s legs are supported in the lithotomy position (the alternative upright breech technique is described later). Primigravidae will usually require an episiotomy with appropriate analgesia, although multigravidae can be assessed as the perineum stretches up. The buttocks deliver in the sacro‐tranverse position. The mother should be encouraged to push with contractions, aiming for an unassisted delivery up to and beyond the level of the umbilicus. There is no need to pull down a loop of cord. The accoucheur should sit with hands ready, but resting on their own legs. Assistance is only required if the legs do not deliver. Gentle abduction of the fetal thigh whilst hyperflexing the hip, followed by flexing the lower leg at the knee will release the foot and leg ( Fig. 26.4 ). Fig. 26.4 Delivery of extended legs by gentle abduction of the thigh with hyperflexion at the hip, followed by flexion at the knee: (a) right leg; (b) left leg. When the scapulae are visible with the arms flexed in front of the chest, sweep each arm around the side of the fetal chest to deliver using a finger placed along the length of the humerus. If the scapulae are not easily seen or if the arms are not easily reached, they may be extended above the shoulders. This can be resolved using the Løvset manoeuvre. Hold the baby by wrapping both hands around the bony pelvis, taking care not to apply pressure to the soft fetal abdomen. Rotate the baby 180° to bring the posterior shoulder to the front, i.e. to lie anteriorly ( Fig. 26.5 a). Complete delivery of the anterior arm by gently flexing the baby laterally downwards towards the floor; the arm will deliver easily from under the pubic ramus ( Fig. 26.5 b). Repeat the 180° rotation in the opposite direction, bringing the posterior shoulder to the front, then flex the baby laterally downwards to deliver the second arm. Fig. 26.5 Løvset’s manoeuvre for extended arms: (a) rotation to bring the posterior (left) arm to the front followed by (b) delivery of the left arm (now anterior) from under the pubic ramus. Nuchal displacement (an arm trapped behind the fetal neck) is rare. If the left arm is trapped, the baby will need to be rotated in a clockwise direction to ‘unwrap’ the arm so that it can be reached. If the right arm is involved, anticlockwise rotation is needed. Allow the head to descend into the pelvis, assisted by the weight of the fetus until the nape of the neck is visible under the symphysis pubis. Ensure slow controlled delivery of the head using one of four methods. Mauriceau–Smellie–Veit manoeuvre: two fingers are placed on the maxilla, lying the baby along the forearm. Hook index and fourth fingers of the other hand over the shoulders with the middle finger on the occiput to aid flexion. Apply traction to the shoulders with an assistant applying suprapubic pressure if needed ( Fig. 26.6 ). Burns–Marshall method: grasp the feet, apply gentle traction and swing the baby gently up and over the maternal abdomen until the mouth and nose appear. Forceps are applied to the head from below, with an assistant supporting the baby’s body in the horizontal plane avoiding hyperextension. Kielland’s forceps can be useful as they lack a pelvic curve. Apply traction, bringing the forceps upwards as the mouth and nose appear. The upright breech technique is increasingly popular in midwifery deliveries. Mobility is encouraged with delivery on all fours, sitting (on a birth stool), kneeling, standing or lying in a lateral position. Delivery is spontaneous with no manual assistance in 70% of cases and a reduced incidence of perineal trauma (14.9%). Fig. 26.6 Delivery of the head using the Mauriceau–Smellie–Veit manoeuvre assisted by suprapubic pressure. Entrapment of the aftercoming head This rare complication occurs in two situations. If the fetal back is allowed to rotate posteriorly, the chin may be trapped behind the symphysis pubis. Correction requires difficult internal manipulation to free the chin by pushing it laterally. McRoberts’ manoeuvre and suprapubic pressure may help. Symphysiotomy is a last resort that can increase the available pelvic diameters. In preterm delivery, the body can slip through an incompletely dilated cervix, with resulting head entrapment. If the cervix cannot be ‘stretched up’ digitally, surgical incisions are made in the cervical ring at 2, 6 and 10 o’clock (Dührssen incisions). Head entrapment in the contractile upper segment can occur at CS. Acute tocolysis and/or extension of the uterine incision may be required to release the head. Women should be intimately involved in decisions about mode of breech delivery and the available evidence presented appropriately. A senior midwife or a doctor experienced in assisted breech delivery must be present. As vaginal breech deliveries decline, developing expertise in breech delivery now relies on simulation training and experience of breech delivery at CS. Summary box 26.1 ECV has a high success rate (51–66%) and should be encouraged. Ensure the fetal back does not rotate posteriorly during breech delivery. The most experienced accoucheur available should directly supervise vaginal breech delivery. Brow presentation Brow presentation occurs in 1 in 1500–3000 deliveries. The head is partially deflexed (extended), with the largest diameter of the head presenting (mento‐vertical, 13.5 cm). The forehead is the lowest presenting part but diagnosis relies on identifying the prominent orbital ridges lying laterally. The eyeballs and nasal bridge may just be palpated lateral to the orbital ridges. Position is defined using the frontal bone as the denominator (i.e. ‘fronto‐‘). Persistent brow presentation results in true disproportion, but when diagnosed in early labour careful assessment of progress is appropriate. Flexion to vertex or further extension to face presentation occurs in 50% and vaginal delivery is possible. Cautious augmentation with oxytocin should only be considered in nulliparous patients for delay in the early active phase of labour. If brow presentation persists, emergency CS is recommended. Vaginal delivery of a brow presentation is possible in extreme prematurity. Preterm labour is best managed in the same way as term labour, with delivery by CS if progress slows or arrests. Cord prolapse is more common and, though rare, uterine rupture can occur in neglected labour or with injudicious use of oxytocin. For this reason labour should not be augmented in multigravid patients with a confirmed brow presentation if progress is inadequate. Face presentation Face presentation occurs in 1 in 500–800 labours. The general causes of malpresentation apply for face presentation, but fetal anomalies (neck or thyroid masses, hydrocephalus and anencephaly) should be excluded. The fetal head is hyperextended and the occiput may be felt higher and more prominently on the same side as the fetal spine. However, face presentation is rarely diagnosed antenatally. On vaginal examination in labour, diagnosis relies on feeling the mouth, malar bones, nose and orbital ridges. Position is defined using the chin or mentum as the denominator. The mouth and malar bones form a triangle which can help differentiate face presentation from breech, where the anus lies in a straight line between the prominent ischial tuberosities. Face presentation is often first diagnosed in late labour. The submento‐bregmatic diameter (9.5 cm) is compatible with normal delivery but only with the fetus in a mento‐anterior position (60%) ( Fig. 26.7 ). The same diameter presents with a persistent mento‐posterior position (25%) but this cannot deliver vaginally as the fetal neck is maximally extended. Fetal scalp clips, blood sampling and vacuum extraction are absolutely contraindicated. Forceps delivery from low cavity can be undertaken for mento‐anterior or mento‐lateral positions by an experienced accoucheur but CS may still be required when descent is poor. Fig. 26.7 The anteroposterior submento‐bregmatic diameter of face presentation. Shoulder presentation The incidence of shoulder presentation at term is 1 in 200 and is found with a transverse or oblique lie. Multiparity (uterine laxity) and prematurity are common associations and placenta praevia must be excluded. The lie will usually correct spontaneously before labour as uterine tone increases, although prolapse of the cord or arm is a significant risk if membranes rupture early. For this reason, hospital admission from 38 weeks is recommended for persistent transverse lie. External version can be offered (and may also be considered for transverse lie presenting in very early labour). On vaginal examination, the denominator is the acromium but defining position can be difficult. If membrane rupture occurs at term with the uterus actively contracting, delivery by CS should be undertaken promptly to avoid an impacted transverse lie. If the uterus is found to be moulded around the fetus, a classical CS is recommended to avoid both fetal and maternal trauma. In cases of intrauterine death with a transverse lie, spontaneous vaginal delivery is possible for early preterm fetuses by extreme flexion of the body (spontaneous evolution). However, CS will usually be required beyond mid‐trimester, although a lower segment approach may be used. Malposition and cephalopelvic disproportion In higher‐income countries, cephalopelvic disproportion is usually ‘relative’ and due to persistent malposition or relative fetal size (macrosomia). Classically we consider these problems with regard to the passage, the passenger or the powers, either alone or in combination. The passage Absolute disproportion due to a contracted pelvis is now rare in higher‐income countries unless caused by severe pelvic trauma and this should be known before the onset of labour. Caldwell and Moloy described four types of pelvis: gynaecoid (ovoid inlet, widest transversely, 50%), anthropoid (ovoid inlet, widest anteroposterior, 25%), android (heart‐shaped inlet, funnel‐shaped, 20%) and platypelloid (flattened gynaecoid, 3%). These can influence labour outcome but as pelvimetry is rarely used and clinical assessment of pelvic shape is inaccurate, this rarely influences clinical mangement in labour. The anthropoid pelvis is associated with a higher risk of persistent occipito‐posterior (OP) position and relative disproportion. The passenger and OP malposition Fetal anomalies (e.g. hydrocephalus, ascites) where disproportion may be a problem in labour are usually assessed antenatally and delivery by elective CS considered. Fetal macrosomia is increasing, related to the rising body mass index (BMI) in many pregnant populations. The evidence for inducing non‐diabetic women with an estimated fetal weight above the 90th centile (or >4000 g) in order to reduce cephalopelvic disproportion remains equivocal. Malposition is an increasingly common cause of disproportion and may be related to a sedentary lifestyle. OP position is associated with deflexion and/or asynclitism with a larger diameter presenting. Optimal uterine activity will correct the malposition in 75% of cases. Flexion occurs as the occiput reaches the pelvic floor with long rotation through 135° to an OA position and a high chance of normal delivery. Moulding of the fetal skull and pelvic elasticity (related to changes at the symphysis pubis) are dynamic changes that facilitate progress in labour and delivery. Short rotation through 45° to direct OP can result in spontaneous ‘face to pubes’ delivery, although episiotomy may be required to allow the occiput to deliver. Persistent OP position occurs in up to 25% of cases and is associated with further deflexion. The risk of assisted delivery is high because of relative disproportion as the presenting skull diameters increase. Delivery in the OP position from mid‐cavity (0 to +2 station) requires critical assessment to decide whether delivery should be attempted vaginally or abdominally and is discussed in later sections. The powers Disproportion is intimately related to dystocia and failure to progress in labour. National Institute for Health and Care Excellence (NICE) guidelines recommend that first stage delay is suspected with cervical dilatation of less than 2 cm in 4 hours when forewater amniotomy should be offered. Delay is confirmed if progress is less than 1 cm 2 hours later and oxytocin augmentation should be offered [6] . This shortens labour but does not affect operative delivery rates. High‐dose oxytocin may reduce CS rates but larger trials are required before these regimens are used routinely. The decision to use oxytocin in labour arrest in multigravid patients must only be made by the most senior obstetrician and should always be approached with extreme caution as uterine rupture is a possible consequence. In the second stage, particularly with epidural analgesia, passive descent for at least 1 hour is recommended, and possibly longer if the woman wishes, before encouraging active pushing. With regional analgesia and a normal FHR pattern, birth should occur within 4 hours of full dilatation regardless of parity [7] . Oxytocin may be commenced in nulliparous patients in the passive phase if contractions are felt to be inadequate and particularly with the persistent OP position. Failure of second‐stage descent combined with excessive caput or moulding suggests disproportion and requires critical assessment to decide the appropriate mode of delivery. Summary box 26.2 OP position with deflexion of the head and asynclitism results in relative disproportion compounded by inadequate uterine activity. With epidural analgesia in place, passive descent should be encouraged for at least 1 hour. Augmentation with oxytocin should be used with extreme caution in multigravid patients with labour arrest. Instrumental vaginal deliveries Background The incidence of instrumental vaginal delivery (IVD) varies widely and in Europe ranges from 0.5% (Romania) to 16.4% (Ireland), although there is no direct relationship with CS rates [ 8 , 9 ]. Epidural analgesia is associated with higher IVD rates. Allowing a longer passive second stage for descent results in less rotational deliveries and possibly a reduction in second‐stage CS [ 10 , 11 ]. Common indications for IVD include delay in the second stage of labour due to inadequate uterine activity, malposition with relative disproportion, maternal exhaustion and fetal compromise. Women with severe cardiac, respiratory or hypertensive disease or intracranial pathology may require IVD to shorten the second stage (when forceps may be preferred). Assessment and preparation for IVD The condition of the mother and fetus and the progress of labour should be assessed prior to performing IVD. Personal introductions to the woman and her partner are essential, explaining the reason for IVD and ensuring a chaperone and enough support are available. The findings, plan of action and the procedure itself should be explained and the discussions carefully recorded. Verbal or written consent is obtained. The mother and her partner may be physically and emotionally exhausted and great care should be exercised in terms of behaviour, communication and medical action. On abdominal examination, the fetal head should be no more than 1/5 palpable (preferably 0/5). A scaphoid shape to the lower abdomen may indicate an OP position. The FHR pattern should be assessed, noting any clinical signs of fetal compromise (e.g. fresh meconium). With acute fetal compromise (e.g. profound bradycardia, cord prolapse) delivery must be expedited urgently and this may only allow a brief explanation to be given to the patient and her partner at the time. If contractions are felt to be infrequent or short‐lasting, an oxytocin infusion should be considered in the absence of signs of fetal compromise. Both vacuum and forceps deliveries are associated with an almost threefold increased risk of shoulder dystocia compared with spontaneous delivery and this should be anticipated. However, it remains unclear whether this increased incidence is a cause or effect phenomenon [12] . On vaginal examination the cervix should be fully dilated with membranes absent. The colour and amount of amniotic fluid is recorded. Excessive caput or moulding may suggest the possibility of disproportion. Inability to reduce overlapping skull bones with gentle pressure is designated ‘moulding +++’; overlapping that reduces by gentle digital pressure is ‘moulding ++’, and meeting of the bones without overlap is ‘moulding +’. Identification of position, station, degree of deflexion and asynclitism will help decide whether IVD is appropriate, where it should be undertaken and who should undertake the procedure. Successful IVD is associated with station below the spines and progressive descent with pushing. If the head is 1/5 palpable abdominally, the leading bony part of the head is at the level of the ischial spines (mid‐cavity). When the head is more than 1/5 palpable and/or when station is above the spines, delivery by CS is recommended. Position is determined by identification of suture lines and fontanelles. The small posterior fontanelle (PF) lies at the Y‐shaped junction of the sagittal and lambdoidal sutures but may be difficult to feel when there is marked caput. The anterior fontanelle (AF) is a larger diamond‐shaped depression at the junction of the two parietal and two frontal bones. It can be differentiated from the PF by identifying the four sutures leading into the fontanelle. In deflexion (particularly OP positions) the AF lies centrally and is easily felt. Position can be confirmed by reaching for the pinna of the fetal ear, which can be flicked forwards indicating that the occiput lies in the opposite direction. Reaching the ear suggests descent below the mid‐pelvic strait. The degree of asynclitism should be assessed (see Fig. 26.1 ), with increasing degrees suggesting disproportion and a potentially more difficult IVD. Assessment of level and position can be difficult with OP position and in obesity. If there is any doubt after careful clinical examination, ultrasound assessment is recommended. The fetal orbits are sought and the position of the spine is noted. This is simple to do and can reduce the incorrect diagnosis of fetal position without delaying delivery, although on its own may not reduce morbidity associated with IVD [13] . IVD is normally performed with the mother in the dorsal semi‐upright position with legs flexed and abducted, supported by lithotomy poles or similar. The procedure is performed with good light and ideally aseptic conditions. The vulva and perineum should be cleansed and the bladder catheterized if the woman is unable to void. Adequate analgesia is essential and requires careful individualized assessment. Epidural anaesthesia is advisable for mid‐cavity IVD (i.e. station 0 to +2 cm below the ischial spines; see Fig. 26.2 ). In the absence of a pre‐existing epidural, spinal anaesthesia may be considered. IVD at station +2 cm or below is termed ‘low‐cavity’ and regional or pudendal block with local perineal infiltration (20 mL 1% plain lidocaine) can be used. Outlet IVD is performed when the head is on or near the perineum with the scalp visible without separating the labia. Descent to this level is associated with an OA position requiring minimal or no rotation and perineal infiltration with pudendal anaesthesia is effective. When the vertex is below the spines, IVD is carried out with different types of forceps or vacuum equipment, depending on the position and station of the vertex and the familiarity and experience of the doctor. Overall, comparing outcomes is easier if designation is by station and position at the time of instrumentation (e.g. left OP at +3) rather than simply mid, low or outlet IVD [ 11 , 14 ]. Choice of instruments: forceps or ventouse The choice of instrument depends on the operator’s experience, familiarity with the instrument, station and position of the vertex. Therefore, knowledge of the station and the position of the vertex is essential. The fetus in an OA position in the mid/low cavity can be delivered using non‐rotational, long or short‐handled forceps or a vacuum device: silicone, plastic or anterior metal cups (with suction tubing arising from the dorsum of the cup) are all suitable. For the fetus lying OT at mid‐ or low‐cavity, or lying OP position mid‐cavity, Kielland’s forceps or vacuum devices can be used to correct the malposition. Manual rotation is another technique to consider. Low‐cavity direct OP positions can be delivered ‘face to pubis’ but this may cause signifcant perineal trauma as the occiput delivers. For this reason, an OP vacuum cup (with the suction tubing arising from the edge of the cup) may be preferred. The cup will promote flexion and late rotation to OA often occurs on the perineum just prior to delivery. The Kiwi OmniCup® is an all‐purpose disposable vacuum delivery system with a plastic cup and in‐built PalmPump™ suitable for use in all positions of the vertex. Later models also display force traction to help the accoucheur avoid cup slippage ( http://clinicalinnovations.com/portfolio‐items/kiwi‐complete‐vacuum‐delivery‐system/ ) Forceps delivery Forceps come in pairs and most have fenestrated blades with a cephalic and pelvic curve between the heel and toe (distal end) of each blade. The heel continues as a shank which ends in the handle. The handles of the two blades sit together and meet at the lock. The cephalic curve fits along either side of the fetal head with the blades lying on the maxilla or malar eminences in the line of the mento‐vertical diameter ( Fig. 26.8 a). When correctly attached, uniform pressure is applied to the head, with the main traction force applied over the malar eminences. The shanks are over the flexion point, allowing effective traction in the correct direction. Non‐rotational forceps (the longer‐handled Neville Barnes or Simpson, and the shorter‐handled Wrigley’s) have a distinct pelvic curve that allows the blades to lie in the line of the pelvic axis whilst the handles remain horizontal. Kielland’s forceps have a minimal pelvic curve to allow rotation within the pelvis to correct malposition. Fig. 26.8 (a) Malar forceps application showing mento‐vertical diameter; (b) forceps traction (Pajot’s manoeuvre). Prior to applying forceps, the blades should be assembled to check whether they fit together as a pair. All forceps have matching numbers imprinted on the handles or shanks and these should also be checked. Non‐rotational forceps can be applied when the vertex is no more than 45° either side of the direct OA position (i.e. right OA to left OA). Application and delivery in a direct OP position is also possible but not routinely recommended because of increased perineal trauma. The left blade is inserted first using a light ‘pencil grip’, negotiating the pelvic and cephalic curves with a curved movement of the blade between the fetal head and the operator’s right hand, which is kept along the left vaginal wall for protection. Hands are swapped to insert the right blade using the same technique. Correct application results in the handles lying horizontally, right on top of left, and locking should be easy. Before applying traction, correct application must be confirmed: (i) the sagittal suture is lying midline, equidistant from and parallel to the blades; (ii) the occiput is no more than 2–3 cm above the level of the shanks (i.e. head well‐flexed); and (iii) no more than a fingertip passes into the fenestration at the heel of the blade. From mid‐ and low‐cavity, Pajot’s maneouvre should be used, balancing outward traction with one hand with downward pressure on the shanks with the other ( Fig. 26.8 b, white arrow). The handles are kept horizontal to avoid trauma to the anterior vaginal wall from the toes of the blades. Traction is synchronized with contractions and maternal effort, and the resultant movement is outwards down the line of the pelvic axis until the head is crowning. An episiotomy is usually needed as the perineum stretches up. The direction of traction is now upwards once the biparietal eminences emerge under the pubic arch and the head is born by extension. The mother will usually ask to have her baby handed to her immediately (unless active resuscitation is required). After completing the third stage, any perineal trauma is repaired and a full surgical count completed. The procedure, including plans for analgesia and bladder care, should be fully documented. Rotational forceps Kielland’s forceps have a minimal pelvic curve allowing rotation of the head at mid‐cavity. They are powerful forceps requiring a skilled accoucheur who is willing to abandon the procedure if progress is not as expected. The number of units able to teach use of Kielland’s forceps to the point of independent practice is declining in the UK. The forceps should match and are applied so that the knobs on the handles face the fetal occiput. Kielland’s are used to correct both OT and OP positions using two methods of application. Direct application involves sliding each blade along the side of the head if space permits, and is more easily achieved with OP positions. Wandering application is useful in OT positions. The first blade is applied in front of the fetal face, from where it is gently ‘wandered’ around to lie in the usual position alongside the malar bone. The posterior blade is applied directly using the space in the pelvic sacral curve. If application is difficult or the blades do not easily lock, the procedure should be abandoned. Correct application should be confirmed. Once locked, it is essential to hold the handles at a relatively steep angle downwards in the line of the mid‐pelvic axis in order to achieve easy rotation. Asynclitism is corrected using the sliding lock, moving the shanks over each other until the knobs are aligned. Rotation should take place between contractions, using only gentle force. Rotation may require the fetal head to be gently disimpacted, either upwards or downwards but no more than 1‐cm displacement is needed. Correct application should be checked again after rotation. Traction should result in progressive descent and an episiotomy is usually required. At the point of delivery, the handles of Kielland’s are only just above the horizontal because of the lack of pelvic curve. If there is no descent with traction during three contractions with maternal effort, the procedure should be abandoned. Whether Kielland’s delivery takes place in the delivery room or in obstetric theatre requires careful assessment of fetal and maternal condition, analgesia and labour progress. If there is any doubt, a formal trial of forceps should be arranged. Vacuum delivery Ventouse or vacuum delivery is increasingly favoured over forceps delivery for similar indications in the second stage of labour. The prerequisites to be satisfied before vacuum delivery are the same as for all forms of IVD. Vacuum delivery is contraindicated below 34 +0 weeks and should be used with caution between 34 +0 to 36 +0 weeks [11] . Overall it is contraindicated for fetuses with possible haemorrhagic tendencies (risk of subgaleal haemorrhage) and before full dilatation [11] . Experienced practitioners may consider vacuum after 8 cm in a multigravid patient in some circumstances. There are many types of vacuum cup in regular use, made of different materials and of differing shapes. Whichever cup is used, the aim is to ensure that the centre of the cup is directly over the flexion point. The flexion point is 3 cm in front of the occiput in the midline and is the point where the mento‐vertical diameter exits the fetal skull [15] . Traction on this point promotes flexion, presenting the smallest diameters for descent through the pelvis: this is the optimum flexing median application ( Fig. 26.9 a). Other applications increase the risk of cup detachment, failed vacuum delivery and scalp trauma. In decreasing order of effectiveness, these are the flexing paramedian application ( Fig. 26.9 b), the deflexing median application ( Fig. 26.9 c) and the deflexing paramedian application ( Fig. 26.9 d). Fig. 26.9 Placement of the vacuum cup, from most favourable (a) to unfavourable (d). (a) Flexing median; (b) flexing paramedian; (c) deflexing median; (d) deflexing paramedian. It is vitally important to select the correct cup and this will vary depending on both the position and attitude of the fetus. The soft Silc, Silastic or anterior metal cups (where the tubing is attached on the dorsum of the cup) are not suitable for OT or OP positions, as their shape and configuration do not allow application over the flexion point. They are suitable for OA positions where the flexion point is accessible in the midline. Metal cups come in different sizes, usually 4, 5 or 6 cm in diameter. In a systematic review they were more likely to result in successful vaginal birth than soft cups (RR 1.63, 95% CI 1.17–2.28), but with more cases of scalp injury (RR 0.67, 95% CI 0.53–0.86) and cephalhaematoma (RR 0.61, 95% CI 0.39–0.95) [16] . A specially designed cup should be used for OT and OP positions: metal OP cups have tubing emerging from the lateral aspect of the cup and the Kiwi OmniCup has a groove in the dorsum of the cup to accommodate the flexible stem. These cups can be manoeuvred more laterally or posteriorly to reach the flexion point. Hand‐held vacuum is associated with more failures than metal ventouse [16] , although a larger study suggested that the OmniCup has an overall failure rate of 12.9% [11] . Aldo Vacca (1941–2014) was the doyen of vacuum delivery and (with reference to the flexion point and cup application) his favourite quote was ‘It’s always more posterior than you think’. After ensuring flexion point application, the cup must be held firmly on the fetal scalp, and a finger should be run around the rim to ensure that no maternal tissue is entrapped. A vacuum of 0.2 bar (150 mmHg or 0.2 kg/cm 2 negative pressure) is created using a hand‐held or mechanical pump, before rechecking the position over the flexion point and confirming maternal tissue is not trapped. The vacuum is increased to 0.7–0.8 bar (500–600 mmHg or 0.8 kg/cm 2 ) in one step, waiting 2 min where possible to develop the ‘chignon’ within the cup. Axial traction in the line of the pelvic axis should be timed with uterine contractions and maternal pushing. A thumb should be placed on the cup, with the index finger on the scalp at the edge of the cup allowing the operator to feel any potential detachment before it is heard (by which point it is often too late to prevent detachment). Descent promotes auto‐rotation of the head to the OA position and episiotomy is often not required. Parents should be reassured that the ‘chignon’ will settle over 2–3 days. Manual rotation Manual rotation for persistent OP position is an alternative to IVD. The procedure requires insertion of one hand into the posterior vagina to encourage flexion and rotation. Careful patient selection is essential and the operator must ensure that effective analgesia is in place. The right hand is inserted for a left OP position (insert left hand for right OP). Four fingers are placed behind the fetal occiput to act as the ‘gutter’ on which the head will rotate, with the thumb placed alongside the anterior fontanelle. When the mother pushes with a contraction, the thumb applies pressure to flex the head and rotation to an OA position should occur with minimal effort. In a series ( N = 61) where OP position was managed in two groups, the spontaneous delivery rate increased from 27% to 77% in the group offered digital rotation ( P <0.0001) [17] . Complications of IVD In a Cochrane review of 32 studies ( N = 6597), forceps were less likely to fail to achieve a vaginal birth compared with ventouse (RR 0.65, 95% CI 0.45–0.94) [16] . Vaginal and perineal lacerations, including third‐ and fourth‐degree tears, are more common with forceps than with vacuum. Infra‐levator haematomas may occur occasionally and these should be drained if large or symptomatic. The risk of flatus incontinence or altered continence is also higher. Follow‐up of women who have had low or outlet IVD confirms normal physical and neourological outcomes for the vast majority of the newborn. In terms of neonatal outcome, cephalhaematoma is more common with vacuum but risk of facial injury is less. Facial and scalp abrasions are usually minor and heal in a few days. Unilateral facial nerve palsy is rare and resolves within days or weeks and is not usually related to poor technique. Skull fracture is rare and most need no treatment unless depressed, when surgical elevation may be indicated. Vacuum delivery may result in retinal haemorrhages, haematoma confined to one of the skull bones and neonatal jaundice. Severe scalp lacerations imply poor technique and are fortunately rare. Subgaleal haemorrhage may cause minor or severe morbidity and rarely mortality [18] . In reviewing morbidity associated with IVD, it is important to remember that the alternative option of second‐stage CS is also associated with increased morbidity for both mother and baby. Safe practice: sequential intrumentation and trial of instrumental delivery For all IVDs, the procedure should be abandoned if there is ‘no evidence of progressive descent with moderate traction during each contraction, or where delivery is not imminent following three contractions of a correctly applied instrument by an experienced operator’ [11] . Sequential instrumentation is associated with increased neonatal morbidity and the decision to proceed must take into account the relative risks of delivery by second‐stage CS from deep in the pelvis. It can be difficult to judge whether to proceed with IVD, especially in cases with mid‐cavity malposition at the level of the ischial spines. In such cases a trial of instrumental delivery should be undertaken in theatre under regional anaesthesia, with the full theatre team and neonatal practitioner present. The estimated incidence of trial of instrumental delivery is 2–5%. It is vital to maintain awareness of the situation, with a clear willingness to abandon the attempt if progress is not as expected, proceeding immediately to CS. The couple should be advised of this strategy and appropriate consent obtained prior to the procedure, which should be undertaken by the most senior obstetrician available. In the presence of fetal compromise, it is prudent to consider delivery by emergency CS, rather than proceeding with a potentially difficult IVD. Paired cord blood samples should be taken and results recorded after every attempted IVD. Contemporary developments in IVD New methods are being developed to achieve IVD and include disposable plastic forceps with the ability to measure traction force (see http://www.medipex.co.uk/success‐stories/pro‐nata‐yorkshire‐obstetric‐forceps/ and Fig. 26.10 ) and the Odon device where traction is applied using a plastic bag placed around the fetal head and neck. This device is undergoing trials led by the World Health Organization (see http://www.who.int/reproductivehealth/topics/maternal_perinatal/odon_device/en/ ). Fig. 26.10 Pro‐Nata Yorkshire obstetric forceps. Reproduced with permission of Mark Jessup.
Share this:
- Click to share on Twitter (Opens in new window)
- Click to share on Facebook (Opens in new window)
Related posts:
- Subfertility
- The Law and the Obstetrician and Gynaecologist
- Assisted Reproduction
- Ambulatory Gynaecology, Hysteroscopy and Laparoscopy
Stay updated, free articles. Join our Telegram channel
Comments are closed for this page.

Full access? Get Clinical Tree

Abnormal Fetal Position and Presentation
Under normal circumstances, a baby is in the vertex (cephalic) position before delivery. In the vertex position, the baby’s head is at the lower part of the abdomen, and the baby is born head-first. However, some babies present differently before delivery. In these cases, abnormal presentations may place the baby at risk of experiencing umbilical cord problems and/or a birth trauma (1). Types of abnormal fetal positions and presentations include the following. We’ll cover each in more detail on this page.
What is the difference between fetal presentation and position?
In the womb, a fetus has both a presentation and a position . Presentation refers to the baby’s body that leads, or is expected to lead, out of the birth canal (9). For example, if a baby’s rear is set to come out of the birth canal first, the baby is said to be in “breech presentation.” Position refers to the direction the baby is facing in relation to the mother’s spine (9). A baby could be lying face-first against a mother’s spine, or face up towards the mother’s belly.
What way should a baby come out during birth?
Vertex presentation is the ‘normal’ way that a baby is positioned for birth and the lowest-risk presentation for vaginal birth (1). In vertex presentation, the baby is positioned head-first with their occiput (the part of the head close to the base of the skull) entering the birth canal first. In this position, the baby’s chin is tucked into their chest and they are facing the mother’s back (occipito-anterior position). Any position other than vertex position is abnormal and can make vaginal delivery much more difficult or sometimes impossible (2). If a baby’s chin isn’t tucked into their chest, they may come out face-first (face presentation), which can cause birth injury (1).
What happens if a baby isn’t in the standard vertex position during birth?
Before delivery, it is critical that the fetus is in the standard vertex presentation and within the normal range for weight and size. This helps ensure the safety of both baby and mother during labor. When the baby’s size or position is abnormal, physician intervention is usually warranted (1). This may mean simple manual procedures to help reposition the baby or, in many cases, a planned C-section delivery . The failure of healthcare professionals to identify and quickly resolve issues related to fetal size, weight, and presentation is medical malpractice . There are numerous complications related to abnormal weight, size, abnormal position, or abnormal presentation.
Compound presentation
In the safest presentation (vertex presentation), the baby is born head first, with the rest of the body following. In a compound presentation, however, there are multiple presenting parts. Most commonly, this means that the baby’s head and an arm come out first at the same time. Sometimes compound presentation can occur with twins where the head of the first twin presents with the extremity of the second twin (3).
Risk factors for compound presentation include (3):
- Prematurity
- Intrauterine growth restriction (IUGR)
- Multiple gestations ( twins , triplets, etc.)
- Polyhydramnios
- A large pelvis
- External cephalic version
- Rupture of membranes at high station
Compound presentations can be detected via ultrasound before the mother’s water breaks. During labor, compound presentation is identified as an irregular finding during a cervical examination (3).
If a mother has polyhydramnios, the risk of compound presentation is higher, as the flow of amniotic fluid when the membranes rupture can sweep extremities into the birth canal, or cause a cord prolapse , which is a medical emergency (3). If compound presentation continues, it is likely to cause dystocia (the baby becoming stuck in the birth canal), which is also a medical emergency (3). Often, the safest way to deliver a baby with compound presentation is C-section, because complications like dystocia and cord prolapse carry risks of severe adverse outcomes, including cerebral palsy , intellectual and developmental disabilities, and hypoxic-ischemic encephalopathy (HIE) (3).
Limb presentation
Limb presentation during childbirth means that the part of the baby’s body that emerges first is a limb – an arm or a leg. Babies with limb presentation cannot be delivered safely via vaginal delivery; they must be delivered quickly by emergency C-section (4). Limb presentation poses a large risk for dystocia (the baby getting stuck on the mother’s pelvis), which is a medical emergency.
Occipitoposterior (OP) position
Approximately 1 out of 19 babies present in a posterior position rather than an anterior position. This is called an occipitoposterior (OP) position or occiput posterior position (3) In OP position, the baby is head-first with the back part of the head turned towards the mother’s back, rotated to the right (right occipitoposterior position, or ROP), or to the left (left occipitoposterior position, or LOP) of the sacroiliac joint. Occipitoposterior position increases the baby’s risk of experiencing prolonged labor , prolapsed umbilical cord , and use of delivery instruments, such as forceps and vacuum extractors (5). These conditions can cause brain bleeds , a lack of oxygen to the brain, and birth asphyxia .
When OP position is present, if a manual rotation cannot be quickly and effectively performed in the face of fetal distress, the baby should be delivered via C-section (5). A C-section can help prevent oxygen deprivation caused by prolonged labor, umbilical cord prolapse, or forceps and vacuum extractor use.
A nurse explains posterior position
Breech presentation
Breech presentation is normal throughout pregnancy. However, by the 37th week, the baby should turn to the cephalic position in time for labor. Breech presentation occurs when a baby’s buttocks or legs are positioned to descend the birth canal first. Breech positions are dangerous because when vaginal delivery is attempted, a baby is at increased risk for prolapsed umbilical cord, traumatic head injury, spinal cord fracture, fatality, and other serious problems with labor (6).
There are 4 types of breech positions:
- Footling breech presentation : In footling position, one or both feet enter the birth canal first, with the buttocks at a higher position than the feet.
- Kneeling breech presentation : This is when the baby has one or both legs extended at the hips and flexed at the knees.
- Frank breech presentation : This is when the baby’s buttocks present first, the legs are flexed at the hip and extended at the knees, and the feet are near the ears.
- Complete breech presentation : In this position, the baby’s hips and knees are flexed so that the baby is sitting cross-legged, with the feet beside the buttocks.
When a baby is in breech position, physicians often try to maneuver the baby into a head-first position. This should only be attempted if fetal heart tracings are normal (the baby is not in distress ) (7). The only type of breech position that may allow for a vaginal delivery is frank breech , and the following conditions must be met:
- The baby’s heart rate is being closely monitored and the baby is not in distress.
- Cephalopelvic disproportion (CPD) is not present; x-rays and ultrasound show that the size of the mother’s pelvis will allow a safe vaginal birth.
- The hospital is equipped for and the physician is skilled in performing an emergency C-section .
If these conditions are not present, vaginal birth should not be attempted. Most experts recommend C-section delivery for all types of breech positions because it is the safest method of delivery and it helps avoid birth injuries (6). Mismanaged breech birth can result in the following conditions:
- Brain bleeds, intracranial hemorrhages
- Spinal cord fractures
- Hypoxic-ischemic encephalopathy (HIE)
- Cerebral palsy
- Intellectual disabilities
- Developmental delays
Face presentation
A face presentation occurs when the face is the presenting part of the baby. In this position, the baby’s neck is deflexed (extended backward) so that the back of the head touches the baby’s back. This prevents head engagement and descent of the baby through the birth canal. In some cases of face presentation, the trauma of a vaginal delivery causes face deformation and fluid build-up (edema) in the face and upper airway, which often means the baby will need a breathing tube placed in the airway to maintain airway patency and assist breathing (1).
Image by healthhand.com
There are three types of face presentation:
- Mentum anterior (MA) : In this position, the chin is facing the front of the mother.
- Mentum posterior (MP) : The chin is facing the mother’s back, pointing down towards her buttocks in mentum posterior position. In this position, the baby’s head, neck, and shoulders enter the pelvis at the same time, and the pelvis is usually not large enough to accommodate this. Also, an open fetal mouth can push against the bone (sacrum) at the upper and back part of the pelvis, which also can prevent descent of the baby through the birth canal.
- Mentum transverse (MT) : The baby’s chin is facing the side of the birth canal in this position.
Trauma is very common during vaginal delivery of a baby in face presentation, so parents must be warned that their baby may be bruised and that a C-section is available to avoid this trauma.
Babies presenting face-first can sometimes be delivered vaginally, as long as the baby is in MA position (1). Safe vaginal delivery of a term-sized infant in persistent MP position is impossible due to the presenting part of the baby compared to the size of the mother’s pelvis (1). Babies in MP position must be delivered by C-section. Babies in MT position must also be delivered by C-section. Some babies in the MP and MT positions will spontaneously convert to the MA position during the course of labor, which makes vaginal delivery a possibility. If the baby is in the MA position and vaginal delivery is able to proceed, engagement of the presenting part of the baby probably will not occur until the face is at a +2 station (1).
The management of face presentation requires close observation of the progress of labor due to the high incidence of CPD with face presentation. In face presentation, the diameter of the presenting part of the head is, on average, 0.7 cm greater than in the normal vertex position (1).
In any face presentation situation, if progress in dilation and descent ceases despite adequate contractions, delivery must occur by C-section. In fact, when face presentation occurs, experts recommend liberal use of C-section (1).
Since there is an increased risk of trauma to the baby when the face presents, the physician should not try to rotate the baby internally. In addition, the physician must not use vacuum extractors or manual extraction (grasping the baby with hands) to extract the baby from the uterine cavity. Outlet forceps should only be used by experienced physicians; these forceps increase the risk of trauma and brain bleeds. In almost all clinical circumstances a cesarean delivery is the safest method of delivery.
Listed below are complications that can occur if face presentation is mismanaged by the medical team:
- Prolonged labor
- Facial trauma
- Facial and upper airway edema (fluid build-up in the face, often caused by trauma)
- Skull molding (abnormal head shape that results from pressure on the baby’s head during childbirth)
- Respiratory distress or difficulty in ventilation (the baby being able to move air in and out of lungs) due to upper airway trauma and edema
- Spinal cord injury
- Abnormal fetal heart rate patterns
- 10-fold increase in fetal compromise
- Brain bleeds
- Intracranial hemorrhages
- Permanent brain damage
Brow presentation
Brow presentation is similar to face presentation, but the baby’s neck is less extended. A fetus in brow presentation has the chin untucked, and the neck is extended slightly backward. As the term “brow presentation” suggests, the brow (forehead) is the part that is situated to go through the pelvis first. Vaginal delivery can be difficult or impossible with brow presentation, because the diameter of the presenting part of the head may be too big to safely fit through the pelvis.
Risk factors and conditions associated with brow presentation
Brow presentation has been linked to several risk factors and co-occurring conditions. These include:
- Multiparity (having previously given birth)
- Premature delivery
- Fetal anomalies such as anencephaly (an absence of major parts of the brain and skull) or anterior neck mass (a growth on the front of the neck)
- Previous c-section delivery
- Polyhydramnios (excessive amniotic fluid: infants swallow amniotic fluid while in utero, but this may be difficult if their neck is extended)
Diagnosis of brow presentation
Brow presentation can often be diagnosed through a vaginal examination during labor. If there are no conclusive signs from the physical examination alone, an ultrasound can also be used. Warning signs of brow presentation may include signs of fetal distress or lack of labor progression.
Management of brow presentation
Infants who assume a brow presentation early in labor may spontaneously move into a more optimal position during the delivery process. Additionally, safe delivery in brow presentation may be possible if the infant is unusually small and/or the mother’s pelvic opening is unusually large. For these reasons, physicians occasionally recommend vaginal delivery of infants in brow presentation.
Doctors attempting vaginal delivery of a baby in brow presentation must be very careful to watch for signs of fetal distress (such as an abnormal heart rate), and to monitor the progression of labor. Prolonged labor can cause extended periods of fetal oxygen deprivation, which can cause birth asphyxia and permanent injury. Signs of fetal distress can indicate that a baby is in danger of sustaining serious brain damage if action is not quickly taken to prevent this. If an infant in brow presentation begins to show signs of distress, or if labor progress stops or slows significantly, physicians should be ready to move on to a cesarean delivery.
Labor induction or augmentation with the drug Pitocin (synthetic oxytocin) is very dangerous in cases of brow presentation. Pitocin can lead to excessive uterine contractions, which can put pressure on the infant’s head and cut off their oxygen supply; this is especially risky when safe fetal descent is already compromised, such as in cases of brow presentation.
Complications of brow presentation
If brow presentation is diagnosed in a timely fashion and is appropriately managed, there are typically no serious negative effects on the mother or baby. However, if medical professionals fail to recognize brow presentation and intervene as necessary, there can be lasting consequences. Infants may suffer oxygen deprivation due to prolonged labor, or traumatic injuries from a difficult delivery. Some of the most severe conditions resulting from mismanaged brow presentation births include:
- Hypoxic-ischemic encephalopathy
- Periventricular leukomalacia
- Seizure disorders
- Developmental disabilities
Shoulder presentation (transverse lie)
Shoulder presentation (transverse lie) is when the arm, shoulder or trunk of the baby enter the birth canal first. When a baby is in a transverse lie position during labor, C-section is almost always used as the delivery method (8). Mothers who have polyhydramnios (too much amniotic fluid), are pregnant with more than one baby, have placenta previa, or have a baby with intrauterine growth restriction (IUGR) are more likely to have a baby in the transverse lie position (8). Once the membranes rupture, there is an increased risk of umbilical cord prolapse in this position; thus, a C-section should ideally be performed before the membranes break (8). Failure to quickly deliver the baby by C-section when transverse lie presentation is present can cause severe birth asphyxia due to cord compression and trauma to the baby. This can cause hypoxic-ischemic encephalopathy (HIE), seizures, permanent brain damage, and cerebral palsy.
Legal help for birth injuries from abnormal position or presentation
The award-winning birth injury attorneys at ABC Law Centers: Birth Injury Lawyers have over 100 years of joint experience handling birth trauma cases related to abnormal position or presentation. If you believe your loved one’s birth injury resulted from an instance of medical malpractice, you may be entitled to compensation from a medical malpractice or personal injury case. During your free legal consultation, our birth injury attorneys will discuss your case with you, determine if negligence caused your loved one’s injuries, identify the negligent party, and discuss your legal options with you.
- Free Case Review
- Available 24/7
- No Fee Unless We Win
Featured Videos
Testimonial from keziah’s family, posterior position, hypoxic-ischemic encephalopathy (hie).
Featured Testimonial
What Our Clients Say…
After the traumatic birth of my son, I was left confused, afraid, and seeking answers. We needed someone we could trust and depend on . ABC Law Centers: Birth Injury Lawyers was just that.
Helpful resources
More about our firm.
- Meet our birth injury attorneys
- Meet our in-house medical staff
- Verdicts and settlements
- Testimonials
- Julien, S., and Galerneau, F. (2017). Face and brow presentations in labor. Retrieved from https://www.uptodate.com/contents/face-and-brow-presentations-in-labor .
- World Health Organization, UNICEF, and United Nations Population Fund. Malpositions and malpresentations. Retrieved from http://hetv.org/resources/reproductive-health/impac/Symptoms/Malpositions__malpresetations_S69_S81.html .
- Barth, W. (2016). Compound fetal presentation. Retrieved from https://www.uptodate.com/contents/compound-fetal-presentation .
- Gabbe, S.G., … Grobman, W.A. (2017). Compound Presentation. Retrieved from https://expertconsult.inkling.com/read/gabbe-obstetrics-normal-problem-pregnancies-7e/chapter-17/compound-presentation .
- Argani, C.H. and Satin, A.J. (2018) Occiput posterior position. Retrieved from https://www.uptodate.com/contents/occiput-posterior-position .
- Hofmeyr, G.J. (2018). Overview of issues related to breech presentation. Retrieved from https://www.uptodate.com/contents/overview-of-issues-related-to-breech-presentation .
- Hofmeyr, G.J. (2017). Delivery of the fetus in breech presentation. Retrieved from https://www.uptodate.com/contents/delivery-of-the-fetus-in-breech-presentation .
- Strauss, R.A. (2017). Transverse fetal lie. Retrieved from https://www.uptodate.com/contents/transverse-fetal-lie .
- Moldenhauer, J.S. (2018). Abnormal Position and Presentation of the Fetus. Retrieved from https://www.merckmanuals.com/home/women-s-health-issues/complications-of-labor-and-delivery/abnormal-position-and-presentation-of-the-fetus .
Over $350 Million Recovered
In Verdicts, Settlements, & Judgements
$4.75 Million
$3.9 Million
$5.85 Million
Awards & Memberships
- The Open University
- Explore OpenLearn
- Get started
- Create a course
- Free courses
- Collections
My OpenLearn Create Profile
- Personalise your OpenLearn profile
- Save Your favourite content
- Get recognition for your learning
Already Registered?
- Antenatal Care Module: Ethiopian Federal Ministry of Health
- Labour and Delivery Care Module: Acknowledgements
- Labour and Delivery Care Module: Introduction
- Labour Delivery and Care Module: 1. Recognition of Normal Labour
- Labour and Delivery Care Module: 2. Assessing the Woman in Labour
- Labour Delivery and Care Module: 3. Care of the Woman in Labour
- Labour and Delivery Care Module: 4. Using the Partograph
- Labour and Delivery Care Module: 5. Conducting a Normal Delivery
- Labour and Delivery Care Module: 6. Active Management of the Third Stage of Labour
- Labour and Delivery Care Module: 7. Neonatal Resuscitation
- Introduction
- Learning Outcomes for Study Session 8
- 8.1.1 Vertex presentation
- 8.1.2 Malpresentations
- 8.1.3 Malposition
- 8.2 Causes and consequences of malpresentations and malpositions
- 8.3.1 Causes of breech presentation
- 8.3.2 Diagnosis of breech presentation
- 8.3.3 Types of breech presentation
- 8.3.4 Risks of breech presentation
- 8.4.1 Causes of face presentation
- 8.4.2 Diagnosis of face presentation
- 8.4.3 Complications of face presentation
- 8.5.1 Possible causes of brow presentation
- 8.5.2 Diagnosis of brow presentation
- 8.5.3 Complications of brow presentation
- 8.6.1 Causes of shoulder presentation
8.6.2 Diagnosis of shoulder presentation
8.6.3 Complications of shoulder presentation
- 8.7.1 Types of twin pregnancy
- 8.7.2 Diagnosis of twin pregnancy
- 8.7.3 Consequences of twin pregnancy
- 8.8 Management of women with malpresentation or multiple pregnancy
- Summary of Study Session 8
- Self-Assessment Questions (SAQs) for Study Session 8
- Labour and Delivery Care Module: 9. Obstructed Labour
- Labour and Delivery Care Module: 10. Ruptured Uterus
- Labour and Delivery Care Module: 11. Postpartum Haemorrhage
- Download PDF version
- Labour and Delivery Care PDF (4MB)
Download this course
Download this course for use offline or for other devices.
The materials below are provided for offline use for your convenience and are not tracked. If you wish to save your progress, please go through the online version.
About this course
- 26 hours study
- 1 Level 1: Introductory
- Course description

Labour and Delivery Care
If you create an account, you can set up a personal learning profile on the site.
Complications include:
- Cord prolapse
- Trauma to a prolapsed arm
- Obstructed labour and ruptured uterus
- Fetal hypoxia and death.
Remember that a shoulder presentation means the baby cannot be born through the vagina; if you detect it in a woman who is already in labour, refer her urgently to a higher health facility.
8.7 Multiple pregnancy
For further information, take a look at our frequently asked questions which may give you the support you need.
Have a question?
If you have any concerns about anything on this site please get in contact with us here.
Report a concern

Military Obstetrics & Gynecology – 3rd Edition
Fetal presentation.
Fetal presentation means the part of the fetus that is “presenting” at the cervix:
- Cephalic presentation means head first. This is the normal presentation.
- Breech presentation means the fetal butt is coming out first.
- Transverse lie means the fetus is oriented from one side of the mother to the other and neither the head nor the butt is coming out first.
- Compound presentation means that a fetal hand is coming out with the fetal head.
- Shoulder presentation means that the fetal shoulder is trying to come out first.
Fetal “presentation” is different from fetal “position.” Fetal position refers to the orientation of the fetus within the birth canal (eg, looking toward the mother’s pubic bone (OP), or look toward the mother’s coccyx (OA), etc.)

Breech Presentation
Frank breech means the buttocks are presenting and the legs are up along the fetal chest. The fetal feet are next to the fetal face. This is the safest arrangement for breech delivery.
Footling breech means either one foot (“Single Footling”) or both feet (“Double Footling”) is presenting. This is also known as an incomplete breech.

Complete breech means the fetal thighs are flexed along the fetal abdomen, but the fetal shins and feet are tucked under the legs. The buttocks is presenting first, but the feet are very close. Sometimes during labor, a complete breech will shift to an incomplete breech if one or both of the feet extend below the fetal buttocks.
While many breech fetuses deliver vaginally without incident, this presentation is associated with an increased risk of:
- Fetal mechanical injury (fractures, nerve damage, and soft tissue injuries)
- Fetal asphyxia due to umbilical cord prolapse and obstruction, and fetal head entrapment.
For these reasons, many breech babies are delivered by cesarean section, and some obstetricians feel that all breech babies should be delivered in this way.
Transverse Lie
If the fetus remains in a transverse lie, it cannot deliver deliver vaginally as the diameter of the fetal presenting part (the whole body, in this case) cannot descend through the birth canal.

If labor is allowed to continue for enough time with the fetus in transverse lie, the uterus will rupture. Even before the uterus ruptures, there is an increased risk in this presentation for prolapsed umbilical cord. For these reasons, women found to have a transverse lie in labor will usually have a cesarean section.
There are some exceptions to this indication for cesarean section:
- If labor is occurring during the middle trimester and fetus is not considered viable, it may be possible for this very small and fragile fetus to compress enough to squeeze through the pelvis. In this case, fetal survival would not be an issue.
- It may be possible to perform an external version, during which you manipulate the fetus, converting it to either breech or cephalic presentation. This is often more difficult than it sounds, particularly during labor, and carries some risk of injury to the fetus, placenta, umbilical cord, or uterus.
- In the case of twins, it would be acceptable to allow labor, even though the second twin is in transverse lie, anticipating that after delivery of the first twin, you would reach in and perform an internal version, converting the transverse lie to cephalic or breech presentation prior to delivery.
Some predisposing factors for a transverse lie include:
- Grand multiparity – more than 5 term pregnancies.
- Placenta previa
- Bony abnormalities of the pelvis
- Pelvic kidney
- Other pelvic mass
Transverse lie occurs frequently in early pregnancy, when it is of no consequence. At 16 weeks gestation, about half of all pregnancies will be transverse lie. This number steadily falls as pregnancy advances and the incidence of transverse lie by the 28th week is well below 10%. It falls steadily thereafter.
Whenever a fetal transverse lie is encountered near term or in labor, evaluate the patient carefully with ultrasound to determine if there are any predisposing factors, such as a placenta previa or pelvic kidney that could modify your management of the patient. So long as a placenta previa is not present, many obstetricians will check the patient’s cervix at frequent intervals to detect early cervical dilatation and the consequential increased risk of cord prolapse. Sometimes, these patients are delivered early by scheduled cesarean section to avoid that risk.
Compound Presentation
Compound presentation means that a fetal hand is coming out with the fetal head. This is a problem because:
- The amount of baby that must come through the birth canal at one time is increased.
- There is increased risk of mechanical injury to the arm and shoulder, including fractures, nerve injuries and soft tissue injury.

A compound presentation may be resolvable if the fetus can be encouraged to withdraw the hand, for example.
If the fetus and arm are relatively small in comparison to the maternal pelvis, vaginal delivery may still be possible, but with some risk of injury to the arm.
If the fetus and arm are relatively large in comparison to the maternal pelvis, obstructed labor will occur and a cesarean will be needed.
Shoulder presentation
Shoulder presentation means that the fetal shoulder is trying to come out first. This is a more advanced form of transverse lie and is undeliverable vaginally.
In military settings, position and presentation can be made by:
- Pelvic Exam
- Abdominal Exam (Leopold’s Maneuvers)
- Single x-ray of the abdomen
- Ultrasound if available.
Women's Healthcare in Operational Settings
- Patient Care & Health Information
- Diseases & Conditions
- Frozen shoulder

Frozen shoulder occurs when the connective tissue enclosing the joint thickens and tightens.
Frozen shoulder, also called adhesive capsulitis, involves stiffness and pain in the shoulder joint. Signs and symptoms typically begin slowly, then get worse. Over time, symptoms get better, usually within 1 to 3 years.
Having to keep a shoulder still for a long period increases the risk of developing frozen shoulder. This might happen after having surgery or breaking an arm.
Treatment for frozen shoulder involves range-of-motion exercises. Sometimes treatment involves corticosteroids and numbing medications injected into the joint. Rarely, arthroscopic surgery is needed to loosen the joint capsule so that it can move more freely.
It's unusual for frozen shoulder to recur in the same shoulder. But some people can develop it in the other shoulder, usually within five years.
Products & Services
- A Book: Mayo Clinic Family Health Book
- Mayo Clinic Sports Medicine
- Newsletter: Mayo Clinic Health Letter — Digital Edition
- Products for Daily Living from Mayo Clinic Store
Frozen shoulder typically develops slowly in three stages.
- Freezing stage. Any movement of the shoulder causes pain, and the shoulder's ability to move becomes limited. This stage lasts from 2 to 9 months.
- Frozen stage. Pain might lessen during this stage. However, the shoulder becomes stiffer. Using it becomes more difficult. This stage lasts from 4 to 12 months.
- Thawing stage. The shoulder's ability to move begins to improve. This stage lasts from 5 to 24 months.
For some people, the pain worsens at night, sometimes disrupting sleep.
There is a problem with information submitted for this request. Review/update the information highlighted below and resubmit the form.
From Mayo Clinic to your inbox
Sign up for free and stay up to date on research advancements, health tips, current health topics, and expertise on managing health. Click here for an email preview.
Error Email field is required
Error Include a valid email address
To provide you with the most relevant and helpful information, and understand which information is beneficial, we may combine your email and website usage information with other information we have about you. If you are a Mayo Clinic patient, this could include protected health information. If we combine this information with your protected health information, we will treat all of that information as protected health information and will only use or disclose that information as set forth in our notice of privacy practices. You may opt-out of email communications at any time by clicking on the unsubscribe link in the e-mail.
Thank you for subscribing!
You'll soon start receiving the latest Mayo Clinic health information you requested in your inbox.
Sorry something went wrong with your subscription
Please, try again in a couple of minutes
The shoulder joint is enclosed in a capsule of connective tissue. Frozen shoulder occurs when this capsule thickens and tightens around the shoulder joint, restricting its movement.
It's unclear why this happens to some people. But it's more likely to happen after keeping a shoulder still for a long period, such as after surgery or an arm fracture.
Risk factors
Certain factors may increase the risk of developing frozen shoulder.
Age and sex
People 40 and older, particularly women, are more likely to have frozen shoulder.
Immobility or reduced mobility
People who've had to keep a shoulder somewhat still are at higher risk of developing frozen shoulder. Restricted movement can be the result of many factors, including:
- Rotator cuff injury
- Recovery from surgery
Systemic diseases
People who have certain diseases appear more likely to develop frozen shoulder. Diseases that might increase risk include:
- Overactive thyroid (hyperthyroidism)
- Underactive thyroid (hypothyroidism)
- Cardiovascular disease
- Parkinson's disease
One of the most common causes of frozen shoulder is not moving a shoulder while recovering from a shoulder injury, broken arm or stroke. If you've had an injury that makes it difficult to move your shoulder, talk to your health care provider about exercises that can help you maintain your ability to move your shoulder joint.
- McMahon PJ, et al., eds. Sports medicine: Upper extremity. In: Current Diagnosis & Treatment in Orthopedics. 6th ed. McGraw Hill; 2021. https://accessmedicine.mhmedical.com. Accessed June 18, 2022.
- Frozen shoulder. American Academy of Orthopaedic Surgeons. https://orthoinfo.aaos.org/en/diseases--conditions/frozen-shoulder. Accessed June 14, 2022.
- Prestgaard TA. Frozen shoulder (adhesive capsulitis). https://www.uptodate.com/contents/search. Accessed June 14, 2022.
- Challoumas D, et al. Comparison of treatments for frozen shoulder: A systematic review and meta-analysis. JAMA Network Open. 2020; doi:10.1001/jamanetworkopen.2020.29581.
- Kim YJ. Acupuncture management for acute frozen shoulder: A case report. Clinical Case Reports. 2021; doi:10.1002/ccr3.5055.
- Shoulder exercises
Associated Procedures
- Cortisone shots
News from Mayo Clinic
- Mayo Clinic Minute: Tips to help a frozen shoulder Dec. 06, 2023, 06:01 p.m. CDT
- Symptoms & causes
- Diagnosis & treatment
- Doctors & departments
Mayo Clinic does not endorse companies or products. Advertising revenue supports our not-for-profit mission.
- Opportunities
Mayo Clinic Press
Check out these best-sellers and special offers on books and newsletters from Mayo Clinic Press .
- Mayo Clinic on Incontinence - Mayo Clinic Press Mayo Clinic on Incontinence
- The Essential Diabetes Book - Mayo Clinic Press The Essential Diabetes Book
- Mayo Clinic on Hearing and Balance - Mayo Clinic Press Mayo Clinic on Hearing and Balance
- FREE Mayo Clinic Diet Assessment - Mayo Clinic Press FREE Mayo Clinic Diet Assessment
- Mayo Clinic Health Letter - FREE book - Mayo Clinic Press Mayo Clinic Health Letter - FREE book
Your gift holds great power – donate today!
Make your tax-deductible gift and be part of the cutting-edge research and care that's changing medicine.

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- Future Sci OA
- v.6(10); 2020 Dec
Frozen shoulder: overview of clinical presentation and review of the current evidence base for management strategies
Akshay date.
1 Department of Orthopaedics, Basildon & Thurrock University Hospital, Nethermayne, Basildon, Essex, UK, SS16 5NL, UK
Luthfur Rahman
2 Department of Orthopaedics, Chelsea & Westminster Hospital, 369 Fulham Rd, Chelsea, London SW10 9NH, UK
Adhesive capsulitis of the shoulder (ACS) is a condition with significant clinical and economic implications. The etiology of adhesive capsulitis is not clearly understood and there remains lack of consensus in clinical management for this condition. It can occur as a primary idiopathic condition or secondary to medical conditions or trauma. The hallmarks of ACS are pain and stiffness, caused by formation of adhesive or scar tissue in the glenohumeral joint. Management strategies vary depending on stage of presentation, patient factors and clinician preferences, and can range from conservative options to surgical intervention. The aim of this review is to summarize the pathophysiology and clinical presentation of ACS and to discuss the evidence base for various management strategies employed today.
Lay abstract
Frozen shoulder (FS) is a relatively common condition characterized by pain and stiffness of the shoulder joint. The exact cause of primary FS is unknown and in some patients the condition can persist for several years. Treatment strategies vary depending on stage of presentation, patient factors and clinician preferences. This review gives a summary of the clinical presentation of FS and an overview of the current evidence for both surgical and conservative treatment options for the condition.
Adhesive capsulitis of the shoulder (ACS) was first described by Duplay [ 1 ] in 1872 as ‘periarthritis’ and subsequently by Codman [ 2 ], who coined the term ‘frozen shoulder’ in 1934 [ 3 ]. ACS is characterized by varying degrees of pain and restricted movements of the glenohumeral joint. It occurs in approximately 2–5% of the population with a peak incidence between 40 and 70 years of age. It is more common in females and bilateral in 20–30% of cases. The condition is usually self-limiting; however, in some patients, symptoms can last for several years or may never fully resolve [ 4 ]. Treatment for ACS remains a challenge today, placing a significant burden on healthcare systems as well as the wider economy, with patients unable to work for prolonged periods of time. This review article aims to give a brief overview of the pathophysiology and clinical presentation of ACS and to summarize the evidence base for conservative and surgical management of the condition [ 5 ].
Pathophysiology & clinical presentation
Adhesive capsulitis can be either primary or secondary; secondary causes of ACS include trauma, previous shoulder surgery, prolonged immobilization [ 6 ], diabetes [ 7 ], thyroid disease [ 8 ], Dupuytren disease [ 9 ] and other autoimmune disorders [ 10 ]. Primary idiopathic frozen shoulder occurs in patients presenting with painful, restricted shoulder movements where no underlying cause is found. The pathophysiology of primary adhesive capsulitis is still not fully understood, but histological studies have shown that frozen shoulder is characterized by a thickened, tight capsule, with chronic inflammatory cells and fibroblasts found in the joint capsule [ 11 ] Furthermore, fibroblasts in frozen shoulder have an activated phenotype associated with cytokine dysregulation, suggesting an autoimmune etiology [ 12 , 13 ].
Clinically, four stages of adhesive capsulitis have been described as a useful method of monitoring and assessing symptomatology [ 14 ] [ Table 1 ]. The condition starts with a painful phase, characterized by pain and progressive restriction of movement. This phase is characterized by hypertrophic synovitis with hypervascularity, but a normal appearance of the capsular tissue [ 15 ]. This is followed by a ‘freezing’ stage where symptoms gradually worsen over 9 months; histologically, there is perivascular synovitis and collagen deposition. Over the subsequent 1–4 months, the ‘frozen’ phase occurs, characterized by stiffness as a predominating symptom. The ‘thawing’ phase, in which symptoms resolve, has the greatest variability in duration and can last for up to 2 years. The latter two stages involve the formation of dense collagenous tissue in the capsule, associated with scar formation [ 15 ].
Table 1.
| Stage | Symptoms | Duration of symptoms (months) | Histology | |
|---|---|---|---|---|
| I | Painful stage | Moderate pain and reduction of movement | <3 | Hypertrophic synovitis with hypervascularity Normal capsular tissue |
| II | Freezing stage | Severe pain and reduction of movement | 3–9 | Perivascular synovitis and disorganized collagen deposition and scarring |
| III | Frozen stage | Pain may be present but stiffness predominates | 10–14 | Dense and hypercellular collagenous tissue of the capsule |
| IV | Thawing stage | Minimal pain and gradual improvement in movement | 14–24 | Fully developed scar tissue Pathophysiology remains unclear |
There is significant variation in clinical practice and the disease course may not follow such a stepwise progression. The diagnosis is usually made clinically, with pain and stiffness as the hallmark of the condition. The onset of pain is often gradual over a period of months, with night pain being a common feature. The pain may be poorly localized and described as a deep ache, or sometimes presents as a pain referred to the deltoid origin, radiating to the biceps area. Examination findings are often nonspecific without any point tenderness and with normal rotator cuff strength. However, both passive and active range of motion (ROM) are globally reduced; this is best assessed through passive external rotation with the arm by the side. The results of laboratory tests are usually normal but may be useful in identifying underlying conditions, such as diabetes or thyroid disease. Plain radiographs of the shoulder are also usually normal but can help diagnose or exclude other conditions, such as calcific tendinopathy of the rotator cuff, glenohumeral arthritis, acromioclavicular arthritis or even a shoulder dislocation. In calcific tendinopathy, disuse osteopenia may be demonstrated on the plain radiographs. Imaging modalities such as arthrography, technetium bone scans [ 16 ] and magnetic resonance imaging [ 17 ] are not routinely indicated or helpful in evaluation of adhesive capsulitis but can be used to exclude other shoulder pathology [ 18 ].
The goal of treatment in ACS is to restore function and manage symptoms. The choice of treatment can vary with patient factors, stage at presentation, clinician preferences and local policies or funding. Nonsurgical or conservative management is the preferred choice of treatment, with most patients usually improving in 6–18 months [ 19 ]. Conservative treatment options include analgesics, oral steroids, physical therapies, hydrodilatation, suprascapular nerve block (SNB) and intra-articular steroid or sodium hyaluronate injections. Surgical treatment is offered to patients with persistent symptoms despite conservative management; strategies include manipulation under anesthesia (MUA), arthroscopic release and open release. There remains no consensus or high-level evidence to definitively support one treatment modality over another.
Nonsurgical treatment
Physical therapy.
Physical therapy has traditionally been the initial treatment modality in ACS and it is often utilized alongside other adjuncts, including steroid injections, transcutaneous electrical nerve stimulation, analgesics and warm or cold pads [ 20 , 21 ]. There remains variation of physical therapy regimen in both clinical practice and in the literature; however, the principles revolve around a supervised stretching and strength maintenance program [ 22 , 23 ]. In the early freezing stage, gentle stretching exercises of short duration are recommended, including pendulum exercises and passive external supine forward elevation [ 24 ]. Strengthening exercises such as isometric shoulder external rotation and posterior capsular stretching can be introduced in the frozen stage [ 24 ]. In the thawing stages, both strengthening and stretching exercises can be combined and increased in frequency, or combined with Maitland Grade III–IV mobilization, to improve ROM. Griggs et al. , in a prospective nonrandomized study of 75 patients, showed that a supervised stretching program resulted in a satisfactory outcome in 90% of patients at 22 months [ 25 ]. Vermeulen et al. [ 26 ] showed that high-grade mobilization (working through the pain barrier) was marginally better than low-grade mobilization (working within pain limits).
Despite the clinically prevalent use of physical therapy in ACS, there remains a lack of high-level evidence to support physical therapy over observation or medical therapy alone [ 18 , 27 ]. Randomized controlled trials (RCTs) by Bulgen et al. [ 28 ] and later by Carette et al. [ 29 ] showed no significant difference between patients who had physical therapy and those receiving no treatment. Further research is required to determine the role for physical therapy and adjuncts to treatment in ACS management.
Pharmacological treatments
Paracetamol and NSAIDs are often used as first-line treatments for pain in adhesive capsulitis. Analgesics may be more effective when combined with physical therapy [ 20 ] and although NSAIDs have been shown in some studies to provide significant improvement of symptoms compared with placebo [ 30 ], there is no high-level evidence to support this. Studies comparing different NSAIDs including naproxen and indomethicin have shown no significant differences in their effect [ 31 , 32 ].
Oral steroids have also been shown to have benefit in ACS; Buchbinder et al. [ 33 ] showed in a double-blind, placebo-controlled RCT that patients taking 30 mg oral prednisolone daily as a 3-week course had greater improvement in disability, range of active motion and overall pain compared with placebo groups (p = 0.001). However, there was no significant difference between the groups beyond 6 weeks; the authors recommended prednisolone for its short-term benefits. Similar findings were reported by Binder et al. [ 34 ], who showed in a study of 40 patients that night pain significantly improved in patients receiving oral prednisolone over the short term, but that there were no differences between groups at 8 months. There may be a role for oral steroids in ACS in providing short-term pain relief and ROM improvement; however, clinicians should exercise caution with the long-term use of steroids due to the high side effects profile and limited evidence in the literature to support their use in ACS for a prolonged period.
Intra-articular steroid injections
Intra-articular steroid injections are routinely used in the management of ACS and have been shown to provide better short-term pain relief and improved movement compared with oral steroids [ 35 , 36 ] A recent meta-analysis with 225 patients showed that intra-articular steroid injections provided short-term analgesia (reduced pain score up to 8 weeks) and improved passive ROM in both short and long term (up to 24 weeks), compared with control groups receiving placebo [ 37 ]. Furthermore, a systematic review identified three high-quality RCTs showing a significant analgesic benefit of intra-articular injections, given between 6 weeks and 4 months, over placebo or physiotherapy alone [ 38 ]. Shah et al. reported that multiple injections are efficacious without causing significant complications [ 39 ]. Ultrasound-guided injections may be preferred because injections without radiological guidance have a high incidence of not entering the glenohumeral joint [ 40 , 41 ]. However, recent evidence also suggests there may be no significant difference in outcomes between subacromial and glenohumeral injection [ 42 , 43 ].
There is substantial high-level evidence in the literature comparing steroid injections with physiotherapy. Koh et al. , in a systematic review of RCTs, report corticosteroid injections as superior to placebo and physiotherapy in the short term (12 weeks) [ 43 ] Furthermore, a meta-analysis of nine RCTs with 453 patients found steroid injections equally as effective as physiotherapy; the authors recommend single steroid injection as the first line treatment in ACS [ 44 ]. However, several other RCTs have shown that steroid injections used as adjuncts to physiotherapy provide greater improvement in symptoms when compared with physical therapy alone [ 29 , 45 , 46 ].
Intra-articular sodium hyaluronate injections
Sodium hyaluronate can be used as an alternative to steroid injections [ 47 ] or indeed combined with steroids for the treatment of adhesive capsulitis [ 48 ]. A systematic review of seven studies with 140 ACS patients treated with hyaluronate injections showed hyaluronate to be better than placebo and as effective as corticosteroid injections, with the added benefit of fewer side effects [ 49 ]. In addition, it has been suggested that sodium hyaluronate may have a chondroprotective effect and improve the properties of synovial fluid [ 50 ]. A randomized study of 30 patients found tramadol with hyaluronate to be more effective than hyaluronate injections alone [ 51 ]. However, there remains controversy in the literature, with Lee et al. showing in their review of four RCTs including 273 patients that intra-articular hyaluronate was not superior to corticosteroid injection or physical therapy [ 52 ].
Hydrodilatation
Intra-articular distension of the shoulder joint is an alternative method of treatment which has been shown to be of benefit but predominantly in the short term and has not been shown to have any significant benefit in the long term over other treatment modalities. The technique involves dilation of the capsule with either saline or steroid and local anesthetic in an attempt to stretch the capsule and break down any adhesions [ 53 ]. Quraishi et al. [ 54 ], in a randomized trial of 36 patients, compared hydrodilatation with manipulation under anesthetic and demonstrated improved functional scores over a six-month period (p = 0.02) in the hydrodilatation group. There was improvement but not statistical significance in ROM at 6 months in both groups.
Three RCTs have compared hydrodilatation with intra-articular steroid injection. Gam et al. [ 55 ] reported a significant improvement in ROM in the hydrodilatation group but pain and functional scores were comparable; ROM is not a validated outcome for ACS and the findings from this study should be interpreted with caution. Similarly, Tveita et al. [ 56 ] and Corbeil et al. [ 57 ] found no difference in outcomes of pain and ROM. In addition, one study by Khan et al. [ 58 ] compared hydrodilatation with physical therapy; ROM for abduction and external rotation was significantly improved at 8 weeks with hydrodilatation and physiotherapy compared with physiotherapy alone. However, once again there was no significant improvement demonstrated in pain score. The studies described here were limited by sample size and randomization, and the heterogeneity of study design makes it difficult to draw confident conclusions [ 55–58 ]. There is insufficient evidence in the literature to suggest hydrodilatation as superior to other treatment modalities in ACS.
Suprascapular nerve block
The supraclavicular nerve arises from the superior trunk of the brachial plexus (C5, C6) and supplies the muscles of the rotator cuff, namely the supraspinatus and the infraspinatus. SNB involves local anesthetic infiltration through a needle inserted behind the lateral end of the clavicle at the insertion of the trapezius [ 59 ]. The effectiveness of SNB may be improved using electromyographic or ultrasound guidance [ 60–62 ]. In a double-blind, placebo-controlled RCT of 34 patients, Dahan et al. [ 63 ] demonstrated a significantly greater improvement in pain (p = 0.03) but no difference in function (p = 0.24) after SNB with bupivacaine compared with placebo at 1 month. Similarly, Jones et al. performed a prospective RCT and showed that SNB may also provide quicker and more complete resolution of symptoms compared with intra-articular steroid injections [ 62 ]. Mortada et al. showed in their trial of 96 patients that a course of nine injections gave a better outcome than a single injection [ 64 ]. The literature suggests that SNB could be an effective short-term strategy in ACS, although larger multicenter trials would be useful in further defining its role.
Surgical treatment
Manipulation under anesthesia.
Surgical treatments are usually reserved for patients who have persistent symptoms despite nonoperative treatment for between 2 and 6 months [ 65–67 ]. Manipulation of the shoulder is a technique in which the patient is anesthetized and the joint is manipulated to break down thickened and stiff capsular tissue. MUA has been shown to have good results in both the short and the long term, particularly when followed with a program of physical therapy [ 68 , 69 ]. MUA may also be combined with interscalene blocks, which have been shown to provide a sustained improvement in both function and movement at 12 months [ 70 ]. Furthermore, Farrell et al. demonstrated long-term improvements up to 15 years after MUA [ 71 ].
There are, however, significant complications to consider with MUA; these include humeral fractures, glenoid fractures, glenohumeral joint dislocation, rotator cuff tears (especially subscapularis), biceps tendon injuries and labral tears. Care needs to be taken when performing the procedure to avoid these complications while performing an effective manipulation to break down the inferior capsule. Manipulation techniques vary in clinical practice and in the literature, as described by Kraal et al. in their review [ 72 ].
Arthroscopic release
Arthroscopic release is often the preferred method of surgical treatment in refractory cases of adhesive capsulitis. It was first described in 1979 by Conti [ 73 ] and helps avoid the potential but significant complications of MUA. Arthroscopic release has been shown to have good short- and long-term outcomes in terms of both pain and function [ 74 , 75 ]. Arthroscopic release is also effective in patients with insulin-dependent diabetes mellitus, although the outcomes are better in nondiabetic patients [ 76 ] Similarly, patients with idiopathic and posttraumatic adhesive capsulitis have better outcomes than patients with postoperative adhesive capsulitis [ 77 ].
There are several other advantages to arthroscopic release, including controlled release of contracted capsule, synovectomy (if necessary), direct visualization of the joint and identification of other shoulder pathology. In addition, postoperative physical therapy can be started early because patients often have minimal pain. There are, however, some potential complications, including pain and recurrent stiffness, anterior dislocation of the shoulder and axillary nerve injury.
Although arthroscopic release has been shown to have good outcomes, there is still some controversy as to the surgical technique, particularly relating to the extent of the surgical release. Ogilvie-Harris et al. reported good pain relief and functional improvement after arthroscopic release of the intra-articular part of the subscapularis (IASS), superior glenohumeral ligament and the rotator interval [ 74 ]. Pearsall et al. reported that the IASS can be released during arthroscopic capsular release for frozen shoulder with minimal risk of secondary anterior instability [ 78 ]. However, the need to release the IASS is debatable and there is no definitive evidence to demonstrate that it confers significantly better outcomes. Snow et al. demonstrated no significant difference in improvement of ROM with both anterior and posterior capsular release compared with anterior release alone [ 79 ]. Conversely, Jerosch suggested that a 360-degree circumferential capsular release was a reliable method for restoring motion with minimum morbidity [ 80 ].
Kanbe et al. divided 267 ACS patients who underwent arthroscopic release into three groups, based on the severity of the adhesion between the coracohumeral ligament and the long head of biceps (LHB) tendon [ 81 ]. At 5 years post-surgery, all groups had significantly improved functional scores; however, patients with severe LHB and coracohumeral adhesion had significantly different outcomes from those with less severe adhesions (p < 0.0001) [ 81 ]. Notably, the authors also found diabetes mellitus to be a significant risk factor for severity of adhesion. This study highlights the importance of intraoperative release of LHB in arthroscopic release surgery for ACS.
Open release
Open release for adhesive capsulitis is an uncommon procedure because arthroscopic surgery carries significantly less postoperative morbidity. It may, however, be an option in patients who have had unsuccessful arthroscopic release; it has been shown to produce good outcomes in terms of both pain and ROM [ 82 , 83 ], although diabetic patients had poorer outcomes [ 82 ]. Omari et al. showed functional and symptomatic improvement after open arthroscopic release in 25 patients who had failed MUA [ 84 ]. Additional indications for open release include patients who have suffered strokes or head injuries and in posttraumatic or postsurgical adhesive capsulitis where there are significant adhesions and contractures preventing arthroscopic surgery [ 85 ].
ACS is a common condition that causes significant and prolonged morbidity for patients and carries wider economic implications. The management of adhesive capsulitis remains a challenge and there is a need for high-level, definitive evidence to suggest one form of treatment over another. As such, the treatment of this condition remains varied in clinical practice. There is moderate evidence for conservative approaches in the initial stages of ACS, including analgesics, oral steroids, intra-articular steroid or sodium hyaluronate injections, SNB and physiotherapy. Evidence in the literature for the efficacy of hydrodilatation therapy remains inconclusive. In cases resistant to conservative management strategies, MUA or arthroscopic capsular release are evidence-based treatment alternatives. There is limited evidence for open release, and it is also associated with greater post-operative morbidity compared with arthroscopic release. Surgical treatments should be complemented with an appropriate, supervised physical therapy regimen. Further understanding of the underlying pathology of ACS and large, randomized multicenter studies are required in order to define an evidence-based management strategy for the condition.
Future perspective
The last two decades have seen significant progress in our understanding of the pathophysiology behind ACS, which has complemented developments in current management strategies. However, there remains variation in clinical practice with no consensus in treatment for this condition. Nonoperative interventions remain first-line approaches in managing ACS and there is an urgent need for prospective RCTs comparing the efficacy of different treatment strategies. Furthermore, as our understanding of the immunological etiology of ACS develops, there may be opportunities for immunomodulating or targeted therapies in the future.
Executive summary
- Adhesive capsulitis of the shoulder (ACS) is a relatively common condition characterized by pain and stiffness of the shoulder joint.
- The pathophysiology of ACS is still not fully understood; however, histological studies have shown that the condition is characterized by a thickened, tight capsule, with chronic inflammatory cells and fibroblasts found in the joint capsule.
- Clinically, the presentation can be classified into four stages: painful, freezing, frozen and thawing.
- The goal of treatment is to restore patient function and manage symptoms, with a myriad of nonoperative and operative treatment strategies used in clinical practice.
- Physical therapy, often with adjuncts, is the preferred first-line treatment, although there remains a lack of high-level evidence in the literature to support this approach.
- Oral steroids have been shown to be effective in the short term, although their benefits after 6 weeks remain doubtful.
- Steroid injections have been shown in the literature to be as effective as, or even superior to, physiotherapy in the management of ACS.
- Sodium hyaluronate has been shown in one systematic review to be as effective as steroids and more effective than placebo; however, the evidence in the literature is controversial.
- There is a need for further research on the effectiveness of suprascapular nerve block and hydrodilatation, with some studies demonstrating promising results.
- Surgical treatment strategies of manipulation under anesthesia and arthroscopic release are effective in persistent cases of ACS, although there is variation in technique in both clinical practice and literature.
Author contributions
Both authors contributed equally to the writing of this paper.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Open access
This work is licensed under the Creative Commons Attribution 4.0 License. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
Papers of special note have been highlighted as: • of interest; •• of considerable interest
IMAGES
VIDEO
COMMENTS
Compound presentation means that a fetal hand is coming out with the fetal head. This is a problem because: The amount of baby that must come through the birth canal at one time is increased. There is increased risk of mechanical injury to the arm and shoulder, including fractures, nerve injuries and soft tissue injury.
A shoulder presentation is a malpresentation at childbirth where the baby is in a transverse lie (its vertebral column is perpendicular to that of the mother), thus the leading part (the part that first enters the birth canal) is an arm, a shoulder, or the trunk.While a baby can be delivered vaginally when either the head or the feet/buttocks are the leading part, it usually cannot be expected ...
Presentation refers to the part of the fetus's body that leads the way out through the birth canal (called the presenting part). Usually, the head leads the way, but sometimes the buttocks (breech presentation), shoulder, or face leads the way. Position refers to whether the fetus is facing backward (occiput anterior) or forward (occiput ...
7.6.1 Diagnosis. The uterus is very wide: the transverse axis is virtually equivalent to the longitudinal axis; fundal height is less than 30 cm near term. On examination: head in one side, breech in the other (Figures 7.1a and 7.1b). Vaginal examination reveals a nearly empty true pelvis or a shoulder with—sometimes—an arm prolapsing from ...
A transverse lie position in the third trimester may be rare, but here's what it means, the causes, and what can be done. ... it is also sometimes called shoulder presentation. But the fetus can ...
1. Contracted Pelvis. A very narrow pelvis in the mother can cause a shoulder presentation to occur. 2. Placenta Previa. A condition where the placenta covers the uterus opening, either completely or partially. This makes it difficult for your baby's head to enter the pelvic brim. 3. Intra-Uterine Fetal Death.
A shoulder presentation refers to a malpresentation at childbirth where the baby is in a transverse lie (its vertebral column is perpendicular to that of the mother), thus the leading part (the part that enters first the birth canal) is an arm, shoulder, or the trunk. While a baby can be delivered vaginally when either the head or the feet/buttocks are the leading part, it usually cannot be ...
Toward the end of pregnancy, the fetus moves into position for delivery. Normally, the presentation is vertex (head first), and the position is occiput anterior (facing toward the pregnant patient's spine) with the face and body angled to one side and the neck flexed. Abnormal presentations include face, brow, breech, and shoulder.
Shoulder Presentation (Transverse or Oblique lie) Definition. The longitudinal axis of the foetus does not coincide with that of the mother. These are the most hazardous malpresentations due to mechanical difficulties that occur during labour . The oblique lie which is deviation of the head or the breech to one iliac fossa, is less hazardous as ...
Remember that a shoulder presentation means the baby cannot be born through the vagina; if you detect it in a woman who is already in labour, refer her urgently to a higher health facility. In all cases of malpresentation or malposition, do not attempt to turn the baby with your hands! Only a specially trained doctor or midwife should attempt this.
Shoulder presentation. The incidence of shoulder presentation at term is 1 in 200 and is found with a transverse or oblique lie. Multiparity (uterine laxity) and prematurity are common associations and placenta praevia must be excluded. The lie will usually correct spontaneously before labour as uterine tone increases, although prolapse of the ...
Presentation of twins in Der Rosengarten ("The Rose Garden"), a standard medical text for midwives published in 1513. In obstetrics, the presentation of a fetus about to be born specifies which anatomical part of the fetus is leading, that is, is closest to the pelvic inlet of the birth canal. According to the leading part, this is identified as a cephalic, breech, or shoulder presentation.
The .gov means it's official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you're on a federal government site. ... A neglected shoulder presentation is an extremely rare obstetric complication in developed countries; however, it is a reality in low-income parts of the world. Our ...
Limb presentation during childbirth means that the part of the baby's body that emerges first is a limb - an arm or a leg. Babies with limb presentation cannot be delivered safely via vaginal delivery; they must be delivered quickly by emergency C-section (4). ... Shoulder presentation (transverse lie) is when the arm, shoulder or trunk of ...
Remember that a shoulder presentation means the baby cannot be born through the vagina; if you detect it in a woman who is already in labour, refer her urgently to a higher health facility. In all cases of malpresentation or malposition, do not attempt to turn the baby with your hands! Only a specially trained doctor or midwife should attempt this.
Shoulder presentation. Shoulder presentation means that the fetal shoulder is trying to come out first. This is a more advanced form of transverse lie and is undeliverable vaginally. In military settings, position and presentation can be made by: Pelvic Exam; Abdominal Exam (Leopold's Maneuvers) Single x-ray of the abdomen; Ultrasound if ...
Frozen shoulder Enlarge image. Frozen shoulder, also called adhesive capsulitis, involves stiffness and pain in the shoulder joint. Signs and symptoms typically begin slowly, then get worse. Over time, symptoms get better, usually within 1 to 3 years. Having to keep a shoulder still for a long period increases the risk of developing frozen ...
Frozen shoulder (FS) is a relatively common condition characterized by pain and stiffness of the shoulder joint. The exact cause of primary FS is unknown and in some patients the condition can persist for several years. Treatment strategies vary depending on stage of presentation, patient factors and clinician preferences.
Aetiology Clinical anatomy of the glenohumeral joint. The shoulder, or glenohumeral joint, connects the upper arm to the chest.It provides articulation between the glenoid fossa of the scapula and the head of the humerus.These articulating surfaces are separated by a narrow cavity filled with synovial fluid, making it a synovial joint. The shoulder joint is an example of a ball and socket ...
shoulder presentation: [ prez″en-ta´shun ] that part of the fetus lying over the pelvic inlet; the presenting body part of the fetus. See also position and lie . breech presentation presentation of the fetal buttocks, knees, or feet in labor; the feet may be alongside the buttocks (complete breech presentation); the legs may be extended ...
A neglected shoulder presentation is an extremely rare obstetric complication in developed countries; however, it is a reality in low-income parts of the world. Our tertiary care center is located in the rural and remote part of eastern Turkey. In this low-income region, many pregnant women deliver at home and go to the hospital only in case of ...
Joe Biden and Jill Biden both praised Biden's performance at the CNN Presidential Debate against former President Donald Trump. Some Democrats criticized Biden's performance and are ...