How to Analyze Interview Transcripts in Qualitative Research
Mar 15, 2024
Education , Transcription Blog
Rev › Blog › Transcription Blog › How to Analyze Interview Transcripts in Qualitative Research
Studies take time, accuracy, and a drive to provide excellent information, and qualitative research is a critical part of any successful study. You may be wondering how qualitative data adds to a paper or report, given that it’s not the hard “science” we often see highlighted the most often.
How Do You Analyze Qualitative Interviews?
There are two main approaches to qualitative analysis: inductive and deductive . What’s more, there are two types of inductive qualitative analysis to choose from. These are called thematic content analysis and narrative analysis, both of which call for an unstructured approach to research.
Inductive Methods of Analyzing Interview Transcripts
A thematic content analysis begins with weeding out biases and establishing your overarching impressions of the data. Rather than approaching your data with a predetermined framework, identify common themes as you search the materials organically. Your goal is to find common patterns across the data set.
A narrative analysis involves making sense of your interview respondents’ individual stories. Use this type of qualitative data analysis to highlight important aspects of their stories that will best resonate with your readers. And, highlight critical points you have found in other areas of your research.
Deductive Approach to Qualitative Analysis
Deductive analysis , on the other hand, requires a structured or predetermined approach. In this case, the researcher will build categories in advance of their analysis. Then, they’ll map connections in the data to those specific categories.
Each of these qualitative analysis methods lends its benefits to the research effort. Inductive analyses will produce more nuanced findings. Meanwhile, deductive analyses allow the researcher to point to key themes essential to their research.
Successful qualitative research hinges on the accuracy of your data. This can be harder to achieve than with quantitative research. It’s easy to lose important facts and meaning as you transition qualitative data from the source to your published content. This makes transcription a vital tool in maintaining integrity and relaying information in an unbiased way that’s useful for readers and adds appropriate context to the journal or study.
How to Transcribe a Qualitative Interview
Accurate transcription begins early in the interview process, even before you start interviewing. Here are the steps to transcribing a qualitative interview.
1. Collect Feedback for Qualitative Research
There are dozens of ways to gather qualitative data. Recording and accurately transcribing interviews is among the best methods to avoid inaccuracies and data loss, and researchers should consider this approach over simply taking notes firsthand.
Make sure you have a reliable way to record, whether the interview takes place in person, over the phone, or as part of a video call. Depending on the interview method, you may record a video or an audio-only format. Here are some tips depending on where the interview takes place:
These apps can also be used for over-the-phone interviews.
For video interviews , we recommend taking advantage of one of our transcription integrations , such as Zoom. Rev also has an API available for those who want to streamline their workflow even further by integrating Rev directly into their processes and platforms.
2. Organize Your Research Recordings
You should ensure that your audio or video files are easy to save, compile, and share. To do this, be sure to adopt easy-to-remember naming conventions as well to ensure they stay organized. An example of a naming convention that is simple to remember and recreate includes “Date.LastNameofSource.Topic”.
3. Transcribe All the Interviews and Focus Group Recordings
The next critical step is transcription. Done manually, this is a long and tedious process that can add hours, days, or even months to your report-writing process. There are dozens of pitfalls when performing transcriptions manually as well, as it can be hard to pick up words spoken in a heavy dialect or quiet tone. You also want to avoid having to transcribe all the “umms” and “ems” that occur when a source is speaking naturally.
Rev provides a variety of transcription services that take the tedium and guesswork out of the research process. You can choose to edit out all of the “umms,” while ensuring that heavy accents or muffled voices are picked up by the recording service.
You can order transcripts from Rev with both audio and video recordings. Once you’ve received your professional transcripts from Rev, you can begin your qualitative analysis.
The 6 Steps of Qualitative Interview Data Analysis
Among qualitative interview data analysis methods, thematic content analysis is perhaps the most common and effective method. It can also be one of the most trustworthy , increasing the traceability and verification of an analysis when done correctly. The following are the six main steps of a successful thematic analysis of your transcripts.
1. Read the Transcripts
By now, you will have accessed your transcript files as digital files in the cloud or have downloaded them to your computer for offline viewing. Start by browsing through your transcripts and making notes of your first impressions. You will be able to identify common themes. This will help you with your final summation of the data.
Next, read through each transcript carefully. Evidence of themes will become stronger, helping you to hone in on important insights.
You must identify bias during this step as well. Biases can appear in the data, among the interviewees, and even within your objectives and methodologies. According to SAGE Publishing , researchers should “acknowledge preconceived notions and actively work to neutralize them” at this early step.
2. Annotate the Transcripts
Annotation is the process of labeling relevant words, phrases, sentences, or sections with codes. These codes help identify important qualitative data types and patterns. Labels can be about actions, activities, concepts, differences, opinions, processes, or whatever you think is relevant. Annotations will help you organize your data for dissemination .
Be generous with your annotations—don’t hold back. You will have an opportunity to eliminate or consolidate them later. It’s best to do more here, so you don’t have to come back to find more opportunities later.
3. Conceptualize the Data
Conceptualizing qualitative data is the process of aligning data with critical themes you will use in your published content. You will have identified many of these themes during your initial review of the transcripts.
To conceptualize, create categories and subcategories by grouping the codes you created during annotation. You may eliminate or combine certain codes rather than using all the codes you created. Keep only the codes you deem relevant to your analysis.
4. Segment the Data
Segmentation is the process of positioning and connecting your categories . This allows you to establish the bulk of your data cohesively. Start by labeling your categories and then describe the connections between them.
You can use these descriptions to improve your final published content.
Create a spreadsheet to easily compile your data.
Then, use the columns to structure important variables of your data analysis using codes as tools for reference.
Create a separate tab for the front of the document that contains a coding table. This glossary contains important codes used in the segmentation process. This will help you and others quickly identify what the codes are referring to.
5. Analyze the Segments
You’re now ready to take a deep dive into your data segments . Start by determining if there is a hierarchy among your categories. Determine if one is more important than the other, or draw a figure to summarize the results. At this stage, you may also want to align qualitative data with any quantitative data you collected.
6. Write the Results
Your analysis of the content is complete—you’re ready to transition your findings into the real body of your content. Use your insights to build and verify theories, answer key questions in your field, and back aims and objectives. Describe your categories and how they are connected using a neutral, objective voice.
Although you will pull heavily from your own research, be sure to publish content in the context of your field. Interpret your results in light of relevant studies, theories, and concepts related to your study.
Why Use Interviews for Qualitative Data
Unlike quantitative data, which is certainly important, a qualitative analysis adds color to academic and business reports. It offers perspective and can make a report more readable, add context, and inspire thoughtful discussion beyond the report.
As we’ve observed, transcribing qualitative interviews is crucial to getting less measurable data from direct sources. They allow researchers to provide relatable stories and perspectives and even quote important contributors directly. Lots of qualitative data from interviews enables authors to avoid embellishment and maintain the integrity of their content as well.
So, how do you conduct interview data analysis on qualitative data to pull key insights and strengthen your reports? Transcribing interviews is one of the most useful tools available for this task.
As a researcher, you need to make the most of recorded interviews . Interview transcripts allow you to use the best qualitative analysis methods. Plus, you can focus only on tasks that add value to your research effort.
Transcription is Essential to Qualitative Research Analysis
Qualitative data is often elusive to researchers. Transcripts allow you to capture original, nuanced responses from your respondents. You get their response naturally using their own words—not a summarized version in your notes.
You can also go back to the original transcript at any time to see what was said as you gain new context. The editable digital transcript files are incredibly easy to work with, saving you time and giving you speaker tags, time marks, and other tools to ensure you can find what you need within a transcript quickly.
When creating a report, accuracy matters, but efficiency matters, as well. Rev offers a seamless way of doing the transcription for you, saving you time and allowing you to focus on high-quality work instead. Consider Rev as your transcription service provider for qualitative research analysis — try Rev’s AI or Human Transcription services today.
Everybody’s Favorite Speech-to-Text Blog
We combine AI and a huge community of freelancers to make speech-to-text greatness every day. Wanna hear more about it?
Transcribing interviews for qualitative research
Transcribing interviews is an important step in qualitative research, as it forms the backbone of data analysis and interpretation. In other words we can say that it acts as a vital link between those unfiltered conversations and insightful data acquired from them. But why is accurate transcription so crucial in qualitative studies?
The fundamentals of qualitative research itself provide the first justification. The depth with which linguistic expressions and emotions are communicated during interviews is crucial for this kind of research. Accurate transcription ensures that these non-verbal cues are also added for more clarity.
Transcribing interviews qualitative research is essential to ensuring the correctness of findings because it enables researchers to fully capture the range of participant replies and perspectives. Moving forward in this article we have compiled a comprehensive guide to help you get a more clear perspective on how to transcribe interviews for qualitative research.
What Is qualitative research?
Qualitative research is one of the most commonly used research methods in the field of academia. Instead of concentrating just on the what, where, and when of decision-making, it explores the why and how by focusing on the human aspects of a specific issue or situation. It aims to comprehend people's experiences, actions, feelings, and the interpretations they place on objects.
Getting a much deeper insight into people's attitudes, actions, value systems, concerns, motives and goals is the main aim of qualitative research. It is employed to acquire a deeper comprehension of intricate occurrences that are challenging to put into numerical form.
The main characteristics of qualitative research are:
Focus on context: It explores the context in which behaviours and events take place.
Subjectivity: It recognises the subjective nature of the study and frequently captures the perspectives of the participants.
Extensive analysis: This entails a thorough examination of a limited number of case studies or circumstances.
Inductive approach: The inductive approach often begins with observations and builds theories from them.
Flexibility in design: As the study goes on, the research question format may change. Here it is not necessary to follow the predetermined context.
Researchers use qualitative interview as their main method of data collection for this research since it allows them to interact with the subject first hand and focus on the non-verbal cues along with the information they are sharing.
Looking for support in transcribing your qualitative research interviews? Good Tape offers transcription services that can help you better understand your interviews. We're here to help make your transcription process more manageable and efficient. Explore how Good Tape can assist you in your research endeavors .
Qualitative vs quantitative interviews
Qualitative and quantitative interviews are different research approaches, each with a unique strategy for collecting and interpreting data. Quantitative interviews seek to measure human behaviour and experiences in a form that can be statistically examined, whereas qualitative interviews concentrate on investigating and comprehending the depth and complexity of human behaviour and experiences.
While both are extensively used in the field of research, it is important to understand where either of the two should be used. Below is a comparative table of both against which you can determine which of the two would work best in your scenario.
Aspect
Qualitative Interview
Quantitative Interview
Purpose
To understand people's experiences, ideas, and feelings on a deeper level.
To quantify information and generalise findings to a wider audience.
Nature of data collection
Textual, descriptive
Numerical, statistics
Data collection method
Open-ended questions and unstructured interviews
Close-ended questions and structured interviews
Sample size
Smaller since more focus is on depth of information
Larger since more focus is on statistics and generalisation
Approach
Exploratory
Conclusive and factual
Outcome
Detailed understanding of a particular problem or area of interest
Quantifiable insights
Flexibility
Increased flexibility as questions are adapted according to the situation
Decreased flexibility as questions are predetermined and close-ended
This table presents a clear contrast between qualitative and quantitative interviews, highlighting the differences in their technique, strategy, and study conclusions. The choice between both majorly depends on the research question at hand and the nature of the topic being studied.
How to transcribe an interview for qualitative research
For qualitative research, transcription of interviews is a painstaking procedure that needs time and close attention to detail. It requires turning spoken words from your recorded audio or video into text.
In qualitative research, this transcribing procedure is essential to data processing. Here's a step-by-step tutorial on effectively transcribing interviews, along with a few tips to make the process as easy as it can be.
Record clear audio of the interview
Select a peaceful, quiet workstation for your interviews to reduce distractions and improve focus. It is important to have a well-positioned microphone and high-quality headphones if you want to record even the minute details of speech without picking up excessive background noise.
If there are any unpleasant noises in your audio, services like Good Tape can be quite helpful. They are made to carefully pick up on all spoken and nonverbal cues, even in busy settings, and automatically transcribe all your work for you, so you won't miss any important information.
Work around your transcription
Precise transcription is essential for detailed analysis, accurately recording each word and nonverbal cue. This comprehensive approach allows for a deeper understanding of both the verbal as well as non-verbal cues in communication.
Similarly, intelligent verbatim concentrates on streamlining the text by eliminating unnecessary words and sounds to focus on the primary concepts, resulting in a transcript that is more focused and structured. Revised transcriptions enhance the material by improving clarity and fixing grammar, guaranteeing that the final transcript is accurate, comprehensible, and cohesive.
Audio transcription services such as Good Tape make accurate transcription easy with a shorter turnaround time.
Finalise the transcript
For easy navigation and the identification of important points or sensitive parts within the text, transcript formatting consistency is essential. Consistent formatting facilitates reading and improves the transcript's overall usefulness.
A further crucial stage is anonymisation, which anonymises any confidential or private data to comply with legal regulations. This also gives the interviewees peace of mind knowing that the information they provide will not be used illegally. To ensure that the transcript is correct, well-written, and presented professionally, one last review is necessary to spot any spelling, grammatical, or flow errors.
Some useful tips
Manual transcription can take a lot of time, therefore patience is essential. However, if you wish to have accurate transcripts in less time, using services such as Good Tape can cut down on the amount of time required.
It's also very important to make sure that your transcribed documents are safe. Maintaining regular backups is essential to avoiding data loss. Using services that automatically store and back up your transcribed audio might be a sensible choice if you find it difficult to remember to do backups, since they provide efficiency and peace of mind.
Why accurate transcription matters in qualitative research
Precise transcription is essential to qualitative research because it supports the accuracy and essence of the whole research process. It is the first stage of data analysis and has a direct impact on the findings and recommendations of the study. There are several reasons why accurate transcribing is important and advantageous.
Impact on data analysis
Maintains originality: Preserving the original context of spoken words is ensured via precise transcription. For accurate interpretation of the data, this is essential.
Enables comprehensive study: If the transcription has even minute error, it may prevent researchers from doing a thorough study of the interview data, including discourse, theme, and content analysis. Conversation analysis requires a lot of details which is possible through detailed notes of its accurate transcription.
Supports accuracy: Data analysis in qualitative research is a very crucial step. More valid findings are produced when transcripts are accurate because they give researchers a solid foundation.
Impact on research outcomes
Validity of findings: The reliability of the study findings is directly impacted by the quality of the transcribing. Inaccurate conclusions may result from word misinterpretation or omission.
Reliability and reproducibility: A key component of scientific investigation is replication, which is made possible by accurate transcribing, which also increases the research's dependability.
Reflects the voice of the participant: Accurate transcribing preserves the integrity of the participants' contributions by correctly capturing their voices.
Benefits of accurate transcription
Enhances credibility: Precisely recorded information strengthens the credibility of the study among other researchers and readers
Facilitates peer review and cooperation: Because other researchers can comprehend and analyse the data with clarity, it makes effective peer review and cooperation possible.
Enhances engagement with data: When data is precisely translated, researchers may interact with it at a deeper level, which results in more perceptive analysis and interpretation.
Accurate transcription plays a crucial role in maintaining the validity, reliability, and integrity of the research findings. It improves the quality and depth of data analysis, guaranteeing that the conclusions are solid, reliable, and accurate representations of the experiences and viewpoints of the participants.
Discover Good Tape’s interview transcription service
We’ve understood in depth how to transcribe interviews for qualitative research, let’s go over how you can do so accurately and quickly without having to put in much effort. Good Tape has a relatively simpler user interface which you can navigate through without any manual or instructions. Here’s what you can expect when going through the process of transcribing your audios.
Upload your file: The first step in the process is to upload the file you need to transcribe. Make sure the file is complete and has all the information you require
Select the language: Good Tape has a number of options when it comes to choosing the language of transcription. Select the one you want, although you can also choose the “auto-detect” option for the system to automatically identify the language in the audio.
Transcribe the text: Once the file is uploaded and the language is chosen, proceed further by clicking the “transcribe” button. Your audio transcription process starts here.
To wait or not to wait: If you’re a casual plan user, you will have to wait for some time for your transcription to be completed due to excessive load by the users. However, if you’re a professional or a team user, you get your results ASAP! The wait time depends on the plan you’re subscribed to .
Get notified: You will receive a notification once your transcribed document is ready. An e-mail will be sent to your inbox containing the link to access and download the document.
Looking for a good transcribing interviews qualitative research service? Try out Good Tape’s audio-to-text transcription service today and increase your work productivity. Their AI incorporated technology makes sure that every verbal and non-verbal cue is recorded, giving your qualitative data a deeper level of understanding.
More articles
Journalistic interview: How to interview someone for an article
From text to context: A complete guide to qualitative data analysis
What is verbatim transcription?
The essential transcription services for qualitative research
We believe everyone should have access to top-quality automatic trancriptions.
That's why Good Tape is completely free to use . No credit card required.
Why is it free?
The Ultimate Guide to Qualitative Research - Part 2: Handling Qualitative Data
Handling qualitative data
Introduction
Introduction to transcripts in qualitative research
Understanding the transcription process, practical insights: transcription in action, using transcription services, challenges in transcription.
Field notes
Survey data and responses
Visual and audio data
Data organization
Data coding
Coding frame
Auto and smart coding
Organizing codes
Qualitative data analysis
Content analysis
Thematic analysis
Thematic analysis vs. content analysis
Narrative research
Phenomenological research
Discourse analysis
Grounded theory
Deductive reasoning
Inductive reasoning
Inductive vs. deductive reasoning
Qualitative data interpretation
Qualitative data analysis software
Research transcripts
Conducting qualitative interviews or focus groups is only the first part of data collection in a qualitative research project. For most qualitative data analysis , you need to turn those audio or video files into written transcripts. While this may seem self-evident to many researchers, much discussion has taken place about transcripts, best research practices for generating them, the debate between transcription services and human transcription, and so much more.
Qualitative data transcription holds a key role in research , acting as the building blocks from which findings are derived and conclusions are drawn. They are the textual representation of verbal data gathered through interviews , focus groups , and observational studies . Given their significance, it's essential to grasp why they are fundamental to qualitative research.
What is the importance of transcripts in research?
The importance of transcripts in research lies in their ability to convert spoken language into written form, making data analysis significantly more manageable. Transcripts act as the raw material for your analysis , creating a tangible record of the conversations and discussions that form the basis of your research. They provide a precise, detailed account of the verbal data collected, enabling researchers to review the information repeatedly and uncover layers of meaning that might be overlooked when listening to the recording .
Transcripts help researchers systematically organize and manage the data, especially when dealing with large volumes of information. They make it easier to search for specific themes, patterns, or keywords, thereby speeding up the data analysis process. Furthermore, transcripts facilitate the sharing of data among researchers, allowing for collaborative analysis and review. They also ensure the transparency of your research by providing a permanent record that can be scrutinized by other researchers, reviewers, or auditors.
How is transcribing used in qualitative research?
A transcript is used as a way to record and represent the rich, detailed, and complex data collected during qualitative studies such as interviews, focus groups, or observations. Without transcriptions, it would be challenging for researchers to dissect, understand, and interpret the in-depth experiences, perceptions, and opinions shared by the participants. Most research involving audio recordings of interviews requires recordings to undergo the transcription process in order for qualitative data analysis to proceed.
Transcribing, in qualitative research, doesn't merely involve verbatim transcription (the word-for-word rendering of verbal data into text). It can also encompass the translation of non-verbal cues such as laughter, pauses, or emotional expressions that can provide valuable context and insights into the participants' experiences and perspectives. By capturing these details, transcripts can help portray a fuller, more authentic picture of the data, enabling a more comprehensive and nuanced analysis.
In qualitative research, transcriptions are also used for data coding , a process where researchers label or categorize parts of the data based on their content, themes, or patterns. This step is critical for identifying trends and making sense of the data, and having a written transcript makes the coding process significantly more efficient and precise.
How are transcripts used in quantitative research?
Interview transcripts also have an important role in quantitative research , specifically in methods like content analysis and conversation analysis . Content analysis involves the systematic coding and quantifying of data within transcripts, such as the frequency of specific words or themes. This allows researchers to discern patterns and trends and gain insights into the prevalence of certain concepts or attitudes. For example, this could involve quantifying the occurrence of health-related discussions within interviews with healthcare providers.
On the other hand, conversation analysis , while often qualitative, can include quantifiable aspects. Transcripts record details of conversation structure and patterns, such as timing and sequence of speech. Quantitative measures like the count of certain conversational elements or the duration of pauses can be used to understand communication dynamics.
In essence, transcripts are not solely a tool for qualitative research methods but also provide a source of quantitative data and a foundation for quantitative analysis methods. They allow for a detailed, tangible record of spoken data, crucial for both qualitative understanding and quantitative measures, showcasing their versatility in the research field.
The transcription process is a critical stage in qualitative research . It refers to the conversion of recorded or observed speech into written text, turning the fluid and dynamic nature of spoken communication into a tangible and analyzable form . In this section, we will delve deeper into the process of transcription and how it is approached in qualitative research.
How do you create a research transcript?
Writing a research transcript starts with the raw data , usually an audio or video recording from interviews , focus groups , or observations . The first step is to carefully listen to the recording and begin writing down what is being said. This should be done with utmost accuracy, capturing not only the spoken words but also any significant pauses, laughter, or emotional expressions.
A crucial aspect of writing a transcript is deciding how detailed it should be. This varies depending on the research objectives and the nature of the data. For some research, a verbatim transcription, which includes every utterance, filler words, and non-verbal cues, is necessary. For other studies, a clean verbatim transcript, which omits irrelevant details like repeated words or stutters, is sufficient. After the initial transcription, the transcript should be reviewed and cross-checked with the recording for accuracy. During this revision process, the researcher may also add time stamps, annotations, or comments to enrich the transcript further.
Other details in transcripts
Depending on your research inquiry, you may consider more nuanced approaches to generating transcripts when you require the analysis of complex and multifaceted data. Apart from accurately rendering the spoken words into text, a qualitative research transcript can also capture the context, meaning, and nuances inherent in the spoken interaction.
This could involve noting the tone of voice, pauses, emotional expressions, body language, and interactions among participants. These non-verbal cues can provide rich insights into the participants' attitudes, emotions, and social dynamics, thus giving the researcher a deeper understanding of the data.
One unique aspect of transcribing qualitative data is the reflection and interpretative process embedded in it. Researchers often gain a deeper understanding of the data during transcription, as it forces them to engage closely with the data and notice details that might have been missed during the initial data collection.
How is data transcription done?
Data transcription can be done manually or with the assistance of transcription software. Manual transcription involves the researcher or a transcriptionist listening to the recording and typing out the conversation. This method is time-consuming but can lead to a higher level of accuracy and deeper immersion in the data.
Automated transcription software, on the other hand, uses automatic speech recognition (ASR) technology to transcribe audio recordings into text. While this method is faster and can handle large volumes of data, it may not be as accurate, especially when dealing with poor audio quality, heavy accents, or technical jargon.
Regardless of the method chosen, the transcribed data should be reviewed and edited for accuracy. This might involve repeated listening to the audio, making corrections, and refining the transcript until it accurately represents the original data.
In summary, the transcription process is a meticulous task that requires careful listening, accurate writing, and thoughtful interpretation. It is an essential step in transforming the raw data into a form suitable for in-depth analysis, thus laying the foundation for your qualitative research findings. By understanding how to write a research transcript, specifically a qualitative research transcript, and knowing how data transcription is done, you'll be well-equipped to handle this critical phase of your qualitative research process.
Types of data transcription in qualitative research
As qualitative data can be diverse and complex, it’s important to understand that not all transcripts are the same. Depending on the research objectives, data characteristics, and the resources available, researchers might opt for different types of transcriptions. Let's delve deeper into these different types and their applicability in qualitative research.
What are the different types of data transcription?
There are generally three main types of data transcription:
1. Verbatim transcription: This is the most detailed form of transcription. It involves transcribing every single word, including filler words (like "um," "uh," and "you know"), false starts, repetitions, and even non-verbal cues such as laughter, pauses, or sighs. Verbatim transcription is often used in research where the manner of speaking or the emotional context is as important as the content itself.
2. Clean verbatim transcription: This type of transcription also captures every word spoken but omits filler words, stutters, and false starts, resulting in a cleaner, more readable transcript. Clean verbatim transcription is usually preferred when the focus is on the content of the speech rather than the style or manner of speaking.
3. Intelligent transcription (or edited transcription): This form of transcription goes a step further in simplifying and clarifying the text. It not only removes filler words and repetitions but also corrects grammatical errors and may even rephrase sentences for clarity. Intelligent transcription is typically used for creating transcripts intended for publication or for audiences who are not directly involved in the research.
What are the different types of transcription in qualitative research?
In qualitative research, the type of transcription used often depends on the nature of the study and the level of detail required in the analysis.
For studies aiming to explore the content of the conversations, clean verbatim or intelligent transcriptions might be sufficient. These types provide a clear and concise account of the spoken data, allowing researchers to easily identify themes and patterns in the content.
However, for studies interested in the nuances of communication, such as sociolinguistic studies or discourse analysis, a verbatim transcription might be more appropriate. This type captures the exact words, speech patterns, and non-verbal cues, thus providing a richer and more authentic representation of the spoken interaction.
Choosing the right type of transcription for your qualitative research is crucial, as it can significantly impact the depth and quality of your data analysis . By understanding the different types of data transcription and their uses in qualitative research, you will be better positioned to make an informed decision that aligns with your research goals.
ATLAS.ti makes conducting qualitative research easy
Turn your research data into key insights starting with a free trial of ATLAS.ti.
Transcription is more than a technical process; it's a fundamental part of the journey from data collection to analysis in qualitative research . Understanding transcription in action means knowing how to do it, what to include, and how to record it for optimal use in your study.
What are examples of transcription?
Transcription can take various forms based on the nature of your research. For instance, a sociolinguistic study might require a detailed verbatim transcript, including non-verbal cues and speech anomalies.
Here's an example:
Interviewer: So, how are you feeling about the project? (in a concerned tone) Participant: Umm... Well, (laughs nervously) it's been a bit... um, overwhelming?
On the other hand, an interview transcript for a market research study might be a clean verbatim transcript, focusing on the content. Here's how it could look:
Interviewer: What do you like about our product? Participant: I really enjoy its user-friendly interface and the customer service is exceptional
How do you transcribe a research interview?
Transcribing a research interview involves several steps. First, ensure you have a good-quality audio or video recording of the interview . Listen to the recording carefully, typing out the conversation verbatim. You can also slow down the speed of the recording, and shortcut keys to rewind the recording a few seconds can be a great help. It's essential to maintain accuracy and include key details that might influence the interpretation of the data , such as significant pauses or emotional inflections.
Depending on your research aims, you may choose to transcribe in verbatim, clean verbatim, or intelligent transcription style. Once the initial transcription is complete, review and cross-check it against the recording for accuracy. Finally, anonymize the data if necessary to ensure participant confidentiality .
What should be included in an interview transcript?
An interview transcript should include everything that is said in the interview, but the level of detail can vary. Here are some elements that are typically included:
1. Identifiers: These help distinguish between different speakers. In the case of an interview, this would usually be the interviewer and the interviewee(s). 2. Verbal responses: All responses to the interview questions should be included in the transcript. 3. Non-verbal cues: Depending on the research objectives, non-verbal cues such as laughter, sighs, or pauses can provide additional context and should be included. 4. Time stamps: These help locate specific parts of the audio recording and can be very helpful during analysis. 5. Annotations: These might include comments or notes made by the transcriber about the context, the tone of voice, or background noises.
How do I record an interview transcript?
Recording an interview transcript starts with creating an audio or video recording of the interview. After the interview, use either manual transcription or automatic transcription software to convert the audio into written text. Make sure to include identifiers for each speaker, their verbal responses, and any relevant non-verbal cues. Review and revise the transcript for accuracy, adding time stamps or annotations as needed.
In summary, transcribing interviews is a meticulous task that requires careful attention to detail and accuracy. By understanding what to include in a transcript and how to record it, you'll be well-equipped to capture the richness and depth of your interview data, laying the groundwork for a robust analysis.
Benefits of transcription in qualitative research
In qualitative research , transcription represents more than a technical or administrative task. It’s the transformative process that turns spoken communication into a tangible, accessible text form that can be critically examined, dissected, and evaluated. This process forms the underpinning of the entire data analysis journey, creating the foundation upon which interpretations are built and conclusions are drawn.
Looking deeper into the benefits of transcription in qualitative research
Unearthing the multiple layers of transcription’s benefits in qualitative research reveals how it contributes to the efficacy and integrity of a study.
1. Facilitating data accessibility: One of the fundamental benefits of transcription is that it brings to life the spoken word, facilitating accessibility. It translates data into a format that is readable, searchable, and conducive to rigorous analysis. Transcripts can be reviewed multiple times, allowing researchers to revisit the data continually. They can be easily shared among team members or other researchers, enhancing the communicability of the study. Transcription also bridges barriers for those who are hearing-impaired or for whom the original language of the conversation might be a hurdle.
2. Enabling comprehensive analysis: Transcripts are the bedrock upon which qualitative analysis is built. They provide the raw material for various methods of qualitative data examination, whether it's the deep dive of a thematic analysis , the linguistic focus of discourse analysis , or the systematic categorization of content analysis . These written records allow researchers to delve into the data, identify recurring patterns, extract significant themes, and uncover insights that might be less discernible or entirely lost in the original audio or video format.
3. Promoting reflection and interpretation: Transcription is far from being a mechanical, dispassionate process. It necessitates active and continual engagement with the data , leading to a process of reflection and interpretation that forms the basis of qualitative analysis. During the act of transcribing, researchers can glean new insights, recognize overlooked details, and begin to make initial interpretations. It's often during this process that the data begin to speak, allowing researchers to discern their meaning and value.
4. Providing evidence and establishing an audit trail: Transcripts constitute a concrete, verifiable record of the data collected, the words expressed by the participants, their sentiments, and their experiences. This record acts as a form of evidence to substantiate the research findings, ensuring their credibility. Furthermore, they provide an audit trail, contributing to the transparency, accountability, and, thus, the overall trustworthiness of the study.
Justifying the use of transcription for qualitative data
The crucial role of transcription in qualitative research is underscored by its ability to capture the richness and multifaceted nature of spoken data and convert it into a format ripe for in-depth analysis. It provides a lens through which subtle nuances of communication - the ebb and flow of conversation, shifts in tone, or emotional expressions - can be understood. This is invaluable in qualitative research, where the aim is to capture and understand the depth and complexity of human experiences.
Transcripts also serve as a durable, enduring record of the data, preserving the words and voices of the participants. They ensure that the insights, stories, and experiences shared by participants are not transient but can be revisited, reviewed, and reinterpreted in future research.
Transcription services have revolutionized the way researchers process their data, offering a range of possibilities from manual transcription to advanced AI-driven software. These services often come with their own benefits and drawbacks, and understanding these is key to making an informed decision for your qualitative research project. This section will delve into the world of transcription services, helping you to explore your options and make the best choice for your research needs.
Types of transcription services
Broadly, transcription services fall into two main categories: human services and automated services.
Human transcription services employ professional transcribers to convert your audio or video files into text. These services often offer high-quality, accurate transcripts, as they benefit from the nuanced understanding and context interpretation abilities of a human transcriber.
Automated transcription services, on the other hand, use speech recognition software to transcribe audio or video files. They are typically faster and less expensive than human transcription services, but their accuracy can vary depending on the quality of the audio and the complexity of the language used.
Advantages and disadvantages of outside services
Choosing between human and automated transcription services often depends on your project's specific needs. Let's delve into some advantages and disadvantages of each.
Advantages of human services
1. Accuracy: Human transcribers can understand context, decipher accents, and make out words in poor-quality audio better than any software, ensuring high-quality transcripts.
2. Personalized service: They offer personalized service with attention to detail, including specific formatting requests or specialized transcription styles.
Disadvantages of human services
1. Time-consuming: Human transcription is slower than automated transcription, which can be an issue for projects with tight timelines.
2. Cost: Human transcription services can be expensive, especially for large volumes of data. Advantages of automated services
1. Speed: Automated services can transcribe audio or video files much faster than human transcribers.
2. Cost: They are usually more affordable than human transcription services, making them a good option for budget-conscious projects.
Disadvantages of automated services
1. Accuracy: While speech recognition technology has improved significantly, it still struggles with accents, poor audio quality, and complex terminology, which may lead to less accurate transcripts.
2. Lack of context: Automated services may not capture nuances in language or understand context the way a human transcriber can.
Tips for choosing the right service
Selecting the right transcription service should be based on the specific needs and constraints of your project. Here are a few tips to guide your choice:
1. Assess your needs: Consider the complexity of your data, the quality of your recordings, your budget, and your timeline.
2. Test the service: If possible, use a short sample of your data to test the service. This can give you a sense of the quality of the transcription and whether it meets your needs.
3. Read reviews: Check out reviews and ratings from other users to gauge the reliability and performance of the service.
These outside services can be a valuable resource in qualitative research, saving you time and effort. By understanding the benefits and drawbacks of human and automated services and evaluating your specific research needs, you can make an informed choice that best supports your research goals.
The transcription process, while invaluable to qualitative research , does not come without its fair share of challenges. The transformation of oral data into written format can be a complicated endeavor, particularly in cases where the audio quality is poor, speakers have heavy accents, or the conversation is filled with technical or specific jargon. Despite these hurdles, there are various strategies that can help you navigate these issues and ensure high-quality, accurate transcripts.
Audio quality
One of the most common challenges in transcription is dealing with poor audio quality. Background noise, low speaking volumes, or unclear pronunciations can make it difficult to distinguish what is being said. It's a good idea to invest in high-quality recording equipment and choose a quiet, controlled environment for your interviews or focus groups. Ensure that all participants speak clearly and loudly enough to be heard. If your data is already collected and the audio quality is poor, consider using noise-canceling software or hiring a professional transcription service that specializes in handling poor-quality audio.
Accents and dialects
Dealing with heavy accents or unfamiliar dialects can be challenging, particularly for automated transcription services that may not be programmed to handle a wide range of accents or dialects. Human transcribers can spend time familiarizing themselves with the accent or dialect to aid their comprehension. In some cases, it may be beneficial to engage a local transcriber who is familiar with the accent or dialect. For automated services, choosing a service that offers multilingual support or can handle a variety of accents can improve the accuracy of your transcripts.
Technical jargon and specific language
Transcribing conversations that include technical jargon, specific terminology, or industry-specific language can be a challenge, especially if the transcriber is not familiar with the terminology. If you are outsourcing your transcription to a human service, providing a glossary of terms to your transcriber can be very helpful. This can include definitions of technical terms, acronyms, or any specific language used in your study. If using an automated service, choose one that has capabilities to learn and adapt to specific terminology.
Time and resources
Transcription can be a time-consuming and resource-intensive process, especially for large volumes of data. Consider using transcription software or outsourcing to a transcription service to save time. If you’re transcribing manually, developing a systematic approach can increase efficiency. This can include using transcription software to speed up or slow down the audio, utilizing keyboard shortcuts, or creating a consistent formatting system.
Choose ATLAS.ti for your interview research
Analyze transcripts for interviews and focus groups with ATLAS.ti. Download a free trial today.
Research article
Open access
Published: 06 July 2009
Interviewee Transcript Review: assessing the impact on qualitative research
Victoria Hagens 1 ,
Mark J Dobrow 1 , 2 &
Roger Chafe 1 , 2
BMC Medical Research Methodology volume 9 , Article number: 47 ( 2009 ) Cite this article
24k Accesses
103 Citations
Metrics details
This paper assesses interviewee transcript review (ITR) as a technique for improving the rigour of interview-based, qualitative research. ITR is a process whereby interviewees are provided with verbatim transcripts of their interviews for the purposes of verifying accuracy, correcting errors or inaccuracies and providing clarifications. ITR, in various forms, is widely used among qualitative researchers, however there is limited methodological guidance on how it should be employed and little is known about its actual impact on the transcript, the data, the interviewee or the researcher.
ITR was incorporated into a qualitative research study in which 51 key informant interviews were conducted with a range of senior stakeholders within the Canadian health care system. The changes made by interviewees to their transcripts were systematically tracked and categorized using a set of mutually exclusive categories.
The study found that ITR added little to the accuracy of the transcript and may create complications if the goal of the researcher is to produce a transcript which reflects precisely what was said at the time of the interview. The advantages of ITR are that it allows interviewees the opportunity to edit or clarify information provided in the original interview, with many interviewees providing corrections, clarifications, and in some cases, adding new material to their transcripts. There are also potential disadvantages, such as a bias created by inconsistent data sources or the loss of data when an interviewee chooses to remove valuable material. The impact of ITR on the interviewee may be both positive and negative, depending on the specific circumstances and the nature of the study. The impact of ITR on the researcher was minimal in this study, but is again subject to specific circumstances of the research context.
While ITR is employed by many researchers across numerous fields, the advantages of its use may be relatively small in terms of verifying the accuracy of qualitative interview transcripts. Researchers are advised to carefully consider both the potential advantages and disadvantages of ITR outlined in this paper before deciding to incorporate the practice within their qualitative study designs.
Peer Review reports
As part of the qualitative research process, researchers in a variety of fields, such as health [ 1 – 3 ], education[ 4 , 5 ], management[ 6 , 7 ] and social theory[ 8 , 9 ], often invite interviewees to review transcripts of their interviews. We refer to this practice, in its various forms, as interviewee transcript review (ITR). ITR can include requests for interviewees to identify and correct transcription errors or omissions, and in some cases, to clarify or provide additional information and insights directly linked to interview responses. In contrast to approaches for validating research findings, such as member checking [ 10 – 12 ] or triangulation [ 12 , 13 ], we focus on ITR as a methodological approach for verifying the accuracy of the interview transcript before it is formally coded and analyzed.
While there is a large body of literature examining ways to improve methodological rigour in the collection and analysis of qualitative data[ 11 , 14 – 17 ], there is surprisingly limited guidance regarding the verification and review of interview transcripts before they are subjected to formal coding and analysis. ITR raises a number of interesting methodological issues. Perhaps most importantly, although ITR is regularly used, it is unclear what its actual impact is on qualitative research. The purpose of this paper is to provide researchers with guidance about whether ITR should be incorporated into their study design. We conducted a detailed audit of the impact of ITR that was incorporated into the methodology for a recent interview-based, qualitative research study. Our examination focuses on four key questions regarding the impact of ITR on (1) the quality of the interview transcript (e.g., does ITR result in a transcript that more accurately reflects the verbal interview exchange); (2) the quality of the interview data derived from the interviewee (e.g., does ITR result in additional insights or clarification on what the interviewee knows or believes beyond what was exchanged during the interview); (3) the interviewee; and (4) the researcher?
As part of an embedded multiple case study that examined the development of population-based colorectal cancer screening policies in five Canadian provinces, we incorporated ITR into the study design to assess its impact on the four questions outlined above. The study included 51 semi-structured interviews conducted with government representatives, health system leaders, clinical and epidemiological experts, and advocacy group representatives. Each interviewee signed an informed consent form before participating in the interview. A standard interview guide was used for the interviews, which were all conducted by one of the authors (VH). The interviews lasted on average 50 minutes. Each interview was digitally recorded and a verbatim transcript was prepared by a professional transcriptionist.
Interviewees were informed at the conclusion of the interview that the interview transcript would be sent to them so that it could be reviewed and that they could make corrections if necessary or desired. Each interview transcript was compared to the digital interview recording by one of the authors (VH), before being emailed to the interviewee with an invitation to "review it and send any corrections." Interviewees were asked to return any comments or feedback on their transcripts within two weeks. All edits, additions and omissions made to the interview transcript were documented. Table 1 outlines the ITR process employed.
Six mutually exclusive categories were developed which encompass all types of interviewee edits/additions/omissions made to the interview transcript (Table 2 provides examples). The categories are:
Category 1. Specific transcription errors/omissions corrected
These include instances where the interviewee corrected a word, phrase or name of a person, organization or other entity, data or statistic, which had either been transcribed incorrectly or left incomplete because neither the transcriptionist nor the researcher in conducting initial transcript verification were able to accurately interpret what was said.
Category 2. Specific details added to transcript
These include instances where the interviewee added a specific detail to the transcript, such as the name of a person, organization or other entity, date or statistic, that the interviewee had not been able to recall at the time of the interview.
Category 3. Specific transcription details corrected/changed
These include instances where a specific detail that had been provided in the interview, such as the name of a person, organization or other entity, date or statistic, was corrected or changed by the interviewee upon review of the interview transcript.
Category 4. Grammatical changes or minor clarifications made to transcript
These include instances where the interviewee rephrased a statement made in the interview. The meaning of the statement was not changed, but edits were made to grammar or sentence structure, or the meaning was conveyed using different vocabulary.
Category 5. Statements removed from transcript
These include instances where an interviewee removed a specific section of the transcript.
Category 6. Statements added to transcript
These include instances were an interviewee added comments or statements to the transcript to offer new perspectives and insights which were not made in the interview.
One author (VH) reviewed all revised interview transcripts and classified all edits/additions/omissions into one of the six categories.
Of the 51 interviewees invited to review their interview transcripts, 22 (43%) responded either by returning a revised transcript (16) or by indicating that they had reviewed the transcript but had no revisions to make (6). Of the 16 interviewees who submitted revisions to their transcripts, 12 did so by sending a revised transcript to the researcher by email with changes tracked using the word processor's "track changes" feature. Two interviewees submitted printed copies of the transcript with hand-written revisions, while another two interviewees submitted electronic copies of the transcript with changes made but not tracked. Table 3 summarizes the results of the ITR audit for the 22 interviewees who indicated that they had reviewed their interview transcripts.
For the 16 revised transcripts, 39 specific transcription errors were corrected (category 1), 11 specific details were added (category 2), and 6 specific transcription details were corrected (category 3). There were 204 instances in which an interviewee made grammatical changes and/or revised the transcript in an apparent effort to clarify or articulate better a point made in the interview (category 4). There were another 39 instances where interviewees removed statements from their transcripts (category 5). These were generally statements of opinion, although a few factual statements were also removed. There were also 43 instances where interviewees added new information that had not been discussed during the interview (category 6). Two of the interviewees added numerous new and substantive comments that had not been discussed during the interview.
The audit provided useful data for assessing the potential advantages and disadvantages of ITR. Table 4 summarizes the impacts of ITR on the transcript, the data provided, the interviewee and the researcher.
Impact of ITR on the interview transcript
While there is some disagreement among researchers about what constitutes good quality transcription [ 16 , 18 ], for the purposes of this audit we characterize a high quality interview transcript as a complete and accurate reflection of the verbal exchange between the interviewer and interviewee during the interview. Based on this characterization, transcription quality was improved by ITR (beyond normal transcript verification by the researcher) with 39 errors and omissions corrected (category 1). Typically, however, these were relatively minor corrections and while all interviewees were offered the opportunity to revise their transcripts, only 16 (31%) interviewees returned a revised transcript, with some of these interviewees stating that they did not read their transcripts carefully because they found them to be too lengthy and/or cumbersome to review. As well, the majority of interviewees who revised their transcripts did so in such a way that the transcript no longer reflected accurately the verbal exchange during the interview. Transcripts revised by interviewees therefore can be seen to represent a different type of data source than the transcripts not revised by other interviewees.
The incremental benefits of ITR in producing marginally higher quality transcripts likely do not justify its use. If the goal is solely to correct inaccuracies in interview transcripts then a modified process involving researcher verification of the interview transcript, as was also done in this study, followed by targeted interactions with interviewees to clarify any outstanding errors, inaccuracies or omissions, is likely a more appropriate approach than ITR. In our study, having one of the researchers check the transcript provided by the transcriptionist against the audio recording corrected the vast majority of transcription errors and omissions. A researcher could then contact specific interviewees with specific questions about their transcripts (such as the correct spelling of a name, or a key word that is missing from a sentence), rather than sending full transcripts to all interviewees for their review. Combined, researcher review and targeted follow-up can improve transcription quality without requiring interviewees to review their full transcripts.
Impact of ITR on the interview data
The impact of ITR on the quality of interview data is a more complicated issue. An accurate interview transcript can still represent poor quality data if the interviewee has inaccurately conveyed his or her knowledge or beliefs. Existing guidelines and methods protocols which address quality and rigour in qualitative research provide only limited and indirect guidance on how ITR techniques impact on data quality[ 10 , 19 – 22 ]. Based on the results of this audit, ITR can improve the quality of interview data where specific details are added or corrected by interviewees such as dates, statistics, and the names of people, organizations or other entities (categories 1, 2, and 3). Almost two-thirds of the interviewees who reviewed their transcripts within our audit added or corrected at least one such detail. While specific missing details may be more reliably added through direct, targeted communication with interviewees, incorrect details are most likely only detectable by the interviewees themselves and so ITR may be the only way to achieve this improvement to data quality.
It is less clear whether interviewees should be given the opportunity to edit the wording of statements made in their interviews (category 4) or to include additional information (category 6). Such results can improve data quality by providing researchers with increased clarity around key statements in the interview and/or providing additional insights which would not otherwise have been acquired. Indeed, in this study, the ITR process resulted in substantive new insights from two interviewees which could potentially influence the data analysis. However, there are important questions which need to be considered regarding whether ITR is the appropriate approach to obtaining these additional insights. First, it may be argued that spontaneous responses delivered in an interview setting are likely to offer different insights than responses modified through ITR. Even where the intention of an interviewee is simply to clarify a statement by editing grammar or sentence structure, information which was gleaned from a more candid expression during an interview might be lost[ 23 ]. Second, incorporating interviewees' key additional comments and revisions may generate a systematic bias, with some interview transcripts reflecting interviewees' more thoughtful and time-considered responses to interview questions, compared with other transcripts simply reflecting the unaltered verbal interview exchange. And third, it should be noted that employing ITR in our study resulted in only two of the 51 interviewees (two of 22 interviewees who responded to the ITR request) providing significant new insights, creating questions regarding the efficiency of this approach for collecting additional data.
ITR also impacts on interview data quality when data are retracted by interviewees[ 24 ]. In this study, seven interviewees removed at least one statement from their transcripts, with two of those interviewees removing statements which provided particularly important and/or controversial comments. This study involved discussions regarding sometimes sensitive issues surrounding the development of a major public policy decision and some candid interview comments were particularly informative. However, based on the ethics protocol for the project, statements removed by interviewees were not included in the analysis. While data loss can be viewed as a potential disadvantage of ITR, the ethical responsibility to protect the interviewee can be enhanced through the process.
Impact of ITR on the interviewee
For interviewees, an advantage of ITR is that their rights as research participants are reinforced. The right to withdraw one's own responses from a research study is a right which is ensured to research participants in many ethics protocols and was stated in the consent forms signed by interviewees in this study. However this right is often difficult to exercise if the participant is not provided with a transcript or summary of the interview exchange. As shown above, seven of our interviewees chose to withdraw material from their transcripts, thus exercising a right that they may not otherwise have had the opportunity to employ.
This advantage for the interviewee needs to be balanced against some potential disadvantages. Serious harm could be caused if a transcript is mistakenly sent to the wrong interviewee. While necessary care was taken to ensure that this did not occur in this study, it is important to note that a breach of privacy of this sort could result in harm to participants greater than any benefits gained from ITR, as well as a violation of the protections researchers make to their study participants. Additionally, some interviewees may feel discomfort reviewing verbatim transcripts. In particular, when the interview focuses on personal experiences and/or sensitive topics, requests for the interviewee to review the transcript may add considerably to the burden of participation. Interviewees may even experience discomfort with respect to reviewing poor grammar reflected in their transcripts, as was expressed by several interviewees in our study.
Finally, it is important to note that considerable time and effort is required from interviewees to participate in ITR. Transcripts can be both lengthy and cumbersome to read, and although participation in transcript review is voluntary, interviewees who wish to participate or who perceive pressure to participate may be negatively impacted by the time and effort required.
Impact of ITR on the researcher
The impacts of ITR on the researcher should also be considered in the context of weighing the overall advantages and disadvantages of the technique. One impact of ITR on the researcher is that the relationship between interviewees and researchers is reinforced. Lines of communication are kept open, and in some cases an additional method of correspondence is established (e.g., email), thus facilitating future exchanges. In this study, several interviewees indicated during their interview that they had relevant documents that might be of interest to the researchers, with the ITR process providing a convenient follow-up mechanism. Additionally, ITR can save the researcher time required to fill-in blanks and/or check questionable details within transcripts.
One potentially negative impact of ITR on the researcher is the additional time and effort required for transcript preparation and communication with interviewees. Appropriate steps must be taken to securely deliver the transcript to the appropriate interviewee and analysis of interview data can be delayed due to the time required to allow interviewees to review their transcripts. For this study, the two-week time window for interviewees to respond with transcript revisions did not alter our analysis timelines significantly, however other research processes may be subject to different time pressures thus altering the impact of this delay.
Study limitations
The impacts of ITR likely vary by the target population and the nature of the research questions addressed. In this study, we conducted interviews with key stakeholders in the Canadian health care system, including senior clinical and administrative leaders. Issues related to power differentials between the researcher and the interviewee, literacy levels, or email access were not a factor for our interviewee population. Therefore, while the process of ITR was well within the basic capabilities of our study population, it might not necessarily be so for other more varied populations, particularly patient populations. The nature of our project directed focus on interviewees' perceptions of key events and factors within a complex policy-making process. Other issues may arise when interviews are primarily intended to capture interviewees' experiential knowledge, where contradictions and factual misinformation may provide the researcher with significant insights.
It should be noted that in our assessment of the impacts of ITR we did not attempt to assess the various methods of conducting ITR. Recognizing that there are numerous variables in this process – such as when and how the interviewees are invited to participate in ITR; whether transcripts are provided to all interviewees in a study or only those interviewees who respond positively to an ITR invitation; and the specific instructions given to interviewees on the purpose of ITR and on the types of feedback they are requested or invited to provide – further research is required to assess the role played by these variables in the impacts of ITR on the transcript, the data, the interviewee and the researcher.
The decision to use ITR must weigh its potential advantages and disadvantages as they relate to the particular study at hand. While ITR is employed by many researchers across numerous disciplines, overall our audit revealed that the advantages to its use may be relatively small, particularly in relation to the added time and effort required for interviewees and in light of other existing techniques to address transcript and data quality such as researcher review of transcripts and targeted communication with interviewees. Furthermore, ITR as defined in this study, is not intended for the validation of qualitative research findings. However, further examination of how ITR could be potentially integrated with established methods for validating qualitative research findings, such as member checking, is needed. Researchers who are considering the use of ITR are advised to be clear on what they hope to achieve through its use and to take into account the various impacts associated with ITR for their specific project and interviewee population.
Goeman D, Aroni R, Stewart K, Sawyer S, Thien F, Abramson M, et al: Patients' views of the burden of asthma: a qualitative study. Medical Journal of Australia. 2008, 177: 299-
Google Scholar
Beeton K, Neal D, Lee C: An exploration of health-related quality of life in adults with haemophilia – a qualitative perspective. Haemophilia. 2005, 11: 123-132. 10.1111/j.1365-2516.2005.01077.x.
Hall C: Re-forming the teaching work force: the case of the academic coach. Educational Review. 2007, 59: 161-178. 10.1080/00131910701254932.
Article Google Scholar
Strauss P: Group assessments: dilemmas facing lecturers in multicultural tertiary classrooms. Higher Education Research & Development. 2007, 26: 147-161. 10.1080/07294360701310789.
Ardley B: Situated learning and marketing. Marketing Education: Constructing the Future. 2006, 24: 202-217.
Schroeder A, Pauleen D: KM governance: investigating the case of a knowledge intensive research organisation. Journal of Enterprise Information Management. 2007, 20: 414-10.1108/17410390710772696.
Reimer KS, Furrow JL: A Qualitative Exploration of Relational Consciousness in Christian Children. International Journal of Children's Spirituality. 2001, 6: 7-23. 10.1080/13644360120100504.
Sinacore AL, Healy P, Justin M: A Qualitative Analysis of the Experiences of Feminist Psychology Educators: The Classroom. Feminism & Psychology. 2002, 12: 339-10.1177/0959353502012003007.
Creswell J: Qualitative Inquiry and Research Design: Choosing among five traditions. 1998, London: SAGE Publications
Lincoln Y, Guba E: Naturalistic Inquiry. 1985, Beverley Hills: Sage Publications
Bloor M: Techniques of validation in qualitative research: a critical commentary. Context and Method in Qualitative Research. Edited by: Miller G, Dingwall R. 1997, London: Sage Publications, 37-50.
Denzin N: Sociological Methods: A Sourcebook. 1978, New York: McGraw Hill, 2
Mays N, Pope C: Qualitative research in health care: Assessing quality in qualitative research. BMJ. 2000, 320: 50-52. 10.1136/bmj.320.7226.50.
Article CAS PubMed PubMed Central Google Scholar
Mays N, Pope C: Qualitative Research: Rigour and qualitative research. BMJ. 1995, 1995: 109-112.
Seale C, Silverman D: Ensuring Rigour in Qualitative Research. European Journal of Public Health. 1997, 1997: 379-384. 10.1093/eurpub/7.4.379.
Barbour RS: Checklists for improving rigour in qualitative research: a case of the tail wagging the dog?. BMJ. 2001, 322: 1115-1117. 10.1136/bmj.322.7294.1115.
Lapadat J, Lindsay A: Transcription in Research and Practice: From standardization of technique to interpretive positionings. Qualitative Inquiry. 1999, 5: 64-86. 10.1177/107780049900500104.
Clark J: How to peer review a qualitative manuscript. Peer review in health sciences. Edited by: Godlee F, Jefferson T. 2003, London: BMJ Books, 219-235.
Malterud K: Qualitative Research: standards, challenges, and guidelines. The Lancet. 2001, 358: 483-488. 10.1016/S0140-6736(01)05627-6.
Article CAS Google Scholar
McLellan E, MacQueen K, Neidig J: Beyond the Qualitative Interview: Data preparation and transcription. Field Methods. 2003, 15: 63-84. 10.1177/1525822X02239573.
Lincoln Y, Guba E: Paradigmatic Controversies, Contradictions, and Emerging Confluences. Handbook of Qualitative Research. Edited by: Denzin N. 2000, Thousand Oaks, Calif.: Sage Publications, 163-
Laurier E: Talking About Cigarettes: Conversational narratives of health and illness. Health. 1999, 3: 189-207. 10.1177/136345939900300204.
Sandelowski M: Rigor or Rigor Mortis: The problem of rigor in qualitative research revisited. Advances in Nursing Science. 1993, 16: 1-8.
Pre-publication history
The pre-publication history for this paper can be accessed here: http://www.biomedcentral.com/1471-2288/9/47/prepub
Download references
Acknowledgements
The authors are grateful to the interviewees for their participation in the study. The study was supported by funding from a grant from the Canadian Institutes of Health Research: CIHR Team in Population-Based Colorectal Cancer Screening.
Author information
Authors and affiliations.
Cancer Services and Policy Research Unit, Cancer Care Ontario, Canada
Victoria Hagens, Mark J Dobrow & Roger Chafe
Department of Health Policy, Management and Evaluation, University of Toronto, Canada
Mark J Dobrow & Roger Chafe
You can also search for this author in PubMed Google Scholar
Corresponding author
Correspondence to Mark J Dobrow .
Additional information
Competing interests.
The authors declare that they have no competing interests.
Authors' contributions
All authors participated in the conception and design of the study. The key informant interviews and ITR process were carried out by VH. The audit was conducted by VH and MJD. VH prepared the original draft of the manuscript, and all authors reviewed and critically revised the original and subsequent manuscript drafts and approved the final manuscript.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Reprints and permissions
About this article
Cite this article.
Hagens, V., Dobrow, M.J. & Chafe, R. Interviewee Transcript Review: assessing the impact on qualitative research. BMC Med Res Methodol 9 , 47 (2009). https://doi.org/10.1186/1471-2288-9-47
Download citation
Received : 24 February 2009
Accepted : 06 July 2009
Published : 06 July 2009
DOI : https://doi.org/10.1186/1471-2288-9-47
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
Transcribing Interviews for Qualitative Research: Best Practices
Serra Ardem
The long hours dedicated to transcribing interviews are now in a galaxy far far away, thanks to the developments in AI and machine learning. Qualitative research highly benefits from these advancements as AI transcription technology not only saves valuable time but also increases research efficiency and accuracy.
In this blog, we emphasize the significance of transcribing interviews for qualitative research as well as the best practices in this area. We also explain why automatic transcription offers more advantages to researchers and how to choose an interview transcription software to achieve optimal results.
Let’s begin.
What is qualitative research?
Qualitative research is a systematic approach to understanding and explaining social phenomena. Focused on “How?” and “Why?” questions, it is an umbrella concept that involves different research methodologies including interviews, participant observation, focus groups and so on.
Qualitative data is based on words, behaviors and images. By analyzing these, qualitative research generates theories and hypotheses on how the social world is experienced and understood by people in everyday life. Unlike quantitative research that depends on numbers and statistics, qualitative research seeks to uncover the underlying meanings in human experiences.
Importance of Transcribing Interviews in Qualitative Research
Transcribing interviews for qualitative research offers several benefits that contribute to the overall depth and success of the research process. Here are its key advantages:
Comprehensive analysis: Transcripts capture every word, nuance and non-verbal cue, which is a goldmine for data analysis. This allows researchers to identify themes and patterns thoroughly to draw meaningful conclusions.
Enhanced reliability: Having the transcript for an interview will strengthen research validity by providing evidence to your argument. Plus, other researchers can review the transcription, ensuring transparency and collaboration.
Reduced bias: Transcribing interviews will reduce bias as it minimizes the risk of misinterpreting or omitting information. Compared to note-taking, which may be influenced by the researcher’s perceptions, transcription offers a more objective representation of data.
Increased accessibility: Via transcription , researchers can share and discuss findings with people who couldn’t participate in the interview due to language barriers. Furthermore, the practice improves accessibility for deaf and hard of hearing individuals by allowing them to engage with the findings through written text.
Time-efficiency: No more jumping back and forth in audio files! When you transcribe the interview, you can quickly search for and navigate to specific parts, saving time during the analysis phase.
4 Types of Transcription
Transcription can be grouped into four categories: verbatim, intelligent verbatim, edited and phonetic. Let’s take a look at each one’s pros and cons, and highlight the best choice for transcribing interviews for qualitative research.
Verbatim Transcription
Verbatim transcription includes every sound in the audio recording such as coughs, doorbells and hesitations (er, mm, etc.) between sentences.
Pros: Provides the most complete and accurate record of the interview, which is essential for capturing the full context and subtle nuances.
Cons: May include unnecessary details. Can be time consuming and expensive to produce in case of manual transcription.
Primarily used in: legal proceedings, sociolinguistic research studies
Intelligent Verbatim Transcription
An intelligent verbatim transcript removes filler words and repetitions but retains key content and non-verbal cues. Its purpose is to provide a more on-point transcript.
Pros: Offers a balance between readability and details.
Cons: May sacrifice some context and require careful quality control to guarantee accuracy.
Primarily used in: qualitative research, especially in interviews and focus groups
Edited Transcription
Clarity is the main focus of an edited transcript. It corrects grammatical errors and eliminates filler words, repetitions and extraneous sounds.
Pros: More readable and concise, therefore suitable for general understanding and thematic analysis.
Cons: Risks losing some nuances and the authenticity of participants’ expressions.
Primarily used in: journalism and media contexts
Phonetic Transcription
Phonetic transcription is unorthodox as it uses symbols from the International Phonetic Association to represent sounds exactly as they are spoken. This includes accents, dialects and non-standard pronunciations.
Pros: Analyzing variations in pronunciation.
Cons: More complex and expensive than other types of transcription.
Primarily used in: linguistic studies
What is the best type for interview transcripts in qualitative research? As we’ve said above, intelligent verbatim transcription is often the best choice: It is readable and manageable for analysis, yet it also provides a detailed record of the conversation.
Still, always consider your research goals, questions, data and budget when transcribing interviews. An edited transcript might be sufficient if you want to focus on broader themes. Meanwhile, verbatim transcription can be pretty useful if details matter to you a lot.
Methods of Transcribing Interviews
There are two main methods when it comes to transcribing interviews: manual and automatic. While manual transcription involves a human transcriber typing out the spoken words in the interview, automatic transcription utilizes speech recognition technology to convert audio to text.
As in types of transcription, these two methods have their unique advantages and disadvantages. Human transcribers can better understand nuances and context. However, this method can also be pretty time consuming and it may be expensive to hire a professional transcriber.
On the other hand, automatic transcription is much faster and cost-effective. This is an important advantage in the realm of qualitative research where large amounts of interview data need to be processed and analyzed. You can definitely save time and resources by using software when transcribing interviews for research.
Moreover, automatic transcription services are getting more accurate day by day thanks to the developments in AI, machine learning and voice recognition. Current systems can handle diverse accents, linguistic variations and even contextual nuances very well. This significantly increases the reliability of the interview transcript and research results.
How to Choose an Interview Transcription Software
Decided to use an interview transcription software for research but confused on how to choose one? Look for these qualities when making your decision:
Accuracy is crucial when transcribing interviews as it directly influences the reliability of your data. Prioritize an AI-powered tool with a high accuracy rate to remain true to your original interview. We recommend you test the AI transcription software beforehand with a small sample of your interview.
Quick turnaround time is essential for researchers who work with large sums of interview data and tight deadlines. The right software must transcribe audio to text rapidly without compromising accuracy and meet the demands of an intense qualitative research process.
It is your responsibility to comply with ethical standards and protect your participants’ sensitive information. You must choose a tool that has end-to-end encryption and clear privacy policies.
Flexibility
Does the transcription software allow you to upload audio and video files in different formats? Is it easy to edit the transcript and add notes? This flexibility will help you refine interviews seamlessly, enhancing the quality of your data.
Customization
Speaker identification, timestamps and punctuation are indispensable when transcribing interviews for qualitative research. Select a software that allows you to tailor these elements to your needs.
Language Support
Make sure that the tool supports the languages spoken in your interviews. Break down the language barrier by choosing a software that transcribes multiple languages and enrich your research with global perspectives.
Transcribing Interviews with Maestra Step-by-Step
If you’re looking for a tool with all these features, then Maestra’s AI-powered interview transcription software is the right choice for you. You can get your transcript instantly by following a few simple steps.
Upload your audio or video file. Maestra supports 125+ languages .
Select audio language and receive the transcript in seconds.
Custom dictionary is especially beneficial when transcribing interviews for research as the audio content is more likely to include technical terminology. With this feature, you can add specific terms to your custom dictionary, assign importance values and Maestra will transcribe them as specified, ensuring accuracy.
You can also select the number of speakers during the upload phase and assign names to each speaker, making it easier to navigate the transcript.
Click “Submit” and witness AI transcription work its magic. You will instantly receive your interview transcript with timestamps and speaker tags.
Ta-da! You can now proofread and edit your transcript, take notes and add comments with Maestra’s built-in text editor .
Maestra has a very high accuracy rate but you can always polish your document for maximum clarity and comprehensibility.
After transcribing interviews, you can safely reach and organize them via MaestraCloud . You can also store your interview recordings here as the cloud allows you to keep audio and video files of any size without time limitations.
Collaborating with fellow researchers? Maestra Teams is ready to help you. You can create team-based channels with different permission levels and edit the document with other researchers in real-time.
Tips for Transcribing Interviews for Qualitative Research
No matter your experience in qualitative research or the software you use, there are certain practices to adopt when transcribing interviews.
Use a High-Quality Recording Device
Utilizing a high-quality recording device lays a solid foundation for interview transcription. Invest in a reliable recorder with good microphone sensitivity and audio quality to capture every part of the conversation. Don’t forget to test your equipment beforehand to avoid potential technical issues during the interview.
Respect Confidentiality
Upholding confidentiality is paramount when transcribing interviews for qualitative research. Always obtain informed consent from participants for recording and transcription, and store your files securely. Avoid sharing any personally identifiable information to safeguard participant privacy and maintain the integrity of your research.
Include Speaker Identification and Time Stamps
This practice enhances the overall usability of an interview transcript by enabling easy reference to specific points. Make sure you clearly identify each speaker on the document either by name, role or pseudonym. You can use different fonts or colors to visually distinguish between speakers.
Follow the Specific Style Consistently
Choose a transcription style guide (verbatim, intelligent verbatim, etc.) and follow it consistently throughout the project. Define rules for punctuation, contractions and interruptions. This will guarantee uniformity and enhance the reliability of your findings.
Add Non-Verbal Cues and Annotations
This one is not mandatory but can provide valuable context. You can document non-verbal expressions, pauses or changes in tone to add depth to qualitative data analysis. Meanwhile, bracketed annotations can help you highlight important moments. Just remember that adding too much detail can be distracting, so only include relevant information.
Edit and Proofread the Transcript
Proofread and edit your document once transcribing an interview: correct any errors, format inconsistencies and review for readability. Double check speaker identification and timestamps for accuracy. These practices will ensure a smooth transition from transcription to analysis and publication.
Frequently Asked Questions
Is transcription necessary for qualitative research.
The necessity of transcription depends on the nature and goals of the qualitative research you conduct. For example, it is crucial for in-depth and focus group interviews but not essential for participant observation where researchers can rely on field notes.
How do you transcribe an anonymous interview?
When transcribing interviews with anonymous participants, remove any information that can directly or indirectly identify the participant such as name, nickname, location, job title and affiliations. Create neutral pseudonyms (Participant 1, Interviewee A, etc.) for the participant and use them consistently throughout the interview transcript.
How do you analyze interview transcripts in qualitative research?
First, familiarize yourself with the data through readings when analyzing an interview transcript for research . Then, assign codes to relevant segments and organize similar codes into broader recurring themes. Finally, present your findings via a structured narrative. Always maintain transparency during the process.
How do you transcribe an interview in APA format?
Transcripts of interviews are usually added to the appendix in APA format . You should use a specific header with interview details, double line spacing and speaker identifiers in the transcript.
How do you summarize an interview transcript?
Carefully read the content and identify key themes when summarizing the transcript of an interview . Organize the information logically, provide brief contextual details when necessary and use quotes to add impact. Capture the essence of the interview by keeping the summary short and sweet.
Interview transcription is particularly valuable in qualitative research, which delves deep into human experiences and perceptions. Transforming spoken words into text enables researchers to derive meaningful insights from the rich tapestry of qualitative data. It also increases the accessibility of the research, empowering scholars to collaborate with colleagues across disciplines and borders.
The advent of AI technology revolutionized the process of transcribing interviews and will continue to do so in the future. Its benefits range from increased accuracy to cost-effectiveness, providing a much refined experience for researchers. By choosing the right software and adopting the best practices for transcribing interviews, researchers can unleash the full potential of their endeavors.
About Serra Ardem
Serra Ardem is a freelance writer and editor based in Istanbul. For the last 8 years, she has been collaborating with brands and businesses to tell their unique story and develop their verbal identity.
We Trust in Human Precision
20,000+ Professional Language Experts Ready to Help. Expertise in a variety of Niches.
API Solutions
API Pricing
Cost estimate
Customer loyalty program
Educational Discount
Non-Profit Discount
Green Initiative Discount1
Value-Driven Pricing
Unmatched expertise at affordable rates tailored for your needs. Our services empower you to boost your productivity.
Special Discounts
Enterprise transcription solutions
Enterprise translation solutions
Transcription/Caption API
AI Transcription Proofreading API
Trusted by Global Leaders
GoTranscript is the chosen service for top media organizations, universities, and Fortune 50 companies.
GoTranscript
One of the Largest Online Transcription and Translation Agencies in the World. Founded in 2005.
6 Easy Steps in Learning How to Analyze Interview Data in Qualitative Studies
It’s understandable if you find qualitative data analysis quite challenging. Unlike quantitative methodologies, qualitative data analysis doesn’t follow a systematic, rigid, and formulaic process. Once you decide to analyze interview transcripts in qualitative research, the work is slightly more intuitive than tangible.
We won’t sugarcoat things and say that qualitative analysis is an easy task. However, there are practical steps you can take to avoid turning the entire process into something chaotic. In most cases, you’ll start by having accurate interview transcripts that you need to read over and over again.
This article will guide teach you how to transcribe and analyze interview data for qualitative research.
Why It’s Important to Analyze Interview Data in Qualitative Research
Quantitative data may offer rigor to your research. However, it is qualitative analysis that will add color to your business or academic report. By taking this approach, you can add context to your data and make it more readable. It will inspire a more meaningful discussion that goes beyond the hard numbers in your report.
Most of the time, interviews allow you to acquire subjective data from direct sources. As a researcher, you’ll get relatable perspectives and stories. You can also get important quotes from subject matter experts. Interviews provide qualitative data that strengthens the integrity and eliminates embellishment in their research.
Now, how do you acquire the information you need for qualitative data? Well, transcribing interviews provides you with the best resources for qualitative analysis. You can add life to your research by interviewing the following sources:
Business leaders
Scientists and investors
Trial or study participants
Journal and research authors
You can include sources that may contribute to the quality of the research. Now, whenever you conduct an interview, you should use the right methods to ensure you’ll get the information you need. You must maximize your recorded interviews by transcribing them accurately.
How to Get an Accurate Qualitative Interview Transcript
It’s more challenging to get the information you need in a qualitative interview. However, by taking a systematic approach, it will be easier for you to gather the data you need. Here are some steps to follow:
1. Gather Qualitative Data
Qualitative data can be collected through various means. For one, you can record the interview and take advantage of legal-grade transcription services. Taking this approach will help you avoid data loss and inaccuracies. This method is ideal for focus group discussions and customer interviews. With this process, respondents can be more open in answering the questions.
You may have above-average note-taking skills, but that’s usually unreliable in qualitative research. Whether you’re conducting the interview over the phone, on a video conference call, or in person, you can collect accurate data by recording the conversation. You can either record the interview in an audio-only or video format.
2. Compile Your Interview Recordings Neatly
Your interview video or audio files should be easy to find, identify, and share. Use file-naming conventions that are easy to recall and organize. Ideally, you must include the date of the interview, the source’s last name, and the discussion topic.
No matter what file naming convention you choose, you need to be consistent in the format. This way, it’s easier for you to find the necessary files later when you analyze interview data.
3. Transcribe the Focus Group and Interview Recordings
The next step is to transcribe the recordings. Now, there are plenty of tools online that can automate the process. However, remember that you are working on qualitative research, and you need an accurate transcription.
So, your best bet here is to use 100% human-generated transcription services. GoTranscript offers verbatim results, allowing you to get legal-level accuracy for your qualitative interview recordings. If you’re following tight deadlines, you can opt for a rush order. This way, you’ll get your files within your requested turnaround time and begin your qualitative analysis.
What Are the Methods Used to Analyze Interview Data in Qualitative Research?
When it comes to qualitative data analysis, you can choose from two primary approaches – inductive and deductive. If you opt for the former, you can take an unstructured approach to your research by conducting narrative or thematic content analysis.
Inductive Method for Analyzing Qualitative Interview Transcripts
Thematic content analysis – This method starts by identifying your overarching impressions of the information and weeding out biases. Instead of establishing a framework for approaching the data, you search the materials organically and look for common themes. You aim to discover the recurring patterns across the data set.
Narrative content analysis – This method requires you to make sense of the individual stories of your interview respondents. It is the ideal approach for identifying important aspects of the data that resonate well with your readers.
Deductive Method for Analyzing Qualitative Interview Transcripts
Deductive data analysis is a more systematic or structured approach. Before you begin to analyze interview data, you need to develop categories. During the process, you’ll connect information from the data to those pre-determined categories.
Both approaches to data analysis bring benefits to your research. If you want more nuanced findings, the inductive method is the ideal option. Now, if you want to point to key themes that are crucial to your research, opt for deductive analysis.
6 Practical Steps in Performing Qualitative Analysis of Interview Transcripts
Most of the time, researchers opt for thematic content analysis. Many find it to be the most effective and trustworthy method. The approach makes it easier for anyone to verify and trace the findings of the analysis. Here are six practical steps for conducting a thematic analysis of your interview transcripts:
Step 1: Go Through the Transcripts Carefully
At this point, you likely have a digital copy of your transcript files. You may have them stored locally on your computer or in the cloud. Begin by skimming through the transcripts, and along the process, write down your first impressions. This makes to easier to analyze interview data.
Taking this approach will help you identify common patterns in the data. Your quick notes will also be instrumental in helping you come up with a final summation of the data.
Now, you need to read every transcript carefully. After multiple run-throughs, the common themes will become more visible. As a result, you will be able to come up with crucial and significant insights.
During this process, you should also identify biases. Even within your methodologies and objectives, biases will surface in the data and among the interviewees. Sage Publishing recommends that as early as this step, you should actively neutralize the preconceived notions you identify. This way, you can take an objective approach when you begin to analyze interview data.
Step 2: Begin Annotating the Transcripts
Once you get to this step, you need to label the key phrases, terms, sentences, or section codes on the transcript. Annotating your transcripts allows you to identify important qualitative data patterns and types.
The labels can highlight the varying interviewee opinions, concepts, and data differences. This process makes it easier for you to organize your data set for dissemination. As a result, you’re cutting down the time it takes to analyze interview data.
Step 3: Align the Data with Important Themes
This step requires you to conceptualize the qualitative data by aligning it with important themes for your final content. At this phase, you will have identified the common patterns from the initial transcript reviews.
When conceptualizing the data, you need to group the codes from the annotation to create categories and subcategories. You can combine or eliminate certain codes instead of using all of them. You should identify and retain the codes that are relevant to your analysis.
Step 4: Position and Connect Your Categories
Now, you need to segment the data by positioning and connecting your categories. During this step, you will be able to cohesively establish most of your data. You can begin by labeling the categories, and describing how they connect to each other. The descriptions will be instrumental in optimizing your final output. Here are the steps you can take:
Compile your data conveniently by using a spreadsheet.
Structure the data’s critical variables by labeling the columns with proper reference codes.
The document containing the coding table should be on a separate tab. This tab functions as a glossary containing critical codes for the segmentation process. As a result, you can quickly identify what the codes are referring to.
Most researchers prefer doing all these steps electronically for convenience. However, some people prefer having a printed copy so they can highlight segments using pens. In any case, you should save a copy of the transcript files. You can print them out when you need to.
Step 5: Perform a Deep Analysis of the Data Segments
Once you’ve segmented the data, it’s time to perform a deep analysis. You can begin by identifying the categories’ hierarchy. You need to decide if one category is more important than the other. You can also summarize the results by drawing a figure. This stage should also let you align the qualitative data with your quantitative data.
Step 6: Write Your Findings
Once you’ve performed a deep analysis of your data, you’re ready to write the results into a body of content. Establish and verify theories by using your data insights. You can also answer key questions that your field may ask, and don’t forget to adequately support your research goals. Use an objective, neutral voice in describing how your categories connect to each other.
Naturally, you will use your own research and pull insights heavily from it. However, make sure to consider the context of your field when writing your results. Interpret your findings alongside relevant theories, studies, and concepts when you analyze interview data.
Accurate Transcription Is Necessary in Qualitative Research Analysis
Researchers often find qualitative data analysis challenging. As such, it is important to have transcripts that capture the nuanced, unadulterated responses from interviewees. You can get their organic responses because they are using their own words and not the shortened version from your notes.
What’s great about having a transcript is that you can go back to it whenever you gain find new context. However, to ensure a reasonable level of objectivity, you must ensure that your transcript is accurate.
With GoTranscript, you can have a convenient yet efficient way of transcribing your qualitative interviews. You can save time and focus on more important aspects of your research.
“The interviews were transcribed”, but how? Reflections on management research
RAUSP Management Journal
ISSN : 2531-0488
Article publication date: 30 September 2019
Issue publication date: 9 December 2019
In qualitative research, it is recurrent to conduct data collection through interviews, which must be first transcribed for the data to be analyzed. Although there is a relationship between the stages of the interview and the data analysis, the link between them (i.e. the transcription) seems to be a neglected methodological procedure. This occurs because, in papers, it is generally reported that “the interviews were transcribed”, without any details about the transcriptions conduction. From this methodological gap, this paper aims to discuss the relevance of detailing the methodological procedures adopted in the transcription in research reports in the management field.
Design/methodology/approach
This paper takes the form of a methodological essay.
The discussion focuses on the concepts of naturalized and denaturalized transcription, the relevance of adopting transcription norms and the need for reflexivity in conducting transcriptions – elements that must be explained in research reports to improve the methodological quality.
Practical implications
This paper explores methodological details that management students and researchers can adopt when performing transcriptions. Consequently, journal editors and reviewers will have more subsidies on the methodological quality employed in researches, which contributes to a better evaluation process.
Originality/value
This study demonstrates the relevance of a neglected methodological technique – transcription, which needs to be detailed in research reports, to contribute to the increase of methodological accuracy and to provide essential information to readers, allowing them to evaluate the rigor of the research. Thus, it is proposed that transcription should be considered a quality criterion in qualitative research.
Transcription
Methodology
Qualitative research
Naturalized transcription
Denaturalized transcription
Nascimento, L.d.S. and Steinbruch, F.K. (2019), "“The interviews were transcribed”, but how? Reflections on management research", RAUSP Management Journal , Vol. 54 No. 4, pp. 413-429. https://doi.org/10.1108/RAUSP-05-2019-0092
Published in RAUSP Management Journal . Published by Emerald Publishing Limited. This article is published under the Creative Commons Attribution (CC BY 4.0) licence. Anyone may reproduce, distribute, translate and create derivative works of this article (for both commercial and non-commercial purposes), subject to full attribution to the original publication and authors. The full terms of this licence may be seen at http://creativecommons.org/licences/by/4.0/legalcode
1. Introduction
The qualitative research has a set of specificities and characteristics that, notably, in the Social Sciences, runs through numerous philosophical conceptions based on a range of data collection, analysis and interpretation methods ( Creswell, 2010 ). This variety of techniques and procedures inherent in the scope of qualitative research is detailed in the method section of reports (e.g. papers, dissertations and theses) that originated from scientific investigations. Such description is essential for rigor analysis ( Gioia, Corley, & Hamilton, 2012 ), reliability analysis and validation analysis ( Flick, 2013 ) used in studies, because it reflects the acceptability of the research by its readers ( Mitchell & Clark, 2018 ).
Specifically, in the management field, there is a concern with the rigor used in researches ( Bertero, Alcadipani, Cabral, Faria, & Rossoni, 2013 ), which can be exposed and analyzed from the description of the method or from the methodological procedures used in studies. In this way, when elaborating scientific documents, there is a prerogative that the authors attempt to explain the methodological approaches adopted in the research, pointing out characteristics, possibilities and limitations of the adopted techniques or methods ( Gerhardt & Silveira, 2009 ).
This detailing becomes even more relevant in qualitative research since it presents specificities and restrictions ( Cavalcanti, 2017 ) that prevent the generalization of results, as many authors postulate ( Mattos, 2011 ). Before the reader's acceptance, the evaluation process of scientific works, especially papers, requires the agreement of the study between the peers, which occurs through the justification, the contribution and the relevance of the research ( Lukosevicius, Guimarães, & Zouain, 2019 ), as well as through the description of the methodological course adopted.
The methodological description includes several steps, one of which being data collection, that occurs in qualitative research mainly through interviews, observation or documents ( Creswell, 2010 ). The interview is a privileged technique of data collection in qualitative studies ( Duarte, 2004 ), especially in the management field and it is understood to be a form of non-standardized research with the objective to obtain individual views of certain interviewees or respondents on a specific thematic ( Flick, 2013 ). There is a variety of interview styles for data collection ( Gerhardt, Ramos, Riquinho, & Santos, 2009 ) and the methodology manuals (e.g. Gil, 2007 ) usually detail the procedures that researchers must adopt before and during each interview.
This demonstrates the methodological relevance of conducting interviews and the need to clarify the steps and procedures adopted with this technique, such as the question of validation and acceptance of the research, as well as other techniques and methods of qualitative research. After delimiting the procedures to conduct the interviews, it is common to detail the procedures adopted for the data analysis of the elements of the interviews, through the methods of content analysis ( Bardin, 2016 ; Flick, 2013 ) and discourse analysis ( Caregnato & Mutti, 2006 ; Gonçalves, 2016 ), which are widely adopted in qualitative research. It is also necessary to detail the course followed in executing the analysis based on these methods, the same way it is done with interviews.
However, even with the advancement of publications in management ( Lukosevicius et al. , 2019 ), it seems that there is still no concern in this field with the transition stage between the interviews and the analysis in qualitative research, i.e. the transcriptions. Every research involving the conduction of interviews also involves the transcription of the conversation into text to facilitate the analysis process, as well as to expose the reports or quotes to readers. Yet, qualitative studies in management do not usually emphasize the transcription technique in method sections, and generally, there is only a simple sentence saying that “the interviews were transcribed”. Therefore, some questions about the transcription technique emerge: How were the interviews transcribed? What are the procedures for transcription? What are the limitations? What guarantees the quality of a transcription?
About these issues, it is relevant to emphasize that some methodology manuals adopted in the management field do not detail the procedures that should be used in conducting transcriptions. When analyzing the books of Creswell (2010) and Flick (2013) , which are widely spread and used as methodological guides in management graduate programs in several universities, it is noticed that the authors do not describe the transcription technique. In the few cases in which the transcription is cited in these works, it appears as a necessary action (for conducting data analysis), but that, a priori, has no significant relevance since it is not discussed.
Considering the methodological gap presented, this paper aims to discuss the relevance of detailing the methodological procedures adopted in the transcription in research reports in the management field. This research is based on the understanding that many times, and without apparent justification, the transcription is not discussed in works of methodology in Social Sciences ( Farías & Montero, 2005 ), especially in the management field. This can lead to an (erroneous) understanding of transcription as an objective and pragmatic action ( Davidson, 2009 ). Instead of an objective action, transcription is a representational process immersed in the subjective interpretation of the researcher ( Bucholtz, 2000 ), requiring reflexivity of the person who is conducting the transcription process ( Oliver, Serovich, & Mason, 2005 ).
Thus, this study shows the different aspects that permeate the transcription technique and the way that detailing the procedures can further increase the qualitative research validity in the management field. Such understanding goes beyond the purely theoretical debate since it becomes essential to construct scientific reports. Therefore, this paper contributes to the methodological description that management students and researchers can adopt when making transcriptions.
Based on this detailing, especially in scientific papers, the editors and reviewers of management journals will have more elements on the methodological quality employed in qualitative research, which will contribute to the evaluation process and the acceptance of papers. In addition, this study collaborates to the stimulus of the analytical spreading of an important technique of qualitative research ( Davidson, 2018 ) that has not yet received attention in management studies.
This paper is characterized as a methodological essay, i.e. a theoretical essay oriented to a methodological discussion or approach. Thus, it is independent of empirical evidence and has an amorphous structure ( Soares, Picolli, & Casagrande, 2018 ). Besides that, this methodological essay focuses on the development of reflections that impact the essential discussions for the advancement of the (administrative) science, and the orientation of this type of study is not based on a search for true answers and statements, but on questions that guide and assist people to have deeper thoughts on certain aspects ( Meneghetti, 2011 ).
Structurally, in addition to this introduction, the characteristics of transcriptions are presented and the applicability of that is discussed using two techniques. Also, the relations of these transcription techniques with content analysis and discourse analysis are described, and it is demonstrated how transcription has been neglected in management studies. Thus, the paper seeks to call the students and researchers’ attention to the potential of the methodological description of transcriptions as a way to improve the rigor of qualitative research in management, i.e. it is proposed that transcription should be considered a quality criterion in qualitative research.
2. What is known about transcriptions?
In qualitative studies, researchers, especially in the Social Sciences, use interviews as a way to discover or interpret the meaning of certain events or facts reported by informants ( Farías & Montero, 2005 ). Interviews can be understood as a social rhythm ( Kvale & Brinkmann, 2009 ) or an interactional event ( Mondada, 1997 ) between actors, based on realities and cultural language practices that may be different for the actors involved in the process. In this way, the linguistic constructions that occur in the scope of the interviews are developed through socio interactional processes ( Santos, 2012 ), where the (social, cultural or political) reality of each actor is modified, constructed and/or deconstructed amid the reciprocal influence of language and personal values.
It is possible to affirm that interviews are socio-cultural constructions based on the subjectivity of the involved actors, requiring the attention of the researchers to perform interpretative actions of the meanings coming from the interviews. This interpretative process is part of the data analysis stage, but for the analytical deepening, it is necessary to transcribe the interviews (that are usually recorded), which is a central practice in qualitative research ( Davidson, 2009 ). At the same time, the transcriptions present many complexities and can be performed through different routes ( Oliver et al. , 2005 ). Thus, transcription seeks to transpose meanings and sociocultural representations from a spoken language to a written language ( Ong, 1982 ), being a process permeated by social, cultural, political and epistemological judgments of the researcher ( Kvale & Brinkmann, 2009 ).
Historically, studies about transcription emerged in Linguistics’ field as the seminal work developed by Ochs (1979) . Currently, many fields in Social Sciences, such as management, adopt transcriptions in qualitative research. In relation to the concept, the transcription literature provides many definitions of transcription ranging from the perspective of conversation analysts to researchers in linguistic anthropology and sociolinguistics ( Davidson, 2009 ). For Davidson (2009) , the different definitions come to a common understanding, in which the transcriptions are understood as data used by researchers, being developed through a selective process composed by definitions and reflexive theoretical objectives ( Ochs, 1979 ).
The transcription has been used over time as a way to show evidence about certain phenomena that constitute research interest in a study ( Duranti, 2006 ). The author states that transcription can be understood as a cultural practice. From this perspective, it is possible to infer that the act of transcribing can be influenced by cultural characteristics related to an institutional environment, academic environment and the background of the researcher who conducts the transcription process. Thus, a researcher from the north region of a given country can transcribe an interview, and the transcript will have certain characteristics that are not present in another transcript coming from the same interview, but transcribed by a researcher from the south region of this country.
This distinction occurs because of cultural differences, showing that transcription should not be understood and conducted as a mathematical process, in which there is a path to follow and a single result to achieve. That is, the act of transcribing is not a static process, but it is permeated by several factors that can influence the configuration of the transcript. This is consistent with Bucholtz's (2000) view of transcription as an interpretive process about what is transcribed and how it will be transcribed. In this way, it is possible to affirm that reflexivity is an inherent component of the transcription process, as stated by Bucholtz (2000) and Oliver et al. (2005) , which leads to the understanding of transcription as a process not only objective (in certain aspects), but also subjective ( Bucholtz, 2000 ), since it characterizes a representational procedure (the transcript) of the data coming from the interviews that are shaped by the researcher ( Green, Franquiz, & Dixon, 1997 ).
The act of transcribing can be based on certain pragmatic logics since they can facilitate the reader's understanding. For example, if the interviewee speaks with a very low voice, it will probably not be possible to understand some words recorded in the audio. Hence, in the transcript, the researcher will need to inform the reader about this situation, which can be demonstrated by the following expression: “(incomprehensible)”, as Marcuschi (2007) argues.
Thus, it is perceivable that objectivity is part of the transcription process, as well as subjectivity, since in the mentioned case above, if the researcher hears the recorded audio again and realizes that the respondent said a certain word but is not sure, the researcher can put this word in parentheses in the text, stating that there is no certainty that the word was spoken ( Marcuschi, 2007 ). This example demonstrates the subjective nature of the transcription, because another researcher can listen to the same audio and understand a different word, and with this, two transcripts from the same interview and its respective recording may present different words, putting in risk the meaning of the transcription and, consequently, the result of the data analysis.
Deepening the discussion about the need of standardization (objectivity) for a better understanding of transcription by readers, Marcuschi (2007) presents some norms that can be adopted in the transcription process. The norms are relevant to the transcription process because they help to minimize inconsistencies that may arise due to technical issues of the recording equipment and to noise or interferences that occur during the interview ( Farías, & Montero, 2005 ; Oliver et al. , 2005 ).
Based on the norms postulated by Marcuschi (2007) , it is possible to format the transcript so the reader can understand the adopted situations by the researcher when transcribing the interview, being evident in the transcript, for example, when the respondent emphasized a word. Some of the norms described by Marcuschi (2007) were grouped in Table I , along with the presentation of some illustrative examples of the application of the norms in transcripts. It is necessary to emphasize that many other norms are described in the work of Marcuschi (2007) , but this paper does not intend to discuss such norms, only to emphasize their relevance.
Besides Marcuschi’s (2007) work, there are other works (e.g. Atkinson & Heritage, 1999 ; O’Connell & Kowal, 1994 ) that discuss standardization in transcription (i.e. notation or norms) and it is relevant for the researcher to inform in the research report the source of the norms that supported the transcription. Thus, the reader is not taken by surprise when encountering unknown symbols in a report from a transcribed speech, because the reader will have the source information of the adopted norm and will be able to consult it. Also, the researcher can use some norms of Marcuschi (2007) , for example, and some norms from other works in the same transcript, as long as the researcher makes clear to readers the sources used and the rules corresponding to each author (work). Likewise, the researcher can create transcription norms, considering that the researcher explicitly informs and, if possible, graphically presents such norms created for the reader’s better understanding.
Although transcription norms are pragmatic concerning standardizing the transcription process, there will always be specific questions that require subjective actions in the transcription process. An example of that is the researcher's decision to present the written text as it was spoken (tending to a more natural or informal language, if any) or making adaptations between what was said and what was written to present a text in accordance with the language’s norms (formal language). Such reflections are essential in defining transcription, and they form the core of the following discussion.
3. Naturalized and denaturalized transcription
There are two basic types of transcription: naturalized and denaturalized, and they often represent extremes in the variety of transcription options ( Bucholtz, 2000 ). These positions correspond to two language representation views ( Oliver et al. , 2005 ). Both forms of transcription have the potential to serve as politicized tools of linguistic representation and, in some cases, are more similar than different ( Bucholtz, 2000 ). The discussion on this theme takes shape from two main views, which may be contradictory and at the same time, complementary. These views are here denominated as theoretical perspectives.
3.1 First perspective – the view of Bucholtz (2000 )
In the denaturalized transcription , the text has links with the forms of the oral discourse, making that, due to its fidelity to the spoken language, the written text loses sense in some cases and this ends up generating a paradox of using written texts to represent spoken languages ( Bucholtz, 2000 ). When the transcription is denaturalized, a description of the speech’s details occurs, and they are also exposed in the written report ( Bucholtz, 2000 ). In such cases, oral details are included through technical transcription systems – norms. Thus, denaturalized transcription preserves the characteristics of oral language ( Davidson, 2009 ). With that, the text that reflects a speech ends up being less comprehensible for readers who are not accustomed to finding oral discourse characteristics in a written text ( Bucholtz, 2000 ). For this author, the more the text reflects the “orality” of the speech, the less transparent and clear it will be for readers who are not used to interpreting oral characteristics in a written text.
In naturalized transcription , the text is in agreement with the written discursive conventions (formal language); that is, the written oral discourse is privileged. The risk in this type of transcription is not emphasizing enough the linguistic form and its transformation from the speech to transcripts ( Bucholtz, 2000 ). The naturalized transcription occurs when the written characteristics of the speech take precedence over those of the speech; therefore, the description of the interviews has many characteristics of the written language that, in fact, do not occur in the spoken dialogue, like commas, long stops and sentence completion ( Davidson, 2009 ).
3.2 Second perspective – the view of Oliver et al. (2005 )
Contrary to what was suggested by Bucholtz (2000) , Oliver et al. (2005) believe that in naturalized transcription , the whole sentence is captured with as many details as possible. Thus, this transcription represents a “real world” approach ( Cameron, 2001 ). In naturalized transcription, speech is expressed as it is, without being overly filtered by transcribers ( Oliver et al. , 2005 ). The goal is to present the data in a natural, objective and accurate manner. This naturalized view of the conversation is captured in the transcription structure and in the discourse representation itself ( Oliver et al. , 2005 ). This kind of transcription is suitable for those researchers who are interested in oral language intricacies. Oliver et al. (2005) point out that the effect of naturalism can alter our understanding of the social context of discourse because when naturally transcribing a recorded interview, assumptions can be made about what is standard and what is non-standard. According to the authors, a naturalistic approach provides details that may obscure substantial interview questions, and this may have some impact on data analysis.
In the opposite, denaturalized transcription preaches the constant grammar correction, the removal of the existing noises in the interviews and the standardization of non-standard speeches and accents ( Oliver et al. , 2005 ). According to these authors, this transcription results in “clean” data, which is free of socio-cultural characteristics and information, and may even improve the study results. This approach also suggests a textual description of speech, and although it seeks a complete and faithful transcription ( Cameron, 1995 ), denaturalized transcription does not consider the accents of involuntary vocalization and the representation of it in speech ( Oliver et al. , 2005 ). In other words, for denaturalization, precision is fundamental for the interviews’ transcription, pondering the meanings and perceptions made during the interview ( Oliver et al. , 2005 ).
Based on the arguments listed in both perspectives, the concepts of naturalized and denaturalized transcription are synthesized in Figure 1 .
As shown throughout this section, the two perspectives share similar and complementary views on the same phenomena (the two transcription techniques), since the concepts (naturalized and denaturalized) given for each phenomenon are inverse if the two perspectives are compared (according to subtitles 1 and 2 of Figure 1 ). This is clearly illustrated in Figure 1 , because the concept of naturalized transcription for Bucholtz (2000) is the same as the one of denaturalized transcription for Oliver et al. (2005) , and this inverse logic also occurs in the understanding of denaturalized transcription for Bucholtz (2000) and its equivalence to naturalized transcription for Oliver et al. (2005) .
How to proceed when facing this confusion of concepts? To minimize this confusion, it is necessary to understand that transcription is a cultural practice ( Duranti, 2006 ), in which the researcher needs to recognize and be sensitive to the linguistic and cultural nuances of transcription as a social practice ( Marcuschi, 2007 ). In this way, transcription can be understood as a cultural activity in which its transcript has a socio-historical character and can be considered a cultural artifact ( Duranti, 2006 ) capable of relating the linguistic form to the social world ( Jaffe, 2000 ).
From this understanding, it can be deduced that even though Bucholtz's (2000) work introduces the perception of transcription as a sociocultural practice ( Jaffe & Walton, 2000 ), the conceptual essence of naturalized transcription adopted by that author is not a purely cultural understanding, since it starts to denote a pragmatic (and even hegemonic) understanding supported by formal language.
On the other hand, the concept of naturalized transcription from Oliver et al. (2005) , which is related to informal language (a socially and culturally practiced in everyday life), better denotes the character of transcription as a cultural practice. Such understanding comes from the fact that formal language is preceded by the informal language, since linguistic variations arise in everyday practice and over time are legitimized and institutionalized as a standard, that is, formal language.
In this way, the concepts used in this paper (naturalized and denaturalized) are the ones proposed by Oliver et al. (2005) , because they better represent the role of transcription as a process permeated by the knowledge of social, political and cultural dynamics ( Pelzang, & Hutchinson, 2018 ) specific to a research context. Having clarified the confusion of concepts, it is important to note that the work of Bucholtz (2000) is complementary to that of Oliver et al. (2005) , as shown in subtitles 3 and 4 of Figure 1 . Thus, the concept of naturalized transcription ( Oliver et al. , 2005 ) is complemented with that of denaturalized ( Bucholtz, 2000 ) transcription, because they are congruent (according to subtitle 3 of Figure 1 ) and vice versa for denaturalized ( Oliver et al. , 2005 ) and naturalized ( Bucholtz, 2000 ) transcription (according to subtitle 4 of Figure 1 ).
3.3 Naturalized or denaturalized: is there a better technique?
On the one hand, the transcription classified as naturalized ( Oliver et al. , 2005 ) can generate conflicting interpretations, because readers who are not accustomed to deciphering these interventions in the dialogue, such as noises, pauses in speech, slang, accents, etc. end up decoding these elements in the way they believe are the best, and this can cause different understandings from the same study.
However, by leaving the interview in its purest and least altered form, the researcher would be as transparent as possible with the readers to demonstrate the reason for the analysis. By keeping the transcripts on their original form, respondents end up speaking for themselves ( Schegloff, 1997 ), since dialogue is not simply an exchange of ideas, but it also involves verbal and non-verbal cues that can alter the tone of the conversation and, consequently, its meaning ( Oliver et al. , 2005 ).
On the other hand, when considering the denaturalized transcription ( Oliver et al. , 2005 ), the author interprets what was said, the way it was said, the noises and interferences in speech, being responsible for this understanding, making the necessary adjustments in the transcription and passing this data to readers, thus everyone will have the same view of what was said. However, depending on the author who does this refinement of the interviews, the results may vary, as well as the data analysis.
Therefore, the great dilemma between the two transcription techniques lies on how much the researcher wants to make the details and the interferences of the interview available and on how much they believe these elements are relevant to the study. This choice considers that, inevitably, transcription is an act of power, since it consists of interpretation and representation actions, involving the context in which speech is inserted ( Bucholtz, 2000 ).
Additionally, it is not possible to develop a perfect transcription process with no ideological positions and personal interpretations ( Bucholtz, 2000 ). For this author, the act of transcribing is authorial and requires creativity, because it considers that humans are not machines, but people who interpret a text and therefore select the most important points according to their own view (or epistemology). Hence, Bucholtz (2000) believes that the act of transcription must be done with responsibility, but not necessarily with neutrality. However, in this paper, it is understood that the choice made should be clearly exposed to readers, as a transparency action, allowing them to discern on the methodological course adopted and have a basis to critically reflect the level of the methodological rigor used (in the process of transcription).
That said, the best technique of transcription is […] wait! There is no technique better than the other! The choice of one of the techniques is dependent on the researcher's reflexivity ( Oliver et al. , 2005 ) and there may be even a half term – using a mix of the two techniques in the same transcription. Regardless of the option, this should be explicitly informed to the reader, as discussed previously. Even if the option is made by the researcher, there are some factors that induce the use of one technique or another, such as the method of data analysis, which is discussed below.
4. Naturalized and denaturalized transcription, norms of transcription, content and discourse analysis: plausible relations
The techniques of naturalized and denaturalized transcription come from the method of data analysis that was defined in the methodological course, being emphasized those of content analysis and discourse analysis. These methods were selected (among many others) because they are widely used and known in qualitative research in the management field, contributing to a better understanding of the relations here discussed. A priori, these relations may sometimes not be identified by the researcher, and this ends up generating an incongruence (little noticeable for some researchers) between the method of analysis and the technique of transcription prior to this stage.
A method of data analysis is a form of interpretation, having specific procedures or techniques that prepare the data for the analysis, since this process aims to make sense in texts ( Creswell, 2010 ). Clearly, the choice of the most appropriate analysis procedure depends on the study purposes, the researcher's ideology and, of course, on the analyzed data ( Chizzotti, 2006 ). Referring to a reverse flow to what was proposed by Chizzotti (2006) , it is believed that the adoption of a transcription technique depends on the method of analysis employed. Therefore, after going through all the methodological planning until the decision by the method of analysis that best fits the research, the researcher must return to the previous stage and decide if it will be used naturalized or denaturalized transcription.
How to know which transcription technique is most appropriate for a given method of analysis? The literature already points to discussions that help in this decision, because as Davidson (2009) states, several methods of analysis can be related to the two transcription techniques. As Oliver et al. (2005) suggest, discourse analysis is related to denaturalized transcription. However, it is argued that such a relationship is fragile (and even incompatible), because it is understood that the discourse analysis has a direct relation with the naturalized transcription , according to the arguments that follow.
This relation is possible because the discourse analysis tries to ponder the mechanisms of domination that are hidden under the language ( Orlandi, 2013 ). The discourse analysis studies words and expressions as well as their form and structure, the use of language, context, interpretations and meanings of discursive practices ( Putnam & Fairhurst, 2001 ), given that it seeks inference through discursive surface effects ( Bardin, 2016 ).
Thus, in the discourse analysis, there is something (subjective and implicit) that goes beyond what was simply said or written, since it investigates how the content is used to achieve a certain effect, is imperative that the researcher has the sensitivity of capturing different subjective interpretations and implied speech in a discourse ( Vergara, 2012 ). That is, to capture the essence of a discourse, it is necessary to analyze it also from the expressions that were spoken or expressed physically by the interviewee. This can only be demonstrated in the transcript from the literal transcription of the interview, without modifications adapting the text to the formal language, that is, the naturalized transcription.
Therefore, language addictions, slangs, syllabic repetitions and even facial expressions or body movements are able to indicate the presence of emotional situations that can reinforce or contradict the words said by the respondents, leading to certain inferences during the analysis. And in order for the researcher to have access to this information in the discourse analysis stage, it is necessary to develop the transcription in a naturalized way.
Just as discourse analysis is for naturalized transcription, content analysis is for denaturalized transcription . Content analysis includes the explanation, systematization and expression of speech content so that logical deductions can be made according to the context of these speeches, and to who issued them and what effects are intended ( Bardin, 2016 ). This method relates the semantic structures to the sociological structures of the statements and analyzes the texts in a way that it is possible to identify their characteristics ( Minayo, 2001 ). The purpose of the method is to understand the meaning of the communications performed, the manifest and latent content, as well as the meanings in the speech ( Chizzotti, 2006 ), which allows to treat the collected data in a way that it is possible to identify the meaning of what was said ( Vergara, 2012 ).
In this way, while the discourse analysis focuses on the sense of discourse, the content analysis focuses on the content of the text ( Caregnato & Mutti, 2006 ), not being much relevant for the latter, for example, the expressions of informal language or other emotional aspects expressed by respondents during an interview. Thus, there is no need to perform a naturalized transcription, which allows the researcher to use reflexivity to leave the text in accordance with the formal language and extract the necessary analytical content to conduct the research.
And where transcription norms enter into these relationships? Norms, like those postulated by Marcuschi (2007) , are essential for the naturalized transcription, because they help to include spoken phenomena in the written text, which will help the conduction of discourse analysis, for example. Thus, it is relevant to use norms to demonstrate when the respondent repeats certain expressions such as “hm […] hm […]”, which may indicate that the respondent is uncertain about the response or speech. Also, the writing of this repetition assists in conducting inferences in discourse analysis, leaving such inference in a clear way (by demonstrating the interview reports or quotes) to the readers of the research report.
In the content analysis, because there is no need to detail informal expressions of the language, the norms are not faithfully followed, since denaturalized transcription prevails. However, it is understood that some norms are necessary for this type of transcription, as the indication that at a certain moment the researcher did not understand a word that the interviewee said, as the use of (incomprehensible). In addition, if the transcript highlight slangs or unknown expressions, such reports from transcription presented in a paper, for example, can make the reading of these reports tedious or incomprehensible to the readers since the focus is on content and not in speech. Thus, if a respondent has a low level of education and speaks in a wrong way (grammatically), the ideal is to demonstrate these words correctly (formal language/denaturalized language) in transcripts, leaving the text concise and clear to readers.
In this way, it is noticeable that there are relations between the transcription techniques to be adopted (naturalized or denaturalized), the transcription norms and the methods of data analysis (content or discourse analysis), since the last two induce to one transcription technique that must be based on transcription norms. These norms must be strongly present in the naturalized transcription and not so present in the denaturalized transcription. The presence (although minimal) of transcription norms in the denaturalized technique is justified by the reflexivity that is also necessary in this technique, and in some cases, it will be necessary to use some norms to demonstrate where there is the researcher’s interpretation (subjective aspect) in the transcription.
5. From relevance to anonymity or from anonymity to relevance
Although this paper has discussed the role of transcription for qualitative research in management and the relevance of detailing (in research reports) the methodological procedure used for conducting the transcription, it is relevant to reinforce the argument that structures the construction of this paper: the neglect of transcription as a component of scientific rigor in qualitative academic studies in the management field.
That said, and taking advantage of the amorphous structure inherent in the construction of a methodological essay, a simple theoretical analysis is presented below to enhance the central argument of this paper. This analysis consisted of the reading of scientific papers published in three generalist top journals of management with a high impact factor. After selecting the journals, it was accessed the current issue of each of the three (on May 10th, 2019) and all papers that conducted data collection by interviews were selected. Sequentially, it was sought to identify in these papers how the interviews were transcribed and, as expected, the papers generally stated that “the interviews were transcribed”, but did not inform how they were transcribed. Table II compiles the information presented in this paragraph.
Based on the information presented in Table II , it is possible to affirm that the methodological detailing of transcriptions in the qualitative research in management is supported by an anonymous perspective. Thus, it is understood from this that transcription is a given, static and institutionalized fact, and it is not necessary to detail the steps that shape the transcription process nor the choices subjectively adopted by the researcher during this process. This is nothing more than the lack of attention to an important methodological step for qualitative research since it is from the transcription that the data analysis is carried out within the scope of the interviews.
In contrast to the current academic state of methodological neglect of transcription, it is necessary to include the methodological detail adopted by the researchers to conduct the transcription in the research reports, especially in papers. It is believed that this action further strengthens the quality employed by the researchers during the conduction of the research, as well as generates transparency so that readers can discern about the methodological rigor employed during the conduction of the work.
6. In search of the final remarks
Nowadays, it is identified that the method sections are being shortened in research reports, especially in papers, which makes researchers deduct that this essential part should be succinct. However, considering its essence and specificities, qualitative research needs more detailing about the methodological procedures. This ensures more clarity to the reader to understand the course adopted, the motivations that led to the course chosen instead of others and the constraints faced. Therefore, detailing allows greater transparency regarding the reliability of the research results and can be a quality criterion to evaluate the research rigor ( Godoy, 2005 ).
In this way, it is necessary to consider the transcription as one quality criterion in qualitative research, which can be demonstrated by means of the methodological detailing in scientific reports. This quality criterion contributes to enrich the methodological rigor, i.e. quality itself ( Lincoln, 1995 ) and demonstrates the researcher sincerity (self-reflexivity and subjective aspects) in conducting the research ( Tracy, 2010 ). Thus, considering that there are many ways of enhancing validity in qualitative research (Mays, & Pope, 2000), the methodological detailing of transcription as a quality criterion can be one of these ways, which contributes to the quality increase in qualitative research ( Golafshani, 2003 ).
Therefore, how to indicate the adopted transcription procedures in a research report? There is no unique recipe or template to be followed. The methodological description will depend on the authors’ intention to clarify certain aspects that were relevant during the transcription process. Nonetheless, it is suggested that the researcher indicates which technique (between naturalized or denaturalized transcription) was adopted (according to the classification already discussed in this paper) or if a variation between them was adopted using reflexivity.
Based on reflexivity, the researcher can report, for example, that the naturalized technique was used, but that at times it was used a more subjective and reflexive basis to change the spoken language so that it became clear (formal language format) in the transcript, avoiding language confusion for readers. Going further, it is relevant to relate the adopted transcription technique with the method of data analysis used in the research, making it clear to readers that the denaturalized transcription was adopted with the purpose to facilitate the content analysis process, or that the naturalized transcription provides greater robustness for the discourse analysis.
It is also relevant to show the reader the adopted transcription norms and its sources. Thus, if the researcher creates norms, a table illustrating such norms can be created, as shown in Table I . This contributes mainly to the clarity in the reading of the reports coming from the interviews since the reader needs to know the norms to be aware of how to identify and understand them by reading interview quotes in scientific reports.
Such detailing is necessary because researchers need to look at their own choices of transcription, including their own limitations, and it is important to explicit them to readers ( Bucholtz, 2007 ), since there are analytical and/or political biases ( Jaffe, 2000 ) that can induce the process of interpretation between spoken and written language, which can change, consecutively, the result of the research. Thus, detailing methodological procedures of transcription in papers can help the evaluation process in journals, since the transcription as a quality criterion can provide more bases for the reviewers to analyze the methodological rigor (including other methodological procedures of the research) from the evidenced transparency in the text.
This paper also presents a potential contribution to the advancement of qualitative research in the management field, since it stimulates reflection on researchers, especially on those who do not have a deep knowledge of the transcription process. Moreover, by using a simplified language, this methodological study can serve as a guide to undergraduate and graduate management students, because it allows them to learn about transcription procedures and techniques, which will be relevant for their academic maturity on methodology. Hence, students will be able to conduct qualitative research with more reflexivity, precision, and detailing on transcription processes, avoiding (or reducing) possible confusion and misunderstandings in data analysis.
There is a variety of methods for data analysis in qualitative research ( Gonçalves, 2016 ; Miles & Huberman, 1994 ), such as conversation analysis ( Marcuschi, 2007 ), dialectical hermeneutic analysis ( Minayo, 2006 ), narrative analysis ( Ryan & Bernard, 2000 ), content analysis ( Bardin, 2016 ) and discourse analysis ( Orlandi, 2013 ). In this way, the choice for delimiting the unit of analysis of transcriptions only for content analysis and discourse analysis (for being more recognized in management) characterizes a limitation of this paper.
From this limitation and from the understanding that all of the methods of analysis above are based on different philosophical foundations ( Chizzotti, 2010 ) and cultural practices, the following question arises: how do the naturalized and denaturalized transcription techniques, norms of transcription and reflexivity relate to each of these methods of analysis? This questioning is necessary to conduct any research based on interviews, allowing a better adaptation of the transcription technique (naturalized or denaturalized) to be adopted to (the specificities of) each method of analysis and can be investigated in future research.
Taking advantage of the discussion about specificities and the choice of discourse analysis and content analysis to support reflection on transcription techniques, another limitation of this paper is given by the consideration of these methods in a universal way. However, the method of content analysis is composed of a set of analysis techniques ( Campos, 2004 ) that correspond to some variations of the content analysis, which also occurs with the method of discourse analysis. Thus, there are variations of both content analysis (Fonseca, 2009 ) and discourse analysis ( Flick, 2013 ; Gonçalves, 2016 ) that were not considered in this discussion.
Some of these variations or techniques are associative content analysis, statement content analysis, thematic or categorical content analysis ( Bardin, 2016 ), Foucauldian discourse analysis, semiotic discourse analysis and critical discourse analysis ( Chizzotti, 2010 ), among others. Thus, future research may consider the particularities of each variation of content analysis or discourse analysis to better suit the transcription technique (naturalized or denaturalized) to be adopted for each one, from a higher or lower level of reflexivity (which will be determined by the specificities).
Considering the relevance of detailing the methodological procedures adopted for transcriptions conduction, it is noticed that the migration of the current paradigm in which relevance is obscured by anonymity to another possibility is a challenge. Thus, is it possible that relevance surpasses and supplants anonymity about the methodological detailing of transcriptions in qualitative research in management? This is an issue that remains to be thought out and rethought.
Finally, to the readers of this paper, a question is proposed: during your academic journey, how many papers have you read, written or reviewed that explain the methodological details adopted to conduct a transcription? With this, the possibilities are open to sympathizers and even to critics of the arguments presented here to take this discussion to the various academic circles that legitimize and institutionalize the (administrative) science.
Concepts of naturalized transcription and denaturalized transcription
Transcription norms
Occurrence
Description
Signs
Examples
Doubts and assumptions
It is common not to understand parts of speech. In this case, the place is marked with parentheses, having two options: (a) indicate them with the expression “incomprehensible” or (b) write in them what the transcriber think to have heard
( )
Interviewee: There is the (impact). There are in my view three important impacts
Sudden truncations
When an interviewee cuts a unit, it is possible mark the suit with a bar
/
Interviewee: So, we have here sev/85 per cent preservation
Emphasis or strong accent
When a syllable or a word is pronounced with emphasis or accent stronger than usual, the fact is written in uppercase
UPPERCASE
Interviewee: The customer, in turn, when he goes to buy, he asks for ALL of this documentation before closing the deal
Reviews from the Analyst
To comment something that occurs, double parentheses are used at the occurrence moment or just before the segment to which it refers
(( ))
Interviewee: ((hesitates to answer the question)) See … What … it was said very long ago that it was impacting on the region in question
Pause filled, hesitation or attention signals
Basically there are reproductions of sounds whose spelling is much discussed, but some are more or less clear, like: “hm” and several others
Interviewee: Later, it goes to (incomprehensible)… That's the preview, then comes ah … ah… are three licenses
Elaborated by the authors from the compilation of information present in
Journal
Impact factor (JCR)
Issue
No. of papers in the issue
Papers with interviews that were transcribed
In how many papers is detailed how the interviews were transcribed?
6.700
62 (2)
12
2
0
8.080
45(5)
16
2
0
5.329
56 (3)
8
5
0
a 2017 Journal Citation Reports (JCR)
Source: Elaborated by the authors (2019)
Atkinson , J. M. , & Heritage , J. ( 1999 ). Transcript notation – structures of social action: Studies in conversation analysis . Aphasiology , 13 , 243 – 249 . http://dx.doi.org/10.1080/026870399402073
Bardin , L. ( 2016 ). Análise de conteúdo , São Paulo, Brazil : Edições 70 .
Bertero , C. O. , Alcadipani , R. , Cabral , S. , Faria , A. , & Rossoni , L. ( 2013 ). Os desafios da produção de conhecimento em administração no Brasil [The challenges of management knowledge production in Brazil] . Cadernos Ebape.Br , 11 , 181 – 196 .
Bucholtz , M. ( 2000 ). The politics of transcription . Journal of Pragmatics , 32 , 1439 – 1465 . https://doi.org/10.1016/S0378-2166(99)00094-6
Bucholtz , M. ( 2007 ). Variation in transcription . Discourse Studies , 9 , 784 – 808 . https://doi.org/10.1177/1461445607082580
Cameron , D. ( 1995 ). Verbal hygiene , London, United Kingdom : Routledge .
Cameron , D. ( 2001 ). Working with Spoken Discourse , London : Sage .
Campos , C. J. G. ( 2004 ). Método de análise de conteúdo: Ferramenta para a análise de dados qualitativos no campo da saúde [Content analysis: A qualitative data analysis tool in health care] . Revista Brasileira de Enfermagem , 57 , 611 – 614 . http://dx.doi.org/10.1590/S0034-71672004000500019
Caregnato , R. C. A. , & Mutti , R. ( 2006 ). Pesquisa qualitativa: Análise de discurso versus análise de conteúdo [Qualitative research: Discourse analysis versus content analysis] . Texto and Contexto – Enfermagem , 15 , 679 – 684 .
Cavalcanti , M. F. R. ( 2017 ). Guidelines for qualitative research in organization studies: Controversy and possibilities . Administração: Ensino e Pesquisa (RAEP) , 18 , 457 – 488 . https://doi.org/10.13058/raep.2017.v18n3.522
Chizzotti , A. ( 2006 ). Pesquisa em ciências humanas e sociais [Research in humanities and social sciences] , 8th ed. , São Paulo, Brazil : Cortez .
Chizzotti , A. ( 2010 ). Pesquisa qualitativa em ciências humanas e sociais [Qualitative research in humanities and social sciences] , 3rd ed ., Petrópolis, Brazil : Vozes .
Creswell , J. W. ( 2010 ). Projeto de pesquisa: métodos qualitativo, quantitativo e misto [Research design: Qualitative, quantitative, and mixed methods approaches] ( 3rd ed ). Trad. Magda Lopes, Rev. téc. Dirceu da Silva . Porto Alegre, Brazil : Artmed .
Davidson , C. ( 2009 ). Transcription: Imperatives for qualitative research . International Journal of Qualitative Methods , 8 , 1 – 52 . https://doi.org/10.1177/160940690900800206
Davidson , C. ( 2018 ). Reflection/commentary on a past article: “Transcription: Imperatives for qualitative research ”. International Journal of Qualitative Methods , 17 , 1 – 3 . https://doi.org/10.1177/1609406918788222
Duarte , R. ( 2004 ). Entrevistas em pesquisas qualitativas [Interviews in qualitative research] . Educar em Revista , 213 – 225 . http://dx.doi.org/10.1590/0104-4060.357
Duranti , A. ( 2006 ). Transcripts, like shadows on a wall . Mind, Culture, and Activity , 13 , 301 – 310 . https://doi.org/10.1207/s15327884mca1304_3
Farías , L. , & Montero , M. ( 2005 ). De la transcripción y otros aspectos artesanales de la investigación cualitativa . International Journal of Qualitative Methods , 4 , 53 – 68 . https://doi.org/10.1177/160940690500400104
Flick , U. ( 2013 ). Introdução à metodologia de pesquisa: Um guia Para iniciantes [Introducing research methodology: A beginner’s guide to doing a research project]. Trad. Magda lopes, rev. Téc. Dirceu da silva , Porto Alegre, Brazil : Penso .
Fonseca , W. C. Jr , ( 2009 ). Análise de conteúdo [Content analysis] . In J. Duarte , & A. Barros , (Eds.), Métodos e técnicas de pesquisa em comunicação [Communication research methods and techniques] ( 2nd ed. , pp. 280 – 303 ). São Paulo, Brazil : Atlas .
Gerhardt , T. E. , Ramos , I. C. A. , Riquinho , D. L. , & Santos , D. L. ( 2009 ). Estrutura do projeto de pesquisa [Research project structure] . In T. E. Gerhardt , & D. T. Silveira , (Eds.), Métodos de pesquisa [Research Methods] (pp. 65 – 88 ). Unid. 4 Coordenado pela Universidade Aberta do Brasil – UAB/UFRGS e pelo Curso de Graduação Tecnológica – Planejamento e Gestão para o Desenvolvimento Rural da SEAD/UFRGS . Porto Alegre, Brazil : UFRGS .
Gerhardt , T. E. , & Silveira , D. T. ( 2009 ). Introdução [Introduction] . In T. E. Gerhardt , & D. T. Silveira , (Eds.), Métodos de pesquisa [Research methods] , Coordenado pela Universidade Aberta do Brasil – UAB/UFRGS e pelo Curso de Graduação Tecnológica – Planejamento e Gestão para o Desenvolvimento Rural da SEAD/UFRGS . Porto Alegre, Brazil : UFRGS , 9 .
Gil , A. C. ( 2007 ). Como elaborar projetos de pesquisa [How to design research projects] , 4th ed. , São Paulo, Brazil : Atlas .
Gioia , D. A. , Corley , K. G. , & Hamilton , A. L. ( 2012 ). Seeking qualitative rigor in inductive research: Notes on the Gioia methodology . Organizational Research Methods , 16 , 15 – 31 . https://doi.org/10.1177/1094428112452151
Godoy , A. S. ( 2005 ). Refletindo sobre critérios de qualidade da pesquisa qualitativa [Reflecting on qualitative research quality criteria] . Gestão.org , 3 , 80 – 89 .
Golafshani , N. ( 2003 ). Understanding reliability and validity in qualitative research . The Qualitative Report , 8 , 597 – 606 . https://nsuworks.nova.edu/tqr/vol8/iss4/6
Gonçalves , A. T. P. ( 2016 ). Análise de conteúdo, análise do discurso e análise de conversação: Estudo preliminar sobre diferenças conceituais e Teórico-Metodológicas [Content analysis, discourse analysis, and conversation analysis: Preliminary study on conceptual and theoretical methodological differences] . Administração: Ensino e Pesquisa (RAEP) , 17 , 275 – 300 . https://doi.org/10.13058/raep.2016.v17n2.323
Green , J. , Franquiz , M. , & Dixon , C. ( 1997 ). The myth of the objective transcript: Transcribing as a situated act . TESOL Quarterly , 31 , 172 – 176 . https://doi.org/10.2307/3587984
Jaffe , A. ( 2000 ). Introduction: Non‐standard orthography and non‐standard speech . Journal of Sociolinguistics , 4 , 497 – 513 . https://doi.org/10.1111/1467-9481.00127
Jaffe , A. , & Walton , S. ( 2000 ). The voices people read: Orthography and the representation of nonstandard speech . Journal of Sociolinguistics , 4 , 561 – 587 . https://doi.org/10.1111/1467-9481.00130
Kvale , S. , & Brinkmann , S. ( 2009 ). Interviews: Learning the craft of qualitative research interviewing ( 2nd ed. ). London, United Kingdom : Sage .
Lincoln , Y. S. ( 1995 ). Emerging criteria for quality in qualitative and interpretive research . Qualitative Inquiry , 1 , 275 – 283 . https://doi.org/10.1177/107780049500100301
Lukosevicius , A. P. , Guimarães , J. C. , & Zouain , D. M. ( 2019 ). Aceitar ou rejeitar? Eis a questão dos tipos de argumentos para a justificativa de artigos em administração [To accept or reject? The issue of the types of arguments for justifying papers in administration] . Administração: Ensino e Pesquisa (RAEP) , 20 , 1 – 23 . https://doi.org/10.13058/raep.2019.v20n1.1222
Marcuschi , L. A. ( 2007 ). Análise da conversação [Conversation analysis] ( 6th ed. ). São Paulo, Brazil : Ática .
Mattos , P. L. C. L. ( 2011 ). Os resultados desta pesquisa (qualitativa) não podem ser generalizados”: pondo os pingos nos is de tal ressalva [The results of this (qualitative) research cannot be generalized: dotting the i’s on this caveat] . Cadernos Ebape.Br , 9 , 450 – 468 . http://dx.doi.org/10.1590/S1679-39512011000600002
Mays , N. , & Pope , C. ( 2000 ). Assessing quality in qualitative research . BMJ , 320 , 50 – 52 . https://doi.org/10.1136/bmj.320.7226.50
Meneghetti , F. K. ( 2011 ). O que é um ensaio-teórico? [What is a theoretical essay?] . Revista de Administração Contemporânea , 15 , 320 – 332 . https://doi.org/10.1590/S1415-65552011000200010
Miles , M. B. , & Huberman , A. M. ( 1994 ). Qualitative data analysis: An expanded sourcebook ( 2nd ed. ). London, United Kingdom : Sage Publications .
Minayo , M. C. S. ( 2001 ). Pesquisa social: Teoria, método e criatividade [Social research: theory, method and creativity] , Rio de Janeiro, Brazil : Vozes .
Minayo , M. C. S. ( 2006 ). O desafio do conhecimento: Pesquisa qualitativa em saúde [The challenge of knowledge: qualitative research in health] ( 9th ed. ), São Paulo, Brazil : Hucitec .
Mitchell , K. M. , & Clark , A. M. ( 2018 ). Five steps to writing more engaging qualitative research . International Journal of Qualitative Methods , 17 , 1 – 3 . https://doi.org/10.1177/1609406918757613
Mondada , L. ( 1997 ). A entrevista como acontecimento interacional: Abordagem lingüística e conversacional [The interview as an interactional event: Linguistic and conversational approach] . Rua , 3 , 59 – 86 . https://doi.org/10.20396/rua.v3i1.8640619
Ochs , E. ( 1979 ). Transcription as theory . In E. Ochs , & B. B. Schiefflin , (Eds.). Developmental pragmatics ( Chap. 3 , pp. 43 – 72 ). New York, NY : Academic . Retrieved from http://www.sscnet.ucla.edu/anthro/faculty/ochs/articles/ochs1979.pdf
Oliver , D. G. , Serovich , J. M. , & Mason , T. L. ( 2005 ). Constraints and opportunities with interview transcription: Towards reflection in qualitative research . Social Forces , 84 , 1273 – 1289 . https://doi.org/10.1353/sof.2006.0023
Ong , W. J. ( 1982 ). Orality and literacy: The technologizing of the word , London, United Kingdom : Methuen .
Orlandi , E. P. ( 2013 ). Análise de discurso: Princípios & procedimentos [Discourse analysis: Principles & Procedures] ( 11th ed. ). Campinas, Brazil : Pontes .
O’Connell , D. C. , & Kowal , S. ( 1994 ). Some current transcription systems for spoken discourse: A critical analysis . Pragmatics , 4 , 81 – 107 . https://doi.org/10.1075/prag.4.1.04con
Pelzang , R. , & Hutchinson , A. M. ( 2018 ). Establishing cultural integrity in qualitative research: Reflections from a cross-cultural study . International Journal of Qualitative Methods , 17 , 1 – 9 . https://doi.org/10.1177/1609406917749702
Putnam , L. L. , & Fairhurst , G. T. ( 2001 ). Discourse analysis in organizations . In F. M. Jablin , & L. L. Putnam , (Eds.), The new handbook of organizational communication (pp. 78 – 136 ). Thousand Oaks, CA : Sage . https://dx.doi.org/10.4135/9781412986243.n3
Ryan , G. W. , & Bernard , H. R. ( 2000 ). Data management and analysis methods . In N. K. Denzin , & Y. S. Lincoln , (Eds.), The handbook of qualitative research ( 2nd ed. , pp. 769 – 802 ). London, United Kingdom : Sage Publications .
Santos , C. C. C. ( 2012 ). Linguagem como prática social e mediadora da formação cultural e humana: Algumas reflexões [Language as a social practice and mediator of cultural and human formation: Some reflections] . Rios Eletrônica , 6 , 41 – 48 . Retrieved from: https://www.fasete.edu.br/revistarios/internas/conteudo/resumo.php?id=97
Schegloff , E. A. ( 1997 ). Whose text? Whose context? Discourse and Society , 8 , 165 – 187 . https://doi.org/10.1177/0957926597008002002
Soares , S. V. , Picolli , I. R. A. , & Casagrande , J. L. ( 2018 ). Pesquisa bibliográfica, pesquisa bibliométrica, artigo de revisão e ensaio teórico em administração e contabilidade [Bibliographic research, bibliometric research, review article and theoretical essay in administration and accounting] . Administração: Ensino e Pesquisa (RAEP) , 19 , 308 – 339 . https://doi.org/10.13058/raep.2018.v19n2.970
Tracy , S. J. ( 2010 ). Qualitative quality: Eight “Big-Tent” criteria for excellent qualitative research . Qualitative Inquiry , 16 , 837 – 851 . https://doi.org/10.1177/1077800410383121
Vergara , S. C. ( 2012 ). Métodos de pesquisa em administração [Research methods in administration] , 5th ed. , São Paulo, Brazil : Atlas .
Acknowledgements
Leandro da Silva Nascimento lead on the conceptualization, data curation, supervision and validation. Fernanda Kalil Steinbruch contributed equally to all other aspects of the paper.
Corresponding author
Related articles, all feedback is valuable.
Please share your general feedback
Report an issue or find answers to frequently asked questions
Contact Customer Support
An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
Publications
Account settings
My Bibliography
Collections
Citation manager
Save citation to file
Email citation, add to collections.
Create a new collection
Add to an existing collection
Add to My Bibliography
Your saved search, create a file for external citation management software, your rss feed.
Search in PubMed
Search in NLM Catalog
Add to Search
A method of analysing interview transcripts in qualitative research
PMID: 1775125
DOI: 10.1016/0260-6917(91)90009-y
A method of analysing qualitative interview data is outlined as a stage-by-stage process. Some of the problems associated with the method are identified. The researcher in the field of qualitative work is urged to be systematic and open to the difficulties of the task of understanding other people's perceptions.
Life history: a qualitative method of research. Hagemaster JN. Hagemaster JN. J Adv Nurs. 1992 Sep;17(9):1122-8. doi: 10.1111/j.1365-2648.1992.tb02047.x. J Adv Nurs. 1992. PMID: 1401553
[Use of participating observation and semi-structured interviews in nursing research]. Lima MA, de Almeida MC, Lima CC. Lima MA, et al. Rev Gaucha Enferm. 1999 Jan;20(1 Suppl):130-42. Rev Gaucha Enferm. 1999. PMID: 10948952 Review. Portuguese.
The use of interviews in Q methodology: card content analysis. Gallagher K, Porock D. Gallagher K, et al. Nurs Res. 2010 Jul-Aug;59(4):295-300. doi: 10.1097/NNR.0b013e3181e4ffff. Nurs Res. 2010. PMID: 20585225 Review.
Use of constant comparative analysis in qualitative research. Hewitt-Taylor J. Hewitt-Taylor J. Nurs Stand. 2001 Jul 4-10;15(42):39-42. doi: 10.7748/ns2001.07.15.42.39.c3052. Nurs Stand. 2001. PMID: 12212430 Review.
Factors shaping network emergence: A cross-country comparison of quality of care networks in Bangladesh, Ethiopia, Malawi, and Uganda. Shawar YR, Djellouli N, Akter K, Payne W, Kinney M, Mwaba K, Seruwagi G, English M, Marchant T; QCN Evaluation Group; Shiffman J, Colbourn T. Shawar YR, et al. PLOS Glob Public Health. 2024 Jul 23;4(7):e0001839. doi: 10.1371/journal.pgph.0001839. eCollection 2024. PLOS Glob Public Health. 2024. PMID: 39042649 Free PMC article.
Identifying primary care clinicians' preferences for, barriers to, and facilitators of information-seeking in clinical practice in Singapore: a qualitative study. Lee MM, Tang WE, Smith HE, Tudor Car L. Lee MM, et al. BMC Prim Care. 2024 May 18;25(1):172. doi: 10.1186/s12875-024-02429-x. BMC Prim Care. 2024. PMID: 38762445 Free PMC article.
Environmental factors that impact the eating behavior of home-living older adults. Kvalsvik F, Øgaard T, Jensen Ø. Kvalsvik F, et al. Int J Nurs Stud Adv. 2021 Oct 12;3:100046. doi: 10.1016/j.ijnsa.2021.100046. eCollection 2021 Nov. Int J Nurs Stud Adv. 2021. PMID: 38746717 Free PMC article.
Assessing the safety of physical rehabilitation in critically ill patients: a Delphi study. Woodbridge HR, McCarthy CJ, Jones M, Willis M, Antcliffe DB, Alexander CM, Gordon AC. Woodbridge HR, et al. Crit Care. 2024 Apr 30;28(1):144. doi: 10.1186/s13054-024-04919-x. Crit Care. 2024. PMID: 38689372 Free PMC article.
The Role of Social Media in the Experiences of COVID-19 Among Long-Hauler Women: Qualitative Study. Garrett C, Aghaei A, Aggarwal A, Qiao S. Garrett C, et al. JMIR Hum Factors. 2024 Apr 23;11:e50443. doi: 10.2196/50443. JMIR Hum Factors. 2024. PMID: 38652515 Free PMC article.
Search in MeSH
Related information
Cited in Books
Citation Manager
NCBI Literature Resources
MeSH PMC Bookshelf Disclaimer
The PubMed wordmark and PubMed logo are registered trademarks of the U.S. Department of Health and Human Services (HHS). Unauthorized use of these marks is strictly prohibited.
Extract insights from customer & stakeholder interviews. At Scale.
Analysing interview transcripts in qualitative research: how to.
Home » Analysing interview transcripts in qualitative research: How to
Thematic analysis serves as a vital tool in qualitative research, guiding researchers through complex interview transcripts to uncover underlying patterns and themes. By systematically organizing and interpreting qualitative data, thematic analysis enables researchers to identify significant narratives and insights that may otherwise remain hidden. This approach empowers researchers to transform raw data into meaningful findings, enriching their understanding of participants' perspectives and experiences.
While engaging with interview transcripts, thematic analysis encourages a reflective process of coding and categorization. Researchers actively seek to understand the connections between the data, delineating central themes that emerge. This method not only enhances data comprehension but also allows for a comprehensive exploration of participant viewpoints, ultimately leading to deeper insights and enriched qualitative analysis.
Understanding Thematic Analysis for Interview Transcripts
Thematic analysis is a valuable method for analyzing qualitative data, particularly interview transcripts. This process involves identifying, analyzing, and reporting patterns, or themes, within the data. By systematically categorizing the insights obtained from interviews, researchers can gain a deeper understanding of participants’ perspectives and experiences. This method allows for flexibility, enabling researchers to interpret and present the data meaningfully, which enhances the overall research narrative.
To effectively conduct thematic analysis, follow these steps:
Familiarization : Begin by reading through the transcripts, immersing yourself in the data to understand the content deeply.
Generating Initial Codes : Create initial codes by highlighting significant statements or phrases that relate to your research questions.
Searching for Themes : Group related codes into potential themes that reflect broader patterns within the data.
Reviewing Themes : Evaluate the themes against the dataset, ensuring they accurately represent the participants' views.
Defining and Naming Themes : Clearly articulate what each theme captures, ensuring clarity and relevance to your research objectives.
By embracing thematic analysis, researchers can translate raw data into insightful narratives that drive meaningful conclusions.
Key Steps in Thematic Analysis
Thematic analysis is a systematic approach to identifying patterns within qualitative data, particularly useful in analyzing interview transcripts. The process begins with familiarization, where researchers immerse themselves in the data to understand the context and content better. This step lays the groundwork for subsequent analyses, allowing for a deeper connection to the participants' perspectives and experiences.
After immersing in the data, the next step is coding. Here, specific themes or patterns emerge as researchers highlight important segments of the transcripts. This coding process captures the essence of participants' replies, providing a structured way to dissect the complexity of the information. Following this, themes are reviewed and refined to ensure they accurately represent the underlying narratives. By utilizing these key steps, researchers can deliver rich, meaningful insights that enhance the understanding of the studied phenomena.
Coding and Clustering Themes
Effective thematic analysis begins with coding, where researchers systematically categorize data into meaningful segments. This process involves identifying keywords, phrases, or patterns in the interview transcripts that reflect the participants' experiences and insights. Once these elements are coded, the next step is clustering them into themes. This clustering helps in organizing your findings, revealing overarching concepts that provide a deeper understanding of the data.
To successfully code and cluster themes, consider the following key steps:
Familiarization : Begin by reading through the interview transcripts multiple times to get a sense of the content and context.
Initial Coding : Generate initial codes by highlighting significant quotes or ideas that resonate with your research questions.
Theme Identification : Look for connections among the codes to group similar ideas together, developing broader themes.
Reviewing Themes : Refine your themes, ensuring they accurately capture the essence of the data.
Defining Themes : Clearly define and name each theme to reflect its significance within the context of your study.
These structured steps facilitate a comprehensive understanding of the qualitative data and enable researchers to present their findings effectively.
Applying Thematic Analysis to Actual Data
Thematic analysis is a powerful method for extracting meaningful patterns from qualitative data, especially interview transcripts. As you begin to apply thematic analysis, it’s crucial to immerse yourself in the data. Start by familiarizing yourself with the transcripts, reading through them multiple times to grasp the overall context and identify initial themes.
Next, organize your findings. Begin coding relevant passages that reflect important ideas or concepts. These codes will serve as the foundation for finding broader themes. Once codes are established, step back to analyze how they relate and form overarching themes that capture the essence of the data. This iterative process can help uncover insights that are not immediately obvious but are central to understanding participant experiences and perspectives. By applying structured thematic analysis, you can convert raw interview data into actionable insights, enriching your qualitative research.
Techniques for Effective Data Interpretation
One fundamental technique for effective data interpretation in qualitative research is conducting thematic analysis. This method involves identifying and analyzing patterns or themes within the data gathered from interviews. By closely examining the transcripts, researchers can uncover common ideas and sentiments expressed by participants, which help in forming a coherent narrative.
To implement thematic analysis effectively, follow these key steps. First, familiarize yourself with the data by reading the transcripts thoroughly. This step helps you grasp the overall context and tone of the interviews. Next, generate initial codes that highlight significant features of the data, capturing pertinent details relevant to your research questions. After coding, categorize these codes into broader themes, ensuring that they accurately reflect the participants' perspectives. Finally, review and refine these themes to ensure they provide meaningful insights into your research topic, enabling you to draw well-founded conclusions and recommendations.
Software Tools to Facilitate Thematic Analysis
Navigating thematic analysis can be significantly streamlined with the right software tools at your disposal. Certain applications specialize in aiding researchers by organizing, coding, and analyzing interview transcripts. These tools often allow users to import textual data, making it easier to identify recurring themes and patterns from qualitative insights.
When considering which software to use, there are several factors to keep in mind. First, user-friendliness can impact the overall research efficiency; intuitive interfaces help speed up the analysis process. Secondly, features such as coding options enable researchers to categorize data effectively. Lastly, the ability to visualize findings graphically can enhance the understanding of the data, making thematic analysis more impactful. Utilizing these tools can drive a deeper understanding of qualitative data and improve the overall research quality.
Conclusion: Mastering Thematic Analysis for Insightful Findings
Mastering thematic analysis is crucial for deriving meaningful insights from qualitative research. This process entails identifying patterns and themes within your interview transcripts, allowing you to gain a deeper understanding of participants' perspectives. By systematically coding the data and extracting key themes, researchers can reveal the underlying narratives that shape participants' experiences.
As you refine your skills in thematic analysis, remember that the quality of insights hinges on thoroughness and attention to detail. A well-executed analysis helps to illuminate trends and divergences, fostering a richer comprehension of your data. Ultimately, embracing this analytic approach will empower you to produce findings that resonate with both your research objectives and the participants' voices.
Turn interviews into actionable insights
On this Page
How to Develop a Research Hypothesis Effectively
You may also like, ai ml use cases for business innovation.
Top Companies Using AI in 2024
Ai computer program solutions for businesses.
Unlock Insights from Interviews 10x faster
Request demo
Get started for free
The Coding Manual for Qualitative Researchers
Student resources, three sample interview transcripts.
The following three transcripts have been provided to help you test your coding skills. Please note these will open in a new window.
Interview Transcript: Digestive Disorders – Brenda
Interview transcript – a teacher’s observations of child oppression, interview transcript: digestive disorders – sam.
The following interview with Brenda [pseudonym] was conducted in April 2013 by Cody Goulder, a graduate student researching people with digestive disorders. Brenda is 25 years old and the transcription is as verbatim as possible.
As a coding and analysis exercise, review the transcript several times to become acquainted with the contents. Make jottings about passages that strike you and pre-code your initial work. Then separate the extended interview transcript into stanzas. Determine the most appropriate coding method(s) for the transcript to help examine the general research questions:
What are the experiences of people with digestive disorders?
How do people with digestive disorders cope with them?
Also consider comparing or combining the analysis of this transcript with Sam, the other case interview on digestive disorders.
B: Bowel disorders, it is what it is.
I: How old were you when you first started to realize you were having problems with your digestion?
B: I was, uh, 21 and a half, to be exact, yeah.
I: And do you suffer from celiac or, how would you define your discomfort?
B: My colonoscopy says no celiac and not inflammatory bowel disease. My blood marker test says I have inflammatory bowel disease. I would label myself definitely gluten intolerant.
I: And for the record, can you describe what that means? Gluten intolerance? As you would describe it.
B: Gluten intolerance means that you, your body just does not digest or break down or really absorb gluten. And that is a protein that is found in wheat. I would also say that I don’t handle processed wheat well either. Um, and the symptoms are across the board. For me personally, um, I get, I’ll get joint pains, exhaustion, um, and I just feel incredibly full. After four or five bites, if I’m having, say, pasta or something where it’s just, after four or five bites, I can’t eat anymore, feel nauseous. That’s actually where the symptoms really first started.
I: Was there anything else beyond that? Say migraine headaches or …
B: Headaches. I have, and it’s gotten a lot better, I had, um, pretty bad hormonal acne, is what they would call it. Went across the board trying to treat it. I tried creams and antibiotics, retin-As, all that stuff. When I started to cut out gluten and wheats, my skin cleared up the best it’s ever been. I even went on Accutane and, I was on Accutane for five months and that is exactly when my symptoms would appear. I’ve been completely healthy my entire life.
I: Do you think there is a connection between …
B: Yes. I, well, studies have shown that if you possibly have Crohn’s disease or ulcerative colitis and you go on Accutane, there is research coming out that, it can set those diseases off. Um, and I just, I can’t, I think that’s what happened to me because of, like I said, I was completely healthy and then one day I’m having bowel issues and medications.
I: You said you’ve seen doctors, medical doctors, what was that process like of getting tested? What was the response?
B: Well, I went to, when I first got sick, I went to my internal medicine doctor and he’s like, “I don’t know if it’s acid reflux or what, so I’m gonna do a blood test on you.” And he did a blood panel, that’s when he said, “OK, according to these markers you have IBD, go to a gastrologist.” And, I went to one that was recommended, um, and she was just like, “OK, I wanna scope you.” I told her about all these symptoms and when I told her I’d been on Accutane, she kind of made a look like, “Oh, OK.” And then I have a family history, unfortunately, with inflammatory bowel disease. Both of my younger sisters have ulcerative colitis. I have an uncle who is deceased who had ulcerative colitis, and two or three second cousins that have ulcerative colitis and Crohn’s.
I: Can you describe what ulcerative colitis is, as you would describe it?
B: Um, it’s just your intestines not really absorbing the proper nutrients and inflammation, um, and that can be where, um, in any part of your gut. All the way to, Crohn’s can even burn your esophagus and mouth, all the way down through the rest of your body. It’s pretty intense. I was the healthy one. I didn’t have asthma or, not like my little sisters. The hell they went through in middle school with getting sick, I never had that.
I: Would you be willing to talk a little more about that?
B: So, my first sister got sick right around middle school. Her symptoms were, any time she’d eat, she immediately would have to go to the bathroom, instant diarrhea. She’d break out in a sweat. She’d get [ unable to transcribe ], which is a kind of skin lesion, which is, we talked to the dermatologist and, but until you treat really the underlying problem, you don’t know what’s going on. Um, what else did she have? And just going from doctor to doctor. Um, they did a scope and there was a little inflammation that they did find. Um, but they still were very hesitant of saying, “Yes, you have ulcerative colitis” because she wasn’t on, your typical textbook case. I found that really hard for doctors. If it’s not black and white, they …
I: We’ve discussed in other interviews, before this, the fear of using labels in …
B: They’re terrified. I mean, I went through several doctors and then finally, um, I think kinda, and going through puberty, I and, while my sisters were going through puberty, it was really hard. With all the hormones and changing, It just kinda, I think, throws a lot of things off. And then my sister, she’s what would you call remission, but it’s never really going away. You’ll always still have it, but she been in remission for a while now. Um, found the right doctor and he didn’t label her until he started treating her.
I: So it was sort of a trial by fire?
B: Yeah, we’d kind of tell them, “Hey, can we try this? It’s not getting better.” And then my youngest sister, right around the same time, about sixth grade, she got sick as well. Different symptoms. Um, she didn’t have, she had ulcerative colitis. But, there can come blood when you go to the bathroom. And she went in, was severely sick, she went to the hospital. And filled up the little cup they have, completely, with blood. And when they went in to scope, they couldn’t find anything. But she had the blood. She had the joint ache. She has the rash. She’s trying to eat as much as she could, but her belly would distend. And they wanted to send my sister to the psych unit. They thought it was a mental thing and we’re like, “No, she’s filling up the cup.” Like, really? And it was just their reaction because they couldn’t figure out why because the gold standard in diagnosing these things is the colonoscopy. But it’s so hard with these diseases to find it.
I: Why do you think there seems to be a reluctance or a unwillingness in wanting to just get right to the point?
B: I’m not really sure. I don’t, I don’t know. I don’t know if they’re taught that in med school that, you know, that it’s not black and white. And we have found also that, when you are in a hospital setting, you don’t see the same doctor. You have a doctor for a week and then, you know, in all honesty, they weren’t all on the same page. They had their own egos and their own agendas. My sister was in there 21 days. Still, we were finally like, “This is enough. It’s not a psych problem, discharge her now.” And she was still bleeding, two weeks later, she was anemic. We ended up, by chance, being able to get into a different doctor at a different practice who would treat her as if. She was in remission for about three years, she’s out of it now, but she’s got good doctors. She’s still trying to figure out how to beat this beast.
I: Are both your sisters, and you as well, on prescription medication?
B: Um, yes. My little sister Tammy now, I think because she’s been in remission is on like a, something for acid reflux. My younger sister, she’s not on any medication. And my one sister, yes, but I don’t remember what she’s on.
I: And, none of these symptoms have been shown in your parents?
B: My mom, yeah. I remember growing up and her having bowel issues, yeah. And, it’s all on my mom’s side. My dad’s side doesn’t have any bowel issues. This gluten intolerance thing, I didn’t really understand it until I was taking a class with a friend and I was just telling her, “God, I really don’t like.” They labeled me as having GERD and put me on severe, pretty intense medication. I just don’t like the fact I have to take this medication.
I: What is GERD?
B: It’s similar to the acid reflux disease. So, a lot of it is by diet. Little things can set it off.
I: Before all this, what was your favorite food?
B: I loved pizza and burgers.
I: Would you say you ate a pretty balanced diet? Not loading up on pasta …
B: No, but it’s funny ‘cause when I was sick, that’s all I wanted, you know? That sounded really good to eat bread and crackers.
I: Is that because it was a comfort basis?
B: No, um, I think people with that, like sugars and complex stuff, especially like all the sugar that’s really not good for you, it’s addicting, you know? The longer you are away from it, it’s easier to stay away. Have a little and it’s like I gotta have more. It’s difficult.
I: When you started to cut out gluten and bad sugars, what was the response?
B: From like a friend?
I: Yeah. Were you a partier?
B: No. I was so, no, it was weird. I kinda went through my drinking when I was underage. By the time I turned 21, I really didn’t enjoy it. Actually, last night, I feel it. Like, I didn’t drink that much and I feel like hell the next day. Two beers. But, say if I have food and water with it, it’s still mm-mm. So, when I cheat, I’m like, “You’re gonna pay for it the next day.” But it’s hard. Not wanting to go out with friends and, you know, it gets kinda, after a while, “Oh, I’ll just have salad cause that’s really all I can eat.” I can still eat stuff, but finding restaurants that are accommodating to eating to that.
I: Is there a feeling of being ostracized? Your friends or actually from the restaurant itself?
B: Yeah, it’s complicated. I just tell them now.
I: Do you have a specific experience that jumps out in your mind?
B: Yeah, I’d just gotten, a couple of times when you ask, “Do you have a gluten-free menu?” They’re getting much better at it, but I remember when I first started, like a year and a half ago, it was still kind of like [ rolls eyes ], “Oh, you’re one of those people.” Um, cause some people will cut out gluten because they think it will be great for them. But it really doesn’t hurt them. So, I don’t like to be grouped into that. It’d be cheaper. Probably be easier just to be able to go with the flow.
I: How does that make you feel when you talk to someone who says they’re cutting out gluten for my diet, but they can eat bread if they desperately wanted to?
B: Um, close friends, no. Not at all. I mean, because, well, they’ve seen me not do well. I’m just not very nice either because I don’t feel well. Um, but strangers, yeah, that don’t get it. You know, there’s kind of a judgment and they, “Why are you, are you doing it to lose weight or … ?” No, I’m doing it ’cause I feel miserable. But that’s also something that’s going around like in the media, I know, it’s being hyped up as, “Cut out gluten, it’ll make you lose weight.” I think that anything, if you’re just trying, doing it to lose weight, that won’t stick.
I: How do feel with all the mass market of gluten-free this, gluten-free that?
B: It’s a little overwhelming, to be honest. You really have to look at the food labels. Are they taking out this? I still, and trying to find stuff, um, at the grocery store that I can eat, but it takes forever. I try to, at least, read every label. Grocery experiences are long [ laughs ].
I: Is there a specific thing that you want, but know you can’t have?
B: Yeah, that’s my downfall. I mean, I’ve found some places that are gluten-free. But, you know, I haven’t found, has anyone found a gluten-free pizza that you can make at home, send it my way ’cause [ laughs ] …
I: In addition to reading labels and breakdown what I can and can’t eat in the moment, how has your lifestyle changed to feel comfort?
B: With gluten intolerance, I’ve done some research. But I’ve gotten to the point where I’ve, I’m taking a class with a friend and she’s like, “I have stomach issues. Why don’t you read this book? It’s called Eat Right for Your Blood Type .” I didn’t know my blood type at the time, so I started reading the type-O diet and I was like, “Oh my god.” It describes how, based on if you eat these foods, it’s what you have. It’s so me. I had to kinda look away. Is this really me? And it was. So for me, I follow the hunter-gatherer type, meat, fruits, and vegetables. Um, and so that alone, that book and I’m so grateful for my friend, because that brought a sense of comfort.
I: It sounds like you’ve got a lot of support around you.
I: And, have you been able to pass that along to your sisters? Did they ever talk to you about what it’s like to be in middle school and have, really feel, have these differences?
B: Oh yeah, it was really, really tough. Kids, not so much kids, but I remember the teachers would not, being, not really getting it. And my mom would try so hard to, I mean, “Hey, this is what my daughters have. There are the type of medications, heavy medication at one point that they were on. Heavy steroids that make you, not really there. Um, she’s maybe not paying attention because her pain or she’s trying not to shit her pants.” And, um, yeah they had a really hard time finding kids that understood what they were going through. And, it’s a disease on the inside that doesn’t always manifest on the outside. And I think a lot of diseases are like that. Just being aware.
I: Especially when a lot of the symptoms are connected to other diseases? Are you concerned, have you thought about at all what this could lead to?
B: That’s why I changed my diet because I know the blood markers, so, in some ways that kind of means I’m a ticking time bomb. You know, I could get the flu really, really bad. And that could set off this disease. Um, but I’m doing everything that I can in my power as far as diet that I can to control it. Because that also can set it off. I’ve adapted this new lifestyle. Exercise like three, four times a week. Um, that’s been the hardest one, to really stay committed. I’ve conquered the food part, but not putting in the exercise as well. And doing yoga ’cause I stress easily. And, that’ll feed into it, that stress will lead me into making poor food choices. So, finding the balance is what I’m really focusing on.
I: Do you feel that, when you’ve had a bad day, it’s the emotional connection, or that emotion is tied to reactions? “I feel bad, I need comfort.”
B: That’s something to be aware of, definitely. That’s happened to me.
I: Do you think there’s a danger in people becoming so emotion-oriented?
B: Oh yeah. Um, yeah you gotta find balance you know? And being aware, it’s all kind of connected.
I: Is there a point where you’ve had to battle and fears or overwhelming emotions? And you had to bring yourself back? Trigger or phrases that help keep you in balance?
B: Um, I have to stay in the present. And not, “God, what if this happens?” ’Cause that, you know, will set it off. And that’s where I need to be, in that present and just focus on that. And when I don’t, that’s when it gets me and stresses me out. And in listening to your body is the best thing. You are your best advocate for yourself. Not taking the medical. Being in tune. It’s clear if I’ve had a bad week. I eat foods I shouldn’t have been eating. I feel really lethargic and exhausted. If you don’t want to feel like this, don’t eat it. It’s pretty immediate.
I: Do you feel you’re leaning towards organic?
B: I have found, for me, the hunter-gatherer, animal protein. I’d watch documentaries on how animals are being treated, on what they’re given and what we’re absorbing and the cancer rate and all. So, I tried vegetarian, but that means I upped my soy. A lot of soy, had a lot of grains too, even lentils, which are supposed to be really good. And I felt miserable. And I gained a lot of weight. And, they, “You know, don’t eat meat and you’ll lose weight.” For me, I felt horrible. Like, my skin was breaking out, I gained weight. I think like everyone is honestly a little bit different. It’s unfair to the consumer. I gotta eat animal protein or I’m not a very nice woman. I’m cranky. Watch out! But, on the other side, I’ve got to pay more for grass-fed animal meat that’s not injected with hormones. I think that’s what’s causing the cancer and all these problems. It’s because of what they’re giving to the animals. And the hormones. Of course we’re gonna get sick. Of course. It’s infuriating, it really is. But you pay more, a little bit, for the great meat, you know, versus paying several years down the line severe medical bills. I’m not saying you couldn’t, one day, have cancer. But you’ve done everything in your power to not get it and I just got the short end of the stick, but at least I can be in control of, at least I’m eating this. Holds me accountable.
I: Last question, what’s it been like?
B: I have a really tough stomach. Yeah we, my sisters and I, do talk about it. Definitely check in and, our poor dad. We’re all so females that, sometimes, there’s a point we’re at dinner conversations and we talk about our bowel habits and what was going on. My poor dad. So, yeah, there’s definitely an open communication and you gotta have a sense of humor. You got these issues, you have to have a sense of humor.
I: What would say to someone that provides comfort? It’s OK, this is life?
B: Um, we just, we just joke. “Hey, remember that one time when,” you know? You just have, you just kind of have a sense of humor about it, accepting what it is and try to stay positive is how we try to move forward. And be on top of it. And really choosing to have a say in relation to our digestion and stuff. Being aware. It’s different for everyone. Be in tune with what your symptoms are. You’re your best advocate.
An interview was conducted with “Ms. D,” a female, fifth-grade, veteran elementary school classroom teacher in preparation for an action research project on school bullying. The research team interviewed fourth- and fifth-grade teachers at a lower middle-class suburban school site to learn about forms of oppression they saw and heard most often among their children.
As a coding and analysis exercise, review the transcript excerpt several times to become acquainted with the contents. Make jottings about passages that strike you and pre-code your initial work. Then separate the interview transcript into stanzas. Determine the most appropriate coding method(s) for the transcript to help examine the pre-action research question:
What are the forms of child oppression?
Also compose an analytic memo that brainstorms the types of strategies that might be taken by an action research team to lessen the amount of child oppression in a school setting.
I: How do children in your classroom oppress each other?
MS. D: Well, they call each other names.
I: Like, what kinds of names?
MS. D: Oh, we’ve got a little girl in here, she looks different and she acts different, so they’ll make up some name that they call her. They, um, it’s the same kid, it seems like every year there’s one kid that gets picked on more than somebody else, because they’re different, because they might look different, they might act different. Say, for instance, she will say something or she gets very excited about something, they’ll tell her to “Sit down,” “Be quiet,” “Stop doing this,” they’re like on her case all the time. Then you’ve got another kid in here who, well he loses control of himself, and so he blurts stuff out or yells out, and the kids will turn around and yell back at him. And out on the playground they do tend to sometimes get pushy-shovy kinda stuff. Like with her [ pointing to a desk ] I’ve watched them actually walk by this little girl and purposely bump into her or something like that, but then even though you’re watching them, the kid’ll turn around and say, “Well, I didn’t do that” after you confront him. And it’s not everybody, it’s just a few, and it’s a few that have behavior problems that seek attention, and they don’t know how to get attention any other way besides a negative way.
I: How do the students deal with these conflicts?
MS. D: They come to me right away to tell me, so then I have to deal with it. I’ve told them to do it that way. I don’t want them taking means into their own hands, ’cause if they do then they’re causing more problems than, because they tend to get physical or it’s a taunting kind of thing that will take place all over the place. So if they come to me right away then I can deal with just the two people it involves and that way it doesn’t tend to get blown out of proportion. It stays right there rather than getting other kids involved in the situation.
I: What kinds of oppressions might your students deal with in their home environment?
MS. D: Oh, jeez. There’s some sad cases here. There’s this one boy who seeks attention because his mother is a drunken alcoholic. The mom says he’s her best buddy and works hard to get him what he wants. He’s had to meet with the school counselor. There was another girl who was taken away from a bad family situation in Philadelphia because of physical and verbal abuse, her mother was into witchcraft. She moved to live with some relatives here but the home situation here isn’t safe either, so the police had to be called in. But she seems to be settling in now. Her mom’s moved down here but the girl’s slowly evolving into one of the neighborhood kids. She’s the one they pick on a lot because she is a little different, but she’s had different experiences than a lot of kids, too.
I: What kinds of differences do kids tend to target?
MS. D: With this one student the kids seem to zero in because she did look different, and she …
I: Clothing-wise?
MS. D: No, just physically, she, she just, and she acted kind of strange, she would just rock back and forth in her chair, that this was a thing of the abuse, that kind of thing. And one of the girls said, “Stop it, stop it!” and I would have to go over to her and just put my hands on her, “Don’t do that now,” that kind of thing, and we had to have her meet with the school nurse. And she’s the type of kid who thinks she knows everything, so that was another thing that bugged the kids, that she would, and yet she does know a lot, but they just didn’t like it, that it was her . You know, once they had this idea that something’s wrong with them, or they don’t like them, then when they start to interact with the kids and the kids kind of, they’re not accepting. But most of the other kids in this room have been together for years, so she’s brand new, the other kid with problems is brand new, and so it’s the ones, they’re kind of not fitting in because they weren’t with this group as they moved on through school.
I: Like a newcomer?
MS. D: Uh-huh, I think it is like a newcomer thing. It’s basically the new ones. These two new ones were pretty outgoing and were put down by the others, but another newcomer moved quietly and she was easily accepted because she didn’t stand out. There’s another boy who’s obnoxious and the class gets upset with him. The kids pick up on attitude. Their whole thing is attention: how can I get attention and bring it to myself? Acting goofy or silly is a big thing, and some of the kids’ll say, “Oh, stop acting like that.”
The following interview with Sam [pseudonym] was conducted in April 2013 by Cody Goulder, a graduate student researching people with digestive disorders. Sam is in his early 30s and the transcription is as verbatim as possible.
Also consider comparing or combining the analysis of this transcript with Brenda, the other case interview on digestive disorders.
I: How old were you when you first realized you had something, celiac or, I should clarify: do you have celiac or is it a variation?
S: And I’ll clarify, too.
I: Yeah, absolutely.
S: A few things: I do energy healing and, um, as well as like, um, counseling of people like with diseases of these natures. So, because of that I also go to medical doctors or energy healers and nutritionists or people more off, off the beaten path, acupuncturists, things like that. And because of that, these doctors are hesitant to specifically name anything, because once you put a label on it, you give it power. You give it a consciousness and the more you, the more that consciousness is spread out, spread around like ADHD and all of that first came out. It gives it a negative connotation, so I was never told celiac. I was never told, the only thing I was ever told was, in the early stages was candida and parasites. And candida is a form of a parasite. Um, and other than that, they don’t address it to me and I don’t really ask. I’ve, I’ve asked, slipped up and asked, in the past, um, the doctors just like don’t worry about it. Because then, I’ll start to research it and buy into the symptoms.
I: Why do you think that is? Aside from not wanting to promote, for lack of a better term, hysteria, why do you think doctors are so reluctant to label …
S: Um, I think medical doctors is because of the lawsuits. Per-, perhaps, and the liability. They don’t wanna, um, but, but the alternative doctors I go to, which are, I mean they’re also chiropractors, so they are doctors. Um, [ pause ] for one of the reasons I just mentioned so that my consciousness doesn’t buy into it and I create more of the disease, within my own body, which I, we all kinda tend to do anyway.
I: For the record, and certainly help clarify because, through this project, we’ve talked to other people we’re interviewing and we’ve heard different labels for it. So, can you help explain the variations?
S: If you went through my symptoms, you would say, you would say celiac. You would say there’s a lot of stuff. And I just saw something on Facebook, um, a medical doctor, I don’t know, I was trying to find it for you. I don’t know whose page it was, ’cause I have so many fan pages. It was a medical doctor that said, “What I used to, when I was practicing medicine, my patients would come to me and they had all these symptoms, which is fatigue, chronic fatigue, like all the, um, diarrhea, chronic diarrhea.” I’ve, you know, chronic stomach pains, intestinal pain, and things like that, um. Vision problems like floaters, um, I forgot what else she said in the list, but it’s like, “Oh, that’s all me.” There’s, there’s no name for that. But, she said, “When I finally would ask my patients what their body needs, because they went through all the protocols and all the testing and nothing would ever change. When I finally asked my patients what their body needs, some would say, you know, this medication or whatever.” That’s a small percentage of what this host said. The rest of the people, 98% would say I need to quit my job. I need to go do something that makes me happy. My body needs this. My body needs, you know, and it wasn’t related to anything that, food-wise or medical-wise, it was related to lifestyle choices. And, as a healer myself, that’s what I’ve learned as well and, you know, knowing this I should be able to heal myself and slowly, slowly, gradually I am. But, it’s, it’s easier said than done. Especially when you’re dealing with something that’s so emotionally tied into your, your system and your psyche. Does that make sense?
I: Yeah, it does.
S: And that kinda follows through with what, when I’ve started reading into the candida years ago, I was first diagnosed.
I: Can you explain a little more about candida?
S: Candida is a yeast infection. And, when I first heard that, I’m thinking “Oh, which chick did I get it from?” [ laughs ] And so, I started like, after a while, after about a week, I’m like, you know, I’m gonna google this, and what it is is, we all have this natural yeast that occurs in our bodies. And, what happens over, it could be a traumatic issue. A traumatic occurrence or a thing like that, um, that happens in our lives and that yeast will, will, like, say we have X amount of yeast in our system. Let’s just, naturally good yeast. Quote unquote, good yeast.
I: On par with, say, the good bacteria living in our stomach.
S: Right. Well, when that good yeast expands to like double X or triple X or however, I’m just, I’m not, um, when it expands, that level, then it starts to become bad yeast. And it starts to take over and, it’s not, it’s only bad because it’s too much of it. And that yeast will affect your ability, and then the more sugar you have, the more you feed the yeast. The more gluten you have, the more wheat, the more things that, you know, have gluten in them, the more you’re gonna feed it. Um, and so forth until you get to the point where it’s like, you can, and I’ve read the diets and the diets, you can’t even, it’s almost impossible. They say it’s almost impossible to do. You have to do this diet to, to cut out all the yeast, you can’t even have carrots.
S: ’Cause of the sugar. But, then they say carrots are iffy because carrots also help kill the bacteria. It’s like there’s so much unknown about this, but it’s said it’s all, but the consensus that, I googled of all these websites that talked about candida is, it’s all emotional in origin. Hippocrates said the same thing. He’s the father of, you know, modern Western medicine. He said all disease is emotional in origin. As a healer, I know this. Because, even cancer starts as an emotion. And the more that emotion manifests, you get a tumor or something negative. Um, and I full-heartedly understand how that works. Because, especially in dealing with patients and myself, it’s like as soon as you get rid of that emotional counterpart, the disease goes away. Even if it’s cancer, I’ve seen it happen. They say it’s pretty amazing. Um, so, I’m sorry, what was your question?
I: What was candida?
S: Yeah, so, that’s what candida is in a nutshell. And so, that’s what my doctor started treating me for. My doctor, my healer, doctor, chiropractor started treating me for. And, and she told me to cut out all of, and this was probably about in oh-five [2005], it was about a year after I graduated [from university], getting my master’s. Um, it was, she treated me, she said no sugar, no caffeine, no dairy, I couldn’t do dairy either and no gluten, obviously. And, gradually I slowly weaned myself off, ’cause she was a vegetarian at the time, I slowly started weaning myself off of meat and stuff. I did eggs for protein. And what ended up and, I believe this was still, this was less than a year, about a year after my mom’s death, which was devastating for me, and I think …
I: What did she die of?
S: Oh, I can tell you the whole story. Can I?
I: Absolutely, we’ll circle back.
S. Yeah, um, and I believe that’s what started this manifestation in my stomach and my, my intestines ’cause I can tell the difference now. After a bowel moment I can, I’m just worn out. Um, so it was a year after my mom died and I went off all these things. Did the eggs for protein for about two months. I lost 40 pounds of muscle. And fat, but mostly muscle. So, I went from a size extra large shirts to mediums.
S: It was bad. It wasn’t, and I was also in depression and that’s why I want to preface that because I believe that depression plays a part in this all. Is that, whether we know it or not, you know?
I: There’s different levels of depression, period.
S: Exactly. And, there’s, and then there’s the fears that I constantly face like, within myself, and I think that contributed to it. I notice that when, like this HOA [Home Owners’ Association] thing and I think, I thought it was perfect that it was coming up. I hate the HOA, just like you were saying. And I was, I don’t know why I was having such anxiety over this meeting, ’cause once I had the meeting, it wasn’t a big deal. But like, there are certain people that I thought were going to be there, and that weren’t there, that I was like, I don’t wanna deal with these assholes, right? So, that, and that, and I was paying attention to what was happening, having anxiety this past week and it was going, it was going right to my gut. And, I’m like, well that’s not good for me. What am I doing to myself? But, like I can intellectualize it. But it’s, but until I like either do meditation or just like breathe and just get it through my system or just face it, which is what I did today, I, that’s why I went to the meeting, um, until you face that fear, you can’t, it’s almost impossible to get rid of it. Because once you face your vulnerability, that’s when, that’s when you empower yourself. But, most people are used to running away from their vulnerabilities. Does that make sense?
I: Absolutely.
S: So, OK, you wanted to go back to my mom or, I kinda jump around so keep me …
I: No, it’s fine, I like to jump around. Um, so how does, let’s backtrack a bit to candida, trying to get a scope of these disorders?
S: I can tell you how candida manifested into other things if you …
I: Absolutely. Oh totally. Yes, so how does it differ from, say, someone who has celiac or has a general gluten or lactose or … ?
S: I think people that have celiac I, don’t quote me on this, but I, well, you can quote me on this.
I: I don’t have to use it.
S: I, I’m pretty sure people who have celi-, celiac also have candida issues. I’m pretty sure and, you know, chronic fatigue plays into all of that. I’m pretty sure that people who have gluten intolerances have the celiac, whether they were tested for it or not. I’m not sure that most medical doctors, some of them do ’cause I’ve been to a few that do, will test for celiac. There’s a spit test you can do. There’s all these other tests you can do that are, that don’t cost money. But how does it come, go into play?
I: Is it sort of like …
S: I think it was, for me, I think it was the first stages. Um, at least as far as a diagnosis goes and my doctor slowly started treating me for celiac. Once she got that under control, then we started treating me for, like, if I have gluten I’m bleeding out my, you know, out my ass because, and I didn’t know that’s what celiac did. Because, my friend works, he’s a higher up at [a restaurant] and he works in the kitchen and he’s like, he’s like it’s very serious. In like, really, ’cause he, everyone calls it celiac ’cause it’s more widespread as a diagnosis and that’s what we label it.
S: In all intents and purposes, you could say I have that, but I don’t like to use that label.
I: Is that because you feel that, as a medical term, celiac is an easy way to create an umbrella over these conditions?
S: Absolutely. Its, it’s just like, back when they used to say ADD and ADHD they would come up with all these initials for that. You remember those, when that happened?
S: And I’m just like, that was us growing up. I was an A student, but it was still, we were, my little brother was way even more hyper. My mom didn’t know what to do with that. But she didn’t drug him because she didn’t want to deal with him. She just dealt with it. And now we call it something so we can put someone on drugs. But it doesn’t help them. You know what I’m saying, it’s like toxic to those kid that grew up, and now they’re adults, a functioning, and they’re like, that was the worst thing you can do to a kid is put them on the drugs, because they can’t access, access their creativity.
I: What are your feelings when you see gluten-free diets, everything’s being marketed as gluten-free this, gluten-free menus when you are in a restaurant?
S: I actually, honestly, I appreciate it. I don’t think of it as, as a bad thing. Like, what is it, on Picasso’s Pizza, Pan Gusto’s Pizza, which is one of the old Picasso’s, they’re, almost all organic and all gluten-free. Organic, I think, fits into it. If you’re gluten-free you’ve got to watch the pesticides you’re putting into your body. Um, and diet, we’re learning more slowly as a society that diet is the best, is a better medicine than actual drugs. Um, it’s what you put into your body, not just the preventative, but um, as a way, that when you do have something, as a way to get out, get yourself out of it. Um, and …
I: Because food is something that you need and you cannot operate without it.
S: Right, right. And if you’re eating stuff that is attributing and continuing exacerbating the issues that you have, whether it’s emotional or not, I mean there’s still, there’s something in your system that’s exacerbating the problem, then how, how is it that any amount of medicine or anything else going to help you? But if you eat stuff that promotes the good stuff to occur and helps you, help you feel better, helps you to feel more energetic and have energy to exercise, that alone and just a better outlook can push away most diseases in anyone’s body, whether that’s gluten or anything else.
S: Um, there’s so much more I was gonna say because, like, as I’m talking, I’m having all these thoughts.
I: If it comes up to you, just throw it out there.
S: I can send you some stuff from like, I see this happening on my pages every day. Like Socrates or Plato or like all these people or Doctor Freud.
I: That would be amazing if you were …
S: It’s some amazing stuff that, like these are all on my feeds that I hit “Like” on. But, it talks about like, all this stuff in different ways. And they, it’s just …
I: Are they posted on your Facebook page?
S: No, it’s just my feed.
S: Various feeds. And so, you know, as it comes, I’ll just forward it to you.
I: Absolutely. I’d love to see these.
S: OK. And, some of them I save and some of them I don’t. If I have any on my computer, I’ll just, yeah, because, and I’ll, it’ll help your, I think it’ll help your [research].
I: I think it will help this project a lot. Um, and just having information too, to know more about …
S: I mean, and you could hear me say, as a healer, like, when you hear other people that are famous, it’s almost kinda almost …
I: Well, it’s refreshing, I mean, it’s refreshing to get it from your perspective because, as you described it, a doctor is going to tell me something that I …
S: And I was at a doctor, um. OK, there’s something I wanna say and it’s all coming out at once, I was …
I: Take your time, we’re in no rush.
S: My, my chiropractor sent me to a doctor because she’s like, “I can’t prescribe medication but I really think, to kick this out of your system, we want to prescribe this,” and she told me that, what she wanted. So, she sends me to a person I know and a person that she knows and this doctor was just, she was a medical doctor but a quack. I’m just like, “You don’t know anything.” And, I’m like, she was testing, which is fine, testing me for all these, testing my blood, testing my liver and all this. And, she’s like, “Well, I don’t know what to do.” I’m like, “What about that medication, you know, doctor- she suggested?” “Well, I could put you on that and I think that’s the best thing, but I just don’t know what’s going on with you.” And, I’m like, it’s all like going back to the medieval days for me. It’s like, I’m like, I spent time with my doctor and we’ve been treating this and we want results to just kick it. But, she’s all, doctors have that ego. Like, “I’m God, I know better than anyone.” And it’s like, so I took the drugs. Literally, it happened Friday night until Sunday evening, I was in-, I was incapacitated. I’ve, I’ve never been, I can’t call it sick, I think I was in a coma. I could, the only thing I could do was get up to pee, I couldn’t even get water. It was, and what happened was, what I researched and what my chiropractor kind of already knew, she’s pretty intuitive, is it killed a parasite in my liver and it caused that reaction. Now had I known in ad-, had I actually known this in advance, and in hindsight, there’s a tea you can drink that’ll counter that and I would have been fine. But, you only know this stuff through experience. It’s who’s, and this is funny ’cause my mom was the same way. She would educate the doctors. And all my, all my uncles are doctors. Um, so my mom had, she, she was gluten-free later on in life, um, because of her, she had rheumatoid arthritis. But, mostly she, she got on a healthy diet because of the arthritis. She would educate my uncles in treating their patients. She’s like, they would argue with her, “This, this is not what we were, the medical books say this.” And, finally, like after, I was, I was a little kid going to [city], that’s where my cousins are. And that one year, they just switched. My mom was just so beside herself, “I’ve been saying this until I’m blue in the face, what made you see the light?” They’re like, “Our patients are demanding it from me.” And so I had to study it and learn that food is more important than medicine in a lot of cases. You know, you’ll never get them. They’re my uncles and I love, they, but they’ll never say that out loud. Because that’s just, it’s their careers and the, it’s the insurance companies. And I’m, I’m doing all of this out of pocket because my insurance company won’t pay for what I had. I got rid of my insurance. They wouldn’t pay for it.
I: Why wouldn’t the insurance company cover that?
S: They won’t pay for a chiropractor, they won’t pay for a nutritionist. They’re just something society doesn’t deem as important. Some insurance companies will. I have Blue Cross. And after, after several years of, after paying my, you know, paying my doctors out of pocket, I’m just, why have insurance? You know, and so my dad would get back because he’s an attorney, he was an attorney. And he would just, so he would pay it for me. And when he died, I was, just would, my dad, he cancel. [ slight laugh ] Because he had, but that’s because, how he was raised. They were taught growing up, is, you know, from grandparents and aunts and uncles that grew up in the Depression. You need insurance. You need this. You need that. And, this is how you live. You live in fear of the what-ifs.
I: That’s going to happen, you may need this.
S: And I, and what helped me change that attitude, because that’s how I was raised by these people. My dad, my grandfather, what changed, my mom wasn’t like that. She was the artist. She did a lot of coppers, but she did a lot of painting as well. But, um, that’s what she did later on in life. Artistic career. And then she became a realtor in the 80s. And that’s what she did until she, and then she kind of retired after all that, when they moved to [a new location]. But, um, so that’s what she did. Where was I going? I forgot what I was talking about.
I: We were discussing, where did we, we started with celiac umbrella term, and, last little blurb. Insurance. Why did you need insurance?
S: And so, I guess we were on a, a track. I was just saying that, you know, we train our society to grow up in these fear modes. I feel that the fear that you have like, that creates the fear of the what-ifs creates more of that happening. Like, what if my house flooded or what if there’s a tornado? Well, those are the people that attract that most to them. And I’ve known, just from my own experience that if you were to ask me this 10 years ago.
I: Is there a specific experience that jumps out to you?
S: Of me creating my own situation?
I: Or seeing it in someone else?
S: In my dad, yeah. He would create these fears and they would happen. Just like, if I didn’t have insurance then I’ll, then you look at someone like me who grew up in the same family, and I don’t have insurance, and even my doctor, my chiropractor, she doesn’t need. She’s like, “Sam, if I could live like you, I would. But, I still have that fear of society. And if you can let that go, if something happens, it happens.” But, if not, it’s, I, it’s like ever since I saw the movie, and I don’t, I’m just gonna throw this at you. I saw that movie, this is as I was going to join [a university degree program] and I, I didn’t want to bring up the girlfriend. She was a [student in the degree program]. Um, but she, she and I were going through a, insane shit. I won’t go into it, but if we …
I: I want you to know that this is a safe place, so if you want to go on a tangent, throw something out there, go for it.
S: Yeah, you could write my life story later, but I, this will [ laughs ], her and I were going through a, um, emotional upheaval that we’re told, um, ’cause we didn’t know what to do. I mean like, shit was, shit was flying around the room. It was like that kind of, like a, um, looking back was an emotional thing. It manifested itself in, there’s so much we don’t know. [ laughs ] That’s another conversation.
I: That’s another conversation for another project.
S: A major conversation. Um, it’s a major conversation. Not because it was personal but because um, but that kind of tied into it as far as, um, her and I saw this movie. I think it was separately because we were breaking up at the time.
I: What was the title?
S: It’s a famous movie. You’ll know it when I tell you it. It came, I can’t think of it. Not The Secret , the one before? [ pause ] But, anyway, it’s this movie, before I’ll, I’ll get it to you.
I: We’ll figure it out after …
S: If I IMDBed [Internet Movie Data Base] it, I’d find it. It’s a documentary. And once I saw that documentary, after this documentary, I’m like, this is stuff I knew in high school. But I would never say it because people thought I was, would think I was crazy. These were scientists that came up with all this stuff. Not gluten people, right? Um, and in the second half of the movie, it was just like, it was more story with Marlene [ sic ] Matlin in it. And, you know with, the deaf one. And you see her like taking all the drugs in her medicine cabinet and throwing them out because it was, it was her realizing that power not to need that. And I used to take Advil all the time for headaches or whatever. Especially going through [university], you understand how that is. I’m just like, you know what, I had such a rush of, after watching that movie, I took, I even threw out my Advils, and I’ve never needed them since. And so, that’s kind of, that’s an example of where I don’t need that insurance, I don’t have to go buy it. And, if I ever do have a headache, which is probably like three times in that eight-year, nine-year period, very minor.
I: Let’s tie it back to the food issue, because one of the theories running around out there is because so much of the food we consume is this genetically altered …
S: Monsanto.
I: Monsanto. There’s, corn is completely different, the amount of steroids and things they put into beer and chicken. Even the treatment of animals is a hot topic issue. It’s all over the place. How much of that do you think ties into these fears that we have? What I put into my body?
S: I think a lot of it does. The people who are against Monsanto and the pro-organic, whenever you’re against something you create a fear. So if I’m saying I’m against, um, non-organic food or I’m against GMOs, well then, you create that fear that these things are bad. I’m not saying they’re bad or good because I don’t know. We haven’t done enough tests on Monsanto. But by creating that fear even we, it’ll even get in my head that it’s, well, I’ve got to be careful I don’t buy GMO. Then, the more I create that myself, I limit the foods I can’t eat. You know, at least in my mind. In reality, could I eat Monsanto and probably be fine? Probably. But, if I knew it was and I was eating it, that would exacerbate the food. I mean, that would exacerbate the food I’m putting into my system. And, I’ve noticed within myself, if I’m focusing on negativity, if I’m pissed off at someone or in a situation where I’m pissed off and not eating, it’s just, I’m gonna, I’m gonna have diarrhea that night. It won’t be the next day, it’ll just go right through me because I’m eating with anger. Doesn’t that make sense?
S: I mean, I’m not sure how much you’re into this.
I: No, this is all good, I mean, we’ll cycle back in and through.
S: And these are all things I’ve learned since, it was either taught to me sometimes or either, but mostly, the way I’ve learned is, and I’ve always thought this was odd, especially going through [university], I would have a revelation or an epiphany or I would have the experience, learn that way. And then, maybe like a week, a month, a year later or two years later, I would have the validation. I mean like, why is that happening? But, I realized because the, it comes from a book, it doesn’t have as much power as coming from me having the experience first. And then I’d have the validation later. Because, I think, I’ve grown up very skeptical of all this shit, trust me. Even though my mom was very into health food, you know, tried to instill that into her children, it was still kinda feel like, oh, that’s just mom. That’s how we are with our parents. So, but because of my own experience, I’ve been able to develop my own ways of doing things, whereas if someone tells me something, then I’m just kind of like a puppet. Being pushed around and the, with the food industry, with Monsanto, people saying pros and cons. And as much as I try to stay out of that, you still see it on Facebook. It’s because of the places that I hit “Like” on.
I: Getting back to the experiences, I wanna circle back into your background, um, how old were you when you first …
S: Had stomach stuff?
S: [ pause ] Here’s where it gets interesting. I believe it was, if I could trace back all the symptoms, I believe it was probably like, when I was, um, probably in my 20s, maybe 21, 22. I remember talking to a friend on the phone, going and asking like, “Don’t you just feel like wiped out after you go to the bathroom? You know have a, have a bowel movement?” And he’s like, “No.” ’Cause I used to work out a lot back then and I’m like, and that happens to me now where I’d have a bowel movement and I’d just, I’d just be exhausted. I’d have to take a nap. I mean, literally, take a nap. Um, and, but no one, who’s to know back then? No one talked about any of this stuff so I wasn’t aware that’s what’s going on. So, I would say probably around 21 is when I felt it started. Um, now, going back before that, when I was in college at [a western university], 18, 19, 20, or maybe even in high school, I drank a lot. And I’m talking Jack Daniels in one hand, Bacardi in another and have a couple of beers for chasers. And the reason I elected to be social, it was because, it actually didn’t make me drunk back then. I would be the designated driver and I was drinking that much. Because people were like, “You’re, you’re sober.” After a while, I stopped arguing with them. My blood alcohol content probably didn’t say that, I could function, yeah. So, I just drank because it was the thing to be social. I think, in the physical world as opposed to the emotional world, I believe that is what helped destroy some of the good lining in my stomach, the bacterias. And I believe that’s where it started. Because one, every year in the spring, this time of year, March, April, May, a month, I would have a stomach issue. And that started so, so the symptoms started when I was 21 with being exhausted after the bowel movement. You know, like, 25, I’m back from school living here. 25, 26, I would notice, like every year, for about four or five years I would have these issues of one-month stomach issues. And that’s exactly what I’m currently going through. Um, and then like gradually, I would have like acid reflux, and so I would take whatever people would, and it always exacerbated with alcohol. So finally, and that’s why I don’t drink too much. I can go six months to a year without drinking a drop. You know, it just depends where I’m at. Because, I know it’s going to re-effect it. Just from experience, I try not to put the thought in there and it doesn’t.
I: How’d that change socially? Did you notice a change at all? Was there?
S: Socially, I had to make, I had to make the, I had to make this decision to stop drinking. And when that happens people feel, like you think your friends are just like, “Oh, c’mon,” it’s really like a tug of war. It’s like, why is my drinking affecting you? In me going through that, it made me a stronger person. In that, like, per-, pressure way. And even the gluten stuff is like, some friends of mine I can’t even be gluten-free around. It’s like, I won’t even eat dinner with you. Sorry. ’Cause it’s like, especially if I go over to their house …
I: What is that conversation like?
S: Most of my friends know now, but like initially, certain friends, especially the ones from [a western university] that aren’t sensitive, mostly guy friends: “You’re fucking weird or pussy,” stuff like that. It’s like, it’s kinda like, “Oh, c’mon.” And I’ll even drink water that doesn’t have ice in it. I thought my mom was crazy growing up, doing that. I couldn’t do that. But my doctor even said, “Don’t drink water with ice in it because what it does is, it makes your stomach and your system work that much harder to digest the coldness and make it warm, room temperature again.” So, if you already have digestive issues, and I take …
I: Don’t they say, in certain diets, that if you want to lose weight you should drink cold water? One of those little tricks that they tell you? Same with eating peppers.
S: Peppers actually do help me. Certain peppers with the intestinal lining, which wore away gradually due to, they call it leaky gut syndrome. And like, all the toxins within your stool with, be passing through. You’re supposed to absorb the good stuff and the toxins go out. Well, all the toxins were getting into my blood because the gut lining was so thin it started going through the wall. That’s what they call a leaky gut, which was contributing to the, um, chronic fatigue. Which I, and I don’t like to label it but, for me, it was chronic fatigue. Back to what your question was, I’m sorry.
I: How it affected you socially.
S: Um, so socially I, I don’t, I don’t go to bars and if do it’s tough.
I: What specifically? Is it just the …
S: Because one, I’m not drinking this. But two, because most bar food is fricking fried and it’s got gluten in it. And, even if it’s not fried, it’s not the most healthy, you know? So, my choices are eat beforehand, meet people, sit around and talk while they eat and drink and, you know, you can still have fun. Like, I have friends that are alcoholics who, you can still have fun and, but you can’t, I mean, I just gradually stopped going. Dwindling, so socially, it’s like, to answer your question it’s, I’ll just tell you, I literally, I haven’t lost friends, but I don’t hang out with them as much as I used to. I mean, not nearly as much. I was out every night. Now, it’s sometimes once a month.
I: And that’s not something one can find, almost like a support group or …
S: And, it’s one of the things I was just gonna address which is, it’s almost easier to say, “I’m an alcoholic” than “I’m gluten-free.” It’s all easier to say, “I’m an alcoholic” than say “I can’t drink alcohol because I choose to not drink alcohol with you.” Because when you’re an alcoholic, people like give you that respect. That just is. But when you’re, when you make a choice for your health, to eliminate something out of your diet, it’s like, it really affects other people. And I had to learn that that’s not my issue. Just because you want to drag me into your hell doesn’t mean that, and I had to learn that, how to be strong enough, to stand up for my own health, really. And that’s what it boiled down to. I mean, literally, and one of the guys I’m talking about, kinda referring to is, I see him once every year or six months now. We used to hang out all the time. But because he couldn’t let go of that, and even with his daughter, she, he had a three-year-old who’s had issues with gluten. And I, we were out at dinner and they order it special, non-dairy because no dairy ties in with gluten. As well as alcohol and all that stuff, sugar. Um, and he, he was getting on her, and his family’s practicing medicine too. His dad and uncles are doctors. The words that came out of his mouth were, “I want her to eat normal cheese because I don’t like it.” So, I can live my life and I’m just thinking, and I don’t like, I don’t like to chastise my friends ’cause that’s their choice how they want to raise their family and live. ’Cause, I don’t want to do to him what they’d do to me basically. But when they say that, it’s like you’d rather put your daughter on drugs and medicine that might affect her later on, at three years old, than just get her off gluten for a while? And have her just be healthy? So, I don’t know, it’s for me. And I see her face too, it’s the irony of that. And it’s kinda like that lady, Louise Hay, who I think it was from 73, 75, she made the decision, not because of her health, because of her health, but not because she was gluten intolerant or anything like that. It was a decision before it was even popular to do no sugar, no dairy, no alcohol, and no gluten. I think no caffeine too, like there’s those kind of four or five things that could kind of contribute to the issues. She’s almost 90 right now. I mean, and that’s amazing in our society and she’s got her own publishing company.
I: Especially when it is not with the assistance of a plastic heart. Or something that has been artificially put in.
S: Exactly, so, and there’s probably everyone for her age, there’s probably other people that are smokers and, you know, do drugs all the time. So, who knows? I mean, I’m just saying, yeah right. Anyway. All these things they’ve found for cures have also proven harmful to your system. So, she actually wanted to learn how to be able to get out of bed during the day because of her arthritis. Because of the gluten at the time. The more she looked into the diet, the more she researched, she learned gluten could affect it all. Back then, all it was was rice, bread, and that’s it. It’s better for me to have brown rice than white because of the nutrients. In the food aspect, I’ve gotten to points where I’m like, I don’t want to eat any more. Like, literally, I, my situation is probably different than others. I eat out almost all the time. I will eat like raw foods, which I’ve found is much better on my system besides processed foods.
I: What is your favorite kind of food?
S: I don’t eat pizza anymore, unless it’s from Picasso’s because they do a great non-gluten, non-dairy pizza that tastes great.
I: Were you a big pizza buff before that?
S: I ate a lot of pizza. I knew it wasn’t good for you but I did it. I mean, it’s cheap. I would eat Taco Bell a lot, and there’s things that I would do in college that I would only do in college that I wouldn’t do when I was out. And that was smoke pot. Although, I didn’t really inhale. As soon as I graduated, I was done. If you put something in your system, make sure it’s good. My dad connected that with gourmet. My mom, she said organic. I like seafood. Just have to be careful it doesn’t have a thickened sauce with flour. Afterwards, no pizza. The dairy will affect me as much as the gluten, if not more. Sugar’s been the hardest one. I can cut it out and be cold turkey. But the little increments I can’t do. Sugar also contributes to cancer. And, they’d rather fight cancer with chemo than do it the right way. The candida was the first thing that we addressed with my treatments. And that was over the course of maybe six months to eight months. Maybe longer, I don’t know. This is my memory. But then after that, we started treating me for parasites. Whether it morphed or it’s just, I think she was doing the stages.
I: And this is when you were seeing the doctor?
S: The chiropractor. And this is all out of pocket. I was seeing and what literally brought, OK, I was seeing her and she got me to a place where I was stable. I stopped seeing her for about three years. Um, I came back to her. It was hard for me to come back to her, not because I didn’t like her, but because, um, I had gotten to a point where I, I would wake up in the morning, go to the bathroom, like you know take a shit, and I was exhausted because like, literally, it was my gut was leaking. So like all the toxins were coming out through and it would burn and it, it was like draining. I learned that your stomach is your power center, it’s where you hold most of your power, and if that’s affected, you’re wiped out. That’s from my experience, I found out research that proves it, but I, or otherwise I’m just telling you what someone else said. So, I’d wake up in the morning, take a shit, ah fuck, go back to bed. I’d get up. I’m like, my God, I’ve gotta eat. I, get this, this was going on for weeks. I’d get up, go downstairs, grab something out of the fridge or out of a cupboard, eat some food, that would wear me out. It’s like it’s wipe me the fuck out. And I would go back to bed. Then I would take a shit. Like, this was throughout the whole day. I would stare at the ceiling looking, thinking, really start talking to God, “Why the fuck am I here? If you want me to, like, what do you want me to do?” It’s like, it’s like you have that conversation and it’s like, just kill me or take me, you know, because I don’t know if I can, if I can’t function, then what’s my purpose here? I can write about this, but I can’t when I’m exhausted. So, I got to this point where I’m just like I have to go back to this doctor. Literally, like, she won’t say anything. She doesn’t want to alarm me, and she knows me, ’cause like, we had this understanding. It’s OK, don’t tell me. Um, literally, she had to treat me for parasites. For all this stuff and she would gradually do it, without explaining to me the process. And I never asked. I didn’t care, because it’s like I don’t want this part to interfere with this part of, you know? If that makes sense? The mind and the stomach. Um, so I started seeing her and literally it was like, but I knew I was ready to die. And she’s like, “You, you’ve had this for a long time” and she’s like “We’re past the point of me treating this for you. You just felt good and stopped seeing me.” OK, I get it. I started seeing her again and like stage by stage we’re treating me for allergies. For gluten allergies, for, I actually started getting some arthritis symptoms here and there and they’d go away once she started treating for, um, for arthritis. She treated me for leaky gut. But you can’t do it all at once. Gradually you can, but she wanted to treat one thing at a time, to make sure it was working. And it was, but, you like, she comes from an engineering background before she became a chiropractor. Intuitive. Nutritional. So we stated with candida, then we would treat me for parasites. Then we would treat me for allergies. Food allergies. And then something emotional would happen, and it would be just like, I’d be back at square one. Not square one, but it felt like I was back at square one. And, when that emotional situation would happen, I can’t remember specifically what incidents back then, but something would set it off and I would either get pissed or all my symptoms started coming back. It can be a physical or emotional stress. My triggers are people attacking me with words. It goes right to my gut and I haven’t gotten past that sensitivity, especially when it involves anger. So, I understand the emotional part. Like people aren’t making this stuff up. How can you agree with one part they say and not the other? People are nuts, man. It’s like you have to do what works for you. When you’re living in a hole where everyone wants to tell you what to do, they don’t know your system. The only one who knows it and can empower it is you. I’ve learned to be stronger, to be able to walk with more confidence as opposed to going around life getting pushed around like a pinball machine. No matter what kind of people try to steer me off course. It’s harder to talk to myself because then I have to listen to this shit. It’s easier for me to explain it to people. I get that. More full life. More satisfaction in life. We always want to be better than our parents and have our children better than us. I’m more in tune with what I’m doing. I’d rather not have gluten at all and cheat after a while. When you have too much of the same food, eventually, your body will reject it because you’re not, it’s just the tolerance for it decreases. Just like the antibiotic. I would take antibiotics to get rid of lingering stuff. I didn’t know there were natural cures. My mom would always say, “All the doctors I go to tell me, only do antibiotics if it’s life or death.” Why wouldn’t they have medicine if it wasn’t good for you? Immunity. I’d done way too much. If I had a fever, I’d take a hot bath, then I’d start throwing up and that would be enough to kick the system. It’d burn my stomach. It was alcohol, it was antibiotics, it was whatever was destroying the lining. I didn’t learn how to express my emotions as a child. We hold our emotions in our gut.
[The interview continued but the participant addressed content not related to the central research question.]
An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
Publications
Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
Advanced Search
Journal List
Springer Nature - PMC COVID-19 Collection
Transcription and Qualitative Methods: Implications for Third Sector Research
Caitlin mcmullin.
Department of Politics & Society, Aalborg University, Aalborg, Denmark
While there is a vast literature that considers the collection and analysis of qualitative data, there has been limited attention to audio transcription as part of this process. In this paper, I address this gap by discussing the main considerations, challenges and implications of audio transcription for qualitative research on the third sector. I present a framework for conducting audio transcription for researchers and transcribers, as well as recommendations for writing up transcription in qualitative research articles.
Introduction
The field of third sector studies is inherently interdisciplinary, with studies from political science, management, sociology and social work, among others. Within the field of research, a large percentage (between 40–80%) of studies employ qualitative methods such as interviews, focus groups and ethnographic observations (von Schnurbein et al., 2018 ). In order to ensure rigor, qualitative researchers devote considerable time to developing interview guides, consent forms and coding frameworks. While there is a vast literature that considers the collection and the analysis of qualitative data, there has been comparatively limited attention paid to audio transcription, which is the conversion of recorded audio material into a written form that can be analyzed. Despite advances made in qualitative methodologies and increasing attention to positionality, subjectivity and reliability in qualitative data analysis, the transcription of interviews and focus groups is often presented uncritically as a direct conversion of recorded audio to text. As technology to facilitate transcription improves, many researchers have shifted to using voice-to-text software and companies that employ AI rather than human transcription. These technological advances in transcription, along with shifts in the way that research is undertaken (for example, increasingly via video conferencing as a result of the COVID-19 pandemic), mean that the need to critically reflect upon the place of transcription in third sector research is more urgent.
In this article, I explore the place of transcription in qualitative research, with a focus on the importance of this process for third sector researchers. The article is structured as follows. First, I review the qualitative methods literature on audio transcription and the key themes that arise. Next, I report on a review undertaken of recent qualitative research articles in Voluntas and the way that authors discuss transcription in these articles. Finally, I propose a framework for qualitative third sector researchers to include transcription as part of their research design and elements to consider in including descriptions of the transcription process in writing up qualitative research.
Audio Transcription: What We Know
At a basic level, transcription refers to the transformation of recorded audio (usually spoken word) into a written form that can be used to analyze a particular phenomenon or event (Duranti, 2006 ). For many qualitative researchers, transcription has become a fairly taken-for-granted aspect of the research process. In this section, I review the methods literature on the process of audio (and video) transcription as part of qualitative research on the third sector, focusing on three key areas—how transcription is undertaken, epistemological and ethical considerations, and the role of technology.
Qualitative research and transcription
While quantitative research seeks to explain, generalize and predict patterns through the analysis of variables, qualitative research questions are more interested in understanding and interpreting the socially constructed world around us (Bryman, 2016 ). This means that data are collected through documents, observation and interviews, and the latter are often recorded in order to analyze these as documents. For third sector research, recordings are most commonly made of interviews and focus groups, but may also be of meetings, events and other activities to ensure that researchers do not have to rely on their power of recall or scribbled notes.
Transcription is a notoriously time-consuming and often tedious task which can take between three hours and over eight hours to transcribe one hour of audio, depending on typing speed. Transcription is not, however, a mechanical process where the written document becomes an objective record of the event—indeed, written text varies from the spoken word in terms of syntax, word choice and accepted grammar (Davidson, 2009 ). The transcriber therefore has to make subjective decisions throughout about what to include (or not), whether to correct mistakes and edit grammar and repetitions. This has been described as a spectrum between “naturalized” transcription (or “intelligent verbatim”) which adapts the oral to written norms, and “denaturalized” transcription (“full verbatim”), where everything is left in, including utterances, mistakes, repetitions and all grammatical errors (Bucholtz, 2000 ).
While some contend that denaturalized transcription is more ‘accurate’, the same can equally be argued for naturalized, as it allows the transcriber to omit occasions when, for instance, an individual mis-speaks and corrects themselves, thereby allowing the transcriber to record closer to what was intended and how the interviewee might have portrayed themselves in a written form. As Lapadat ( 2000 , p. 206) explains, “Spoken language is structured and accomplished differently than written text, so when talk is re-presented as written text, it is not surprising that readers draw on their knowledge of written language to evaluate it.” Other nonverbal cues, such as laughter, tone of voice (e.g. sarcasm, frustration, emphasis) and the use or omission of punctuation, can also drastically alter the meaning or intention of what an individual says. In addition, the transcriber must make decisions about how much contextual information to include, such as interruptions, crosstalk and inaudible segments (Lapadat, 2000 ). Because of the range of types of research that employ qualitative methods, there is no single set of rules for transcription but rather these decisions must be based on the research questions and approach.
Epistemological and Ethical Considerations
Because the researcher (or external transcriber) must make these decisions as they translate audio into written text, transcription is an inherently interpretative and political act, influenced by the transcriber’s own assumptions and biases (Jaffe, 2007 ). Every choice that the transcriber makes therefore shapes how the research participant is portrayed and determines what knowledge or information is relevant and valuable and what is not. Indeed, two transcribers may hear differently and select relevant spoken material differently (Stelma & Cameron, 2007 ). As Davidson ( 2009 ) notes (and as I explore in further detail in the next section), despite being a highly interpretive process, transcription is frequently depicted using positivist norms of knowledge creation.
Transcription also involves potential ethical considerations and dilemmas. When working with disadvantaged communities, deciding how to depict research participants in written text can highlight the challenges of ethical representation. As Kvale ( 1996 , pp. 172–3) notes, “Be mindful that the publication of incoherent and repetitive verbatim interview transcripts may involve an unethical stigmatization of specific persons or groups of people”. Oliver et al. ( 2005 ) similarly demonstrate how transcribers must make decisions about how to represent participants’ use of slang, colloquialisms and accents in ways that are accurate but also respectful of the respondent’s intended meaning. Some researchers decide to send finished transcriptions to interviewees for approval in order to honor commitments to fully informed consent, to ensure transcription accuracy or in some cases as a means to address the balance of power between the researcher and interviewee. As Mero-Jaffe ( 2011 ) describes, on the one hand, this may empower interviewees to control the way that they are portrayed in the research. On the other hand, Mero-Jaffe found that seeking transcript approval from interviewees sometimes increased their embarrassment at the way that their statements appear in text. This may be especially problematic with full verbatim transcriptions.
Technology and Transcription
As technology improves and AI becomes increasingly able to create written text from recorded audio, researchers might ask—is human transcription even necessary? New options in Computer Assisted Qualitative Data Analysis Software (CAQDAS) such as NVivo, Atlas.ti and MAXQDA give qualitative researchers the option to forgo audio-to-text transcription altogether, and instead engage in live coding of audio or video files. Using this method, researchers first watch or listen to recordings to code for nonverbal cues, followed by a stage of note taking and coding based on pre-defined themes and matching these with time codes and nonverbal cues. Finally, researchers then transcribe specific quotes of interest from the recording (Parameswaran et al., 2020 ). This process may improve immersion in the data and allow researchers to account for dynamics that are often lost in complete audio-to-text transcription, such as group interactions and nonverbal communication.
There is a considerable need to develop the evidence base on the role of AI in transcription for qualitative research, with many important publications that consider the issue (e.g. Gibbs et al., 2002 ; Markle et al., 2011 ) out-of-date given the swift rate of change in AI technologies. Over the last few years, voice and speech recognition technologies have improved dramatically and may now be able to provide researchers with “good enough” first drafts of transcripts (Bokhove & Downey, 2018 ), providing certain conditions are in place (e.g. limited number of speakers and excellent audio quality). Using these technologies can save researchers time and money. As a result of the COVID-19 pandemic, many qualitative researchers are now undertaking interviews over Zoom or other video conferencing apps, which is a trend that may continue beyond the pandemic (Dodds & Hess, 2020 ). Zoom offers AI live transcription options, which benefits from the generally clear audio quality of a video conference, compared to in-person interviews where there is a greater chance of audio interference and background noise that may be undetected in the moment.
While AI may offer a cheaper and quicker alternative to human transcription, these transcripts will need to be meticulously checked by the researcher to ensure accuracy, fill in missing details or edit for context and readability. Using cloud-based AI transcription services also raises potential ethical concerns about data protection and confidentiality (Da Silva, 2021 ). There are numerous subjective decisions made in the course of creating a transcription that AI is unable to process, such as where to include punctuation, which words to include or exclude (such as filler words, hesitations, etc.) and how to denote things such as interruptions, hesitations and nonverbal cues. Voice-to-text software is also generally less accurate in discerning multiple voices or different accents (Bokhove & Downey, 2018 ). Several studies have considered how researchers/transcribers can use voice recognition software to listen and repeat the spoken text of an interview into software as a shortcut to traditional typing transcription (Matheson, 2007 ; Tilley, 2003 ), but the above shortcomings and cautions apply.
Transcription and Third Sector Research
Transcription matters for third sector research because qualitative research methodologies make up a large percentage of studies undertaken on nonprofits—as much as 40–80% of research published in this field (Igalla et al., 2019 ; Laurett & Ferreira, 2018 ; von Schnurbein et al., 2018 ). Audio transcription is particularly important for third sector research for several reasons. In conducting qualitative research (which aims to produce rich, rigorous description) and as third sector researchers (who study organizations that seek to improve society and who may be working with traditionally disenfranchised or disadvantaged communities), we have a particular ethical obligation to ensure that our research provides an accurate depiction of our participants’ lives and the organizations with which they are involved.
However, transcription is perhaps the most underacknowledged aspect of the qualitative research process, and this is also evident in the way that transcription is discussed in research articles. In order to survey the current depiction of the transcription process in third sector research, I undertook a review of the 212 most recent papers in Voluntas that include the word ‘interview’ to explore how qualitative research articles discuss transcription as part of their methodology. 1 Of these papers, 79 were deemed not applicable (because they were quantitative research papers that mentioned interviews in another context, or used the word interview to denote the administering of a structured questionnaire, or systematic review papers reporting on other research). This left 133 articles which were analyzed to explore the extent to which transcription was described—if at all—as part of the research methodology. 2
The analysis (illustrated in Fig. 1 ) found that 41% of papers employing interviews as a research method did not mention transcription at all, while 11% mentioned transcripts but not the process of transcription. It was not clear from these whether or not interviews were recorded or if researchers relied upon written notes taken during interviews, or how information from the oral interview was converted into analyzable text. The most common discussion of transcription (19%) was a simple sentence along the lines of “interviews were recorded and transcribed”, while 26% gave some further information including who undertook the transcription (the researcher(s), a research assistant or a commercial company) or that the interviews were transcribed ‘verbatim’ (with none explaining what they mean by this term). These findings are not dissimilar to a study of qualitative research in nursing, where it was found that 66% of articles reporting solely that interviews were transcribed, and the remaining articles indicated only “full” or “verbatim” to clarify the process (Wellard & McKenna, 2001 ). I also surveyed the first authors’ departmental affiliations/field of study to gauge any differences between academic fields (Table (Table1) 1 ) although there were not considerable differences.
Transcription in Voluntas qualitative articles
Description of transcription and field of first authors
Field
Transcription not discussed or passive mention of transcripts
Discussion of transcription
Interviews not recorded
Total
Business, management & economics
13
17
1
31
42%
55%
3%
Political science and international development
18
8
0
26
69%
31%
Sociology
8
12
0
20
40%
60%
Public policy & public administration
12
6
0
18
67%
33%
Social work
4
7
1
12
33%
58%
8%
Other or field unclear
14
10
2
26
54%
38%
8%
The fact that over half of the Voluntas articles using interviews as a research method make no mention of the transcription process is a problem for transparency in qualitative research. This tendency may be a symptom of the fact that qualitative researchers face greater challenges in academic publishing that disadvantage longer from, in-depth qualitative research to fit within prescribed word limits (Moravcsik, 2014 ). In researchers’ efforts to ensure that qualitative research meets requirements for transparency, rigor and reliability, efforts are concentrated on descriptions of case and participant selection and data analysis while transcription as the conduit between data collection and analysis remains unproblematized. This emphasis reflects the growing influence of positivist views of validity. Ignoring the subjective decisions and theoretical perspectives that determine the creation of a transcript therefore inadvertently presupposes a positivist stance on the objective nature of data which is inconsistent with qualitative methodologies.
A Framework for Undertaking and Reporting on Transcription
As shown in the previous section, there is currently widespread neglect of transcription as part of interpretive qualitative research on the third sector. In this section, I present key elements for third sector researchers to consider in regard to transcription, both to ensure rigor as part of the qualitative research process and in writing up qualitative research, drawing upon examples of good practice from previous research in Voluntas. These recommendations are based on a review of the literature as well as my personal experience as a qualitative researcher, qualitative methods teacher, and professional transcriber.
Before Transcribing: Ethics and Data Management
All decisions regarding research design, data collection and data management should be made at the beginning of a qualitative research project when applying for ethical/IRB approval from one’s university, and this includes transcription. At this stage, the researcher should confirm with their university whether they have a budget for transcription. Undertaking ethical qualitative research means ensuring standards of transparency, informed consent, confidentiality and protection of the data obtained from the research (Blaxter et al., 2001 ). Increasing concerns about data protection and legislation such as GDPR in the European Union have prompted many universities to institute strict rules about where research data can be stored. Some universities do not allow the use of certain cloud servers, such as Dropbox. These considerations should be taken into account when deciding how to undertake and record interviews (Da Silva, 2021 )—for instance, if you are recording using your mobile phone, it is important to be sure you know whether recordings automatically upload to the cloud. For this reason, it may be preferable to use a traditional digital recorder so you can manually download the files to your computer and know exactly where everything is saved.
Before Transcribing: The Interview
Before transcription can even be considered, researchers must ensure that they have a suitable audio recording, which begins with the interview itself—whenever possible, interviews should be conducted in a quiet environment without background noise or interruptions and the audio recording device should be placed close enough to the respondent to pick up their voice clearly. While recording interviews with a mobile phone has become increasingly common and easy, using a backup recording device is always a good idea to mitigate against flat batteries, full memory cards, and human error. If recording with your mobile phone, it’s also critical to remember to place it on airplane mode/‘do not disturb’ for the duration of the interview.
To Transcribe or Not to Transcribe?
While transcription from audio recordings is considered standard practice in qualitative research (Tracy, 2019 ), it is not the only way of undertaking qualitative interviews, and it is important to note that there are many reasons why it may not be desirable, appropriate or possible to record interviews at all. In relation to third sector research, this is most commonly the case in community-based research, research with political elites or research in challenging environments. One article explained that they did not record interviews because: “In sectors marked by fear, intimidation, and strong security apparatuses, recording devices would almost certainly have led to self-censorship and limited our access.” (Atia & Herrold, 2018 , p. 1046). Similarly, researchers may be unable to record in community settings because of sub-optimal recording conditions (e.g. meeting outside, noisy environments, etc.) or because using recording device makes participants uncomfortable or reinforces power relations between the researcher and participants (Quintanilha et al., 2015 ).
If researchers decide not to comprehensively transcribe recordings, or decide not to record qualitative fieldwork at all, this should be noted and explained in relation to methods. Other methods of notetaking and analysis may be more suited to certain types of ethnographic research, such as reflexive journaling (Halcomb & Davidson, 2006 ), or Systematic and Reflexive Interviewing and Reporting—a process by which a researcher and research assistant jointly interview participants and write their own reports that include observations and analyses, which are collaboratively analyzed (Loubere, 2017 ).
How to Transcribe?
Traditionally, transcribers used foot pedals to play, rewind and fast forward tape recordings while they typed. Now that audio files are digital, several free and low cost programs are available (such as Express Scribe and oTranscribe) that let transcribers set up hot keys to perform the same actions without having to navigate away from their transcript document.
The degree of detail to include in transcripts should be decided upon before interviews are transcribed. This is important because previous research has demonstrated that the format selected for transcription significantly impacts how the researcher interprets the data (Mishler, 2003 ; Packer, 2017 ). There is no one best or “most accurate” style of transcription, but rather, a researcher should consider the particular theoretical background and research questions of the study in order to determine where on the scale of full verbatim to intelligent verbatim is most appropriate for the study. Because third sector research is most commonly associated with social science and business disciplines rather than linguistics, it will rarely be necessary or appropriate to employ the conventions of conversation analysis or extreme levels of denaturalized transcription (Bucholtz, 2000 ). Indeed, it might most frequently be appropriate to employ a version of naturalized/intelligent verbatim, so that any participants’ quotes included in written works are more ‘readable’ and do not include excessive repetitions or verbal fillers such as ‘um’.
If the researcher determines that naturalized or intelligent verbatim transcription is the most appropriate for their study, several considerations should be heeded in order to ensure that meaning is not distorted or lost. First, indications of laughter, nonverbal cues (such as sighs, huffs, finger-snaps, sobbing or even blowing raspberries) should be included if these convey important meaning. Other considerations of how to transcribe may be based more on personal preference and the ability to produce a document that is easily analyzable in the researcher’s chosen medium. For instance, wide margins on one side can be useful for researchers who choose to analyze their data on paper or in Microsoft Word, while other more flowing templates will work better to import into software such as NVivo. It can also be useful to include time stamps for unclear or inaudible statements, or at regular intervals (e.g. every minute) which makes it much easier to check a transcript against the original audio.
Who Transcribes?
As discussed in the consideration of qualitative studies, the prevalence of the passive voice when reporting on transcription (i.e. “interviews were transcribed”) obscures the important distinction of who undertook the transcription. If the researcher transcribes recordings themselves, then it is generally acceptable to assume the coherence between the research approach and approach to transcription, as well as the researcher’s confidence that the written transcript is an accurate record of the event/interview that took place. If, however, the researchers choose to outsource transcription to a research assistant or commercial transcription company, then care should be taken to give detailed and thorough instructions about the elements described above. The researcher should also spot check transcripts for accuracy, fill in any missed words/inaudibles and ensure that the transcription document fulfils their expectations in regard to level of verbatim, style and formatting.
Ideally, transcribers should be hired who have specialist knowledge of the subject matter and familiarity with the accents or dialect of the speakers. They should be provided with a key information about the project, such as the research questions, important terms and acronyms. Lapadat ( 2000 ) provides several useful suggestions when hiring transcribers in order to ensure transcription quality and increase rigor. First, rather than fully outsourcing transcription, the researchers can transcribe some interviews or portions of interviews themselves in order to provide an example for transcribers and develop a transcription protocol. Another option when employing research assistants to transcribe interviews is to include them directly in the interviews (either as a co-interviewer or observer), so they have direct involvement in the research and context.
Finally, when working with external transcribers it can also be valuable to encourage transcribers to keep memos of the transcription process or contextual observations and impressions that may not come through in the written text. For instance, does the interviewee sound tired, frustrated, distracted or nervous? Does the interviewer interrupt the respondent frequently (which the transcriber may choose to edit for readability)? Or did the interview take place somewhere public, like a cafe, which may have made the respondent more guarded? Such information is often lost, particularly in projects that involve multiple research team members (for instance, a PI, multiple interviewers, research assistants and/or professional transcribers).
Writing about Transcription
Due to limited space or word limits, it is not typically possible or desirable to include all of the above details in research articles. Instead, at a minimum, researchers should include who transcribed the audio recordings as part of a commitment to ethical and transparent qualitative research. If this was done by anyone other than the researchers, authors should ideally describe the measures taken to ensure accuracy (developing a protocol for transcribers, spot checking, proofreading, sending transcripts to interviewees if appropriate) and ethical considerations (such as data protection and confidentiality).
Second, researchers should indicate the type of transcription—whether selective (pulling out relevant quotes and themes, or transcribing just the ‘gist’), intelligent verbatim/naturalized or full verbatim/denaturalized. The choice of type of transcription should align to the researcher’s epistemological position and theoretical framework.
Finally, researchers should include any other subjective decision-making that took place during the transcription process, in much the same way that researchers are encouraged to be transparent about their subjectivity and positionality in undertaking interviews and analysis of qualitative data (McCorkel & Myers, 2003 ). This may include information about selecting the level of verbatim, working with external transcribers, feedback from interviewees on transcripts or efforts to ensure accuracy of transcripts and coherence with the research approach.
The following quotes provide good examples of how to write about transcription:
The interviews, which were conducted in the native language of the interviewees by six female Hebrew-Arabic-speaking interviewers, were recorded, translated, and transcribed verbatim. […] Immediately following the interview, each interviewer transcribed and translated her interviews into Hebrew. In this manner, we sought to achieve a translation that was as close as possible to the interviewer’s insights regarding the participants, and we regarded the interviewers as active agents in the creation of knowledge. (Yanay-Ventura et al., 2020 , p. 6) Three Spanish speaking investigators transcribed all of the interviews from audio recording devices, checked each other’s transcription for accuracy, and analyzed the interviews using thematic analysis (Braun & Clarke, 2006 ). The transcribers observed the focus groups and took notes on participants’ voices and other identifying traits to help the transcription process go more smoothly. Researchers aided the transcribers in this regard by asking participants at the beginning of the focus groups to introduce themselves using a pseudonym and briefly remark upon how they preferred to spend their time. (Schwingel et al., 2017 , p. 170)
In both of these examples, the authors treat the process of transcription as part of the broader research process, rather than as an automatic conversion of audio to text. While there is limited clarification about the type of transcription (beyond ‘verbatim’), the discussion of the subjective decision-making as part of the transcription process and acknowledgment of the agency of the individuals undertaking transcription increases transparency and therefore rigor.
Conclusions
Qualitative research can help us to understand some of the important issues impacting the third sector in ways that quantitative methods fall short of explaining, such as the ways that individuals and organizations make sense of public policy and societal challenges, how and why organizations design their services and activities in particular ways, and the intricacies of the relationships between boards, executives, staff and volunteers. Qualitative methods training stresses that an interpretivist epistemological position sees knowledge as socially constructed, yet transcription has slipped through the cracks of methodological examination in the process of creating and interpreting meaning.
In this short article, I sought to draw our attention to this important stage of qualitative data collection and analysis and call on third sector researchers to critically reflect upon transcription both in conducting research and in writing about it. I have focused primarily on the transcription of interviews , rather than focus groups or other multi-person events. All of the points raised in my framework transcription apply to these methods of data collection as well; however, there are further issues that need to be taken into consideration regarding focus groups that warrant further attention, such as the issues of power and accuracy of transcription when there are multiple people speaking and interrupting one another. Researchers employing multi-person recordings should therefore devote more time and consideration to transcription. Finally, technology continues to advance in the area of voice recognition, which may save researchers considerable time and/or money in transcription; however, I implore scholars to see transcription through an interpretivist rather than positivist lens, to ensure that the production of written transcripts is not approached as the creation of objective knowledge.
Appendix 1: Articles Reviewed
Aasland, A., Kropp, S., & Meylakhs, A. Y. (2020). Between Collaboration and Subordination: State and Non-state Actors in Russian Anti-drug Policy. Voluntas , 31 (2), 422–436. https://doi.org/10.1007/s11266-019-00158-9
Åberg, P., Einarsson, S., & Reuter, M. (2021). Think Tanks: New Organizational Actors in a Changing Swedish Civil Society. Voluntas , 32 (3), 634–648. https://doi.org/10.1007/s11266-019-00174-9
Afkhami, A., Nasr Isfahani, A., Abzari, M., & Teimouri, H. (2019). Toward a Deep Insight into Employee Participation in Employer-Supported Volunteering in Iranian Organizations: A Grounded Theory. Voluntas , 30 (5), 1036–1053. https://doi.org/10.1007/s11266-019-00141-4
Anasti, T. (2020). The Strategic Action Field of Sex Work and Sex Trafficking: A Case Study of a Contentious Field in Chicago. Voluntas , 31 (1), 169–183. https://doi.org/10.1007/s11266-019-00161-0
Appe, S. (2018). Directions in a Post-aid World? South–South Development Cooperation and CSOs in Latin America. Voluntas , 29 (2), 271–283. https://doi.org/10.1007/s11266-017-9838-0
Arhin, A. A., Kumi, E., & Adam, M.-A. S. (2018). Facing the Bullet? Non-Governmental Organisations’ (NGOs’) Responses to the Changing Aid Landscape in Ghana. Voluntas , 29 (2), 348–360. https://doi.org/10.1007/s11266-018-9966-1
Arvidson, M. (2018). Change and Tensions in Non-profit Organizations: Beyond the Isomorphism Trajectory. Voluntas , 29 (5), 898–910. https://doi.org/10.1007/s11266-018-0021-z
Atia, M., & Herrold, C. E. (2018). Governing Through Patronage: The Rise of NGOs and the Fall of Civil Society in Palestine and Morocco. Voluntas , 29 (5), 1044–1054. https://doi.org/10.1007/s11266-018-9953-6
Ávila, L., & Amorim, M. (2021). Organisational Identity of Social Enterprises: A Taxonomic Approach. Voluntas , 32 (1), 13–27. https://doi.org/10.1007/s11266-020-00264-z
Baillie Smith, M., Fadel, B., O’Loghlen, A., & Hazeldine, S. (2020). Volunteering Hierarchies in the Global South: Remuneration and Livelihoods. Voluntas . https://doi.org/10.1007/s11266-020-00254-1
Bandini, F., Gigli, S., & Mariani, L. (2021). Social Enterprises and Public Value: A Multiple-Case Study Assessment. Voluntas , 32 (1), 61–77. https://doi.org/10.1007/s11266-020-00285-8
Bano, M. (2019). Partnerships and the Good-Governance Agenda: Improving Service Delivery Through State–NGO Collaborations. Voluntas , 30 (6), 1270–1283. https://doi.org/10.1007/s11266-017-9937-y
Barinaga, E. (2020). Coopted! Mission Drift in a Social Venture Engaged in a Cross-Sectoral Partnership. Voluntas , 31 (2), 437–449. https://doi.org/10.1007/s11266-018-0019-6
Bayalieva-Jailobaeva, K. (2018). New Donor Strategies: Implications for NGOs in Post-Soviet Kyrgyzstan. Voluntas , 29 (2), 284–295. https://doi.org/10.1007/s11266-017-9878-5
Beaton, E. E. (2021). No Margin, No Mission: How Practitioners Justify Nonprofit Managerialization. Voluntas , 32 (3), 695–708. https://doi.org/10.1007/s11266-019-00189-2
Bergfeld, A., Plagmann, C., & Lutz, E. (2021). Know Your Counterparts: The Importance of Wording for Stakeholder Communication in Social Franchise Enterprises. Voluntas , 32 (1), 104–119. https://doi.org/10.1007/s11266-020-00289-4
Bidet, E., Eum, H., & Ryu, J. (2018). Diversity of Social Enterprise Models in South Korea. Voluntas , 29 (6), 1261–1273. https://doi.org/10.1007/s11266-018-9951-8
Bies, A., & Kennedy, S. (2019). The State and the State of the Art on Philanthropy in China. Voluntas , 30 (4), 619–633. https://doi.org/10.1007/s11266-019-00142-3
Bradford, A., Luke, B., & Furneaux, C. (2020). Exploring Accountability in Social Enterprise: Priorities, Practicalities, and Legitimacy. Voluntas , 31 (3), 614–626. https://doi.org/10.1007/s11266-020-00215-8
Cannon, S. M. (2020). Legitimacy as Property and Process: The Case of an Irish LGBT Organization. Voluntas , 31 (1), 39–55. https://doi.org/10.1007/s11266-019-00091-x
Carlsen, H. B., Doerr, N., & Toubøl, J. (2020). Inequality in Interaction: Equalising the Helper–Recipient Relationship in the Refugee Solidarity Movement. Voluntas . https://doi.org/10.1007/s11266-020-00268-9
Chatterjee, D., Subramanian, B., & Hota, P. K. (2020). Professionalization and Hybridization Dynamics of Social Enterprises. Voluntas , 31 (3), 457–471. https://doi.org/10.1007/s11266-020-00217-6
Chatzichristos, G., & Nagopoulos, N. (2020). Social Entrepreneurship and Institutional Sustainability: Insights from an Embedded Social Enterprise. Voluntas , 31 (3), 484–493. https://doi.org/10.1007/s11266-019-00188-3
Chaves-Avila, R., & Savall-Morera, T. (2019). The Social Economy in a Context of Austerity Policies: The Tension Between Political Discourse and Implemented Policies in Spain. Voluntas , 30 (3), 487–498. https://doi.org/10.1007/s11266-018-00075-3
Chewinski, M. (2019). Coordinating Action: NGOs and Grassroots Groups Challenging Canadian Resource Extraction Abroad. Voluntas , 30 (2), 356–368. https://doi.org/10.1007/s11266-018-0023-x
Clear, A., Paull, M., & Holloway, D. (2018). Nonprofit Advocacy Tactics: Thinking Inside The Box? Voluntas , 29 (4), 857–869. https://doi.org/10.1007/s11266-017-9907-4
Cookingham Bailey, E. (2020). Advocacy and Service Delivery in the Voluntary Sector: Exploring the History of Voluntary Sector Activities for New Minority and Migrant Groups in East London, 1970s–1990s. Voluntas . https://doi.org/10.1007/s11266-020-00253-2
Crack, A. M. (2018). The Regulation of International NGOS: Assessing the Effectiveness of the INGO Accountability Charter. Voluntas , 29 (2), 419–429. https://doi.org/10.1007/s11266-017-9866-9
Crotty, J., & Ljubownikow, S. (2020). Creating Organisational Strength from Operationalising Restrictions: Welfare Non-profit Organisations in the Russian Federation. Voluntas , 31 (6), 1148–1158. https://doi.org/10.1007/s11266-020-00271-0
Deng, G. (2019). Trends in Overseas Philanthropy by Chinese Foundations. Voluntas , 30 (4), 678–691. https://doi.org/10.1007/s11266-017-9868-7
Dinh, K., Hong, K. T., Haire, B., & Worth, H. (2021). Historic and Contemporary Influences on HIV Advocacy in Vietnam. Voluntas , 32 (3), 610–620. https://doi.org/10.1007/s11266-020-00220-x
Dong, Q., Guo, J., & Huang, C.-C. (2019). Nonprofit Alliance in China: Effects of Alliance Process on Goal Achievement. Voluntas , 30 (2), 300–311. https://doi.org/10.1007/s11266-018-9990-1
Edenfield, A. C., & Andersson, F. O. (2018). Growing Pains: The Transformative Journey from a Nascent to a Formal Not-For-Profit Venture. Voluntas , 29 (5), 1033–1043. https://doi.org/10.1007/s11266-017-9936-z
Elsayed, Y. (2018). At the Intersection of Social Entrepreneurship and Social Movements: The Case of Egypt and the Arab Spring. Voluntas , 29 (4), 819–831. https://doi.org/10.1007/s11266-017-9943-0
Eschweiler, J., Svensson, S., Mocca, E., Cartwright, A., & Villadsen Nielsen, L. (2019). The Reciprocity Dimension of Solidarity: Insights from Three European Countries. Voluntas , 30 (3), 549–561. https://doi.org/10.1007/s11266-018-0031-x
Eynaud, P., Juan, M., & Mourey, D. (2018). Participatory Art as a Social Practice of Commoning to Reinvent the Right to the City. Voluntas , 29 (4), 621–636. https://doi.org/10.1007/s11266-018-0006-y
Falkenhain, M. (2020). Dividing Lines: Understanding the Creation and Replication of Fragmentations Among NGOs in Hybrid Regimes. Voluntas , 31 (4), 663–673. https://doi.org/10.1007/s11266-019-00185-6
Fang, Q., Fisher, K. R., & Li, B. (2020). Follower or Challenger? How Chinese Non-governmental Organizations Manage Accountability Requirements from Funders. Voluntas , 31 (4), 722–735. https://doi.org/10.1007/s11266-019-00184-7
Farid, M., & Li, H. (2021). Reciprocal Engagement and NGO Policy Influence on the Local State in China. Voluntas , 32 (3), 597–609. https://doi.org/10.1007/s11266-020-00288-5
Fehsenfeld, M., & Levinsen, K. (2019). Taking Care of the Refugees: Exploring Advocacy and Cross-sector Collaboration in Service Provision for Refugees. Voluntas , 30 (2), 422–435. https://doi.org/10.1007/s11266-019-00097-5
Ferguson, G. (2018). The Social Economy in Bolivia: Indigeneity, Solidarity, and Alternatives to Capitalism. Voluntas , 29 (6), 1233–1243. https://doi.org/10.1007/s11266-018-0013-z
Fulton, B. R., & Wood, R. L. (2018). Civil Society Organizations and the Enduring Role of Religion in Promoting Democratic Engagement. Voluntas , 29 (5), 1068–1079. https://doi.org/10.1007/s11266-018-9965-2
Gaby, S. (2020). Reconfiguring Organizational Commitments: Boundary Crossing in Civic Groups. Voluntas , 31 (6), 1121–1133. https://doi.org/10.1007/s11266-020-00272-z
Gaeta, G. L., Ghinoi, S., Silvestri, F., & Trasciani, G. (2021). Exploring Networking of Third Sector Organizations: A Case Study Based on the Quartieri Spagnoli Neighborhood in Naples (Italy). Voluntas , 32 (4), 750–766. https://doi.org/10.1007/s11266-020-00241-6
García-Orosa, B., & Pérez-Seijo, S. (2020). The Use of 360° Video by International Humanitarian Aid Organizations to Spread Social Messages and Increase Engagement. Voluntas , 31 (6), 1311–1329. https://doi.org/10.1007/s11266-020-00280-z
Grazioli, M., & Caciagli, C. (2018). Resisting to the Neoliberal Urban Fabric: Housing Rights Movements and the Re-appropriation of the ‘Right to the City’ in Rome, Italy. Voluntas , 29 (4), 697–711. https://doi.org/10.1007/s11266-018-9977-y
Grubb, A., & Henriksen, L. S. (2019). On the Changing Civic Landscape in Denmark and its Consequences for Civic Action. Voluntas , 30 (1), 62–73. https://doi.org/10.1007/s11266-018-00054-8
Guha, P. (2019). Going to Scale: A Case Study of an Indian Educational NGO. Voluntas , 30 (6), 1365–1379. https://doi.org/10.1007/s11266-019-00099-3
Guo, C., & Lai, W. (2019). Community Foundations in China: In Search of Identity? Voluntas , 30 (4), 647–663. https://doi.org/10.1007/s11266-017-9932-3
Heckert, R., Boumans, J., & Vliegenthart, R. (2020). How to Nail the Multiple Identities of an Organization? A Content Analysis of Projected Identity. Voluntas , 31 (1), 129–141. https://doi.org/10.1007/s11266-019-00157-w
Heideman, L. J. (2018). Making Civil Society Sustainable: The Legacy of USAID in Croatia. Voluntas , 29 (2), 333–347. https://doi.org/10.1007/s11266-017-9896-3
Hjort, M., & Beswick, D. (2020). Volunteering and Policy Makers: The Political Uses of the UK Conservative Party’s International Development Volunteering Projects. Voluntas . https://doi.org/10.1007/s11266-020-00222-9
Holthaus, L. (2019). Furthering Pluralism? The German Foundations in Transitional Tunisia. Voluntas , 30 (6), 1284–1296. https://doi.org/10.1007/s11266-018-00074-4
Horvath, A. (2020). The Transformative Potential of Experience: Learning, Group Dynamics, and the Development of Civic Virtue in a Mobile Soup Kitchen. Voluntas , 31 (5), 981–994. https://doi.org/10.1007/s11266-018-00062-8
Horvath, A., Brandtner, C., & Powell, W. W. (2018). Serve or Conserve: Mission, Strategy, and Multi-Level Nonprofit Change During the Great Recession. Voluntas , 29 (5), 976–993. https://doi.org/10.1007/s11266-017-9948-8
Huang, Y. (2019). At the Mercy of the State: Health Philanthropy in China. Voluntas , 30 (4), 634–646. https://doi.org/10.1007/s11266-018-9960-7
Ismail, A., & Johnson, B. (2019). Managing Organizational Paradoxes in Social Enterprises: Case Studies from the MENA Region. Voluntas , 30 (3), 516–534. https://doi.org/10.1007/s11266-018-00083-3
Jezierska, K., & Polanska, D. V. (2018). Social Movements Seen as Radical Political Actors: The Case of the Polish Tenants’ Movement. Voluntas , 29 (4), 683–696. https://doi.org/10.1007/s11266-017-9917-2
Kampen, T., Veldboer, L., & Kleinhans, R. (2019). The Obligation to Volunteer as Fair Reciprocity? Welfare Recipients’ Perceptions of Giving Back to Society. Voluntas , 30 (5), 991–1005. https://doi.org/10.1007/s11266-018-00082-4
Kang, Y. (2019). What Does China’s Twin-Pillared NGO Funding Game Entail? Growing Diversity and Increasing Isomorphism. Voluntas , 30 (3), 499–515. https://doi.org/10.1007/s11266-018-00085-1
Kappelides, P., Cuskelly, G., & Hoye, R. (2019). The Influence of Volunteer Recruitment Practices and Expectations on the Development of Volunteers’ Psychological Contracts. Voluntas , 30 (1), 259–271. https://doi.org/10.1007/s11266-018-9986-x
Kennedy, D. (2019). The Inherently Contested Nature of Nongovernmental Accountability: The Case of HAP International. Voluntas , 30 (6), 1393–1405. https://doi.org/10.1007/s11266-019-00134-3
Kewes, A., & Munsch, C. (2019). Should I Stay or Should I Go? Engaging and Disengaging Experiences in Welfare-Sector Volunteering. Voluntas , 30 (5), 1090–1103. https://doi.org/10.1007/s11266-019-00122-7
Korstenbroek, T., & Smets, P. (2019). Developing the Potential for Change: Challenging Power Through Social Entrepreneurship in the Netherlands. Voluntas , 30 (3), 475–486. https://doi.org/10.1007/s11266-019-00107-6
Koubek, M. (2020). When Did They Protest? Beyond Co-optation or Channeling: Effects of EU Funding on Czech Romani NGOs and Civil Society. Voluntas , 31 (2), 404–421. https://doi.org/10.1007/s11266-018-0008-9
Kravchenko, Z., & Moskvina, A. (2018). Entrepreneurial NPOs in Russia: Rationalizing the Mission. Voluntas , 29 (5), 962–975. https://doi.org/10.1007/s11266-018-0016-9
Kumi, E. (2019). Aid Reduction and NGDOs’ Quest for Sustainability in Ghana: Can Philanthropic Institutions Serve as Alternative Resource Mobilisation Routes? Voluntas , 30 (6), 1332–1347. https://doi.org/10.1007/s11266-017-9931-4
Lall, S. A. (2019). From Legitimacy to Learning: How Impact Measurement Perceptions and Practices Evolve in Social Enterprise–Social Finance Organization Relationships. Voluntas , 30 (3), 562–577. https://doi.org/10.1007/s11266-018-00081-5
Lang, R., & Mullins, D. (2020). Field Emergence in Civil Society: A Theoretical Framework and Its Application to Community-Led Housing Organisations in England. Voluntas , 31 (1), 184–200. https://doi.org/10.1007/s11266-019-00138-z
Laurent, A., Garaudel, P., Schmidt, G., & Eynaud, P. (2020). Civil Society Meta-organizations and Legitimating Processes: The Case of the Addiction Field in France. Voluntas , 31 (1), 19–38. https://doi.org/10.1007/s11266-019-00094-8
Lee, E. K. M., & Chandra, Y. (2020). Dynamic and Marketing Capabilities as Predictors of Social Enterprises’ Performance. Voluntas , 31 (3), 587–600. https://doi.org/10.1007/s11266-019-00155-y
Li, S. (2020). Global Civil Society Under the New INGO Regulatory Law: A Comparative Case Study on Two INGOs in China. Voluntas , 31 (4), 751–761. https://doi.org/10.1007/s11266-019-00101-y
Liu, F., & Zhang, X. (2020). Who are Volunteers in Urban China? Voluntas . https://doi.org/10.1007/s11266-020-00251-4
Lund, V., & Juujärvi, S. (2018). Residents’ Agency Makes a Difference in Volunteering in an Urban Neighbourhood. Voluntas , 29 (4), 756–769. https://doi.org/10.1007/s11266-018-9955-4
Marie, B., Isabelle, M., Jordan, B.-L., Hélène, C., Sophie, É., Julie, F., Christine, M., & Andrée, S. (2020). Promising Practices of Nonprofit Organizations to Respond to the Challenges Faced in Countering the Mistreatment of Older Adults. Voluntas , 31 (6), 1359–1370. https://doi.org/10.1007/s11266-020-00252-3
Martinez, D. E., & Cooper, D. J. (2020). Seeing Through the Logical Framework. Voluntas , 31 (6), 1239–1253. https://doi.org/10.1007/s11266-020-00223-8
Mathews, M. A. (2020). The Embeddedness of Nonprofit Leadership in Civic Governance. Voluntas , 31 (1), 201–212. https://doi.org/10.1007/s11266-019-00139-y
Mati, J. M. (2020). Civil Society in ‘Politics’ and ‘Development’ in African Hybrid Regimes: The Kenyan Case. Voluntas , 31 (4), 674–687. https://doi.org/10.1007/s11266-020-00211-y
Maya-Jariego, I., Holgado-Ramos, D., González-Tinoco, E., Muñoz-Alvis, A., & Ortega, M. (2020). More Money, More Problems? Resource Dependence and Professionalization of Non-governmental Social Services Organizations in Southern Spain. Voluntas , 31 (6), 1212–1225. https://doi.org/10.1007/s11266-020-00256-z
McLennan, B. J. (2020). Conditions for Effective Coproduction in Community-Led Disaster Risk Management. Voluntas , 31 (2), 316–332. https://doi.org/10.1007/s11266-018-9957-2
McMullin, C., & Skelcher, C. (2018). The Impact of Societal-Level Institutional Logics on Hybridity: Evidence from Nonprofit Organizations in England and France. Voluntas , 29 (5), 911–924. https://link.springer.com/article/10.1007/s11266-018-9996-8
Meijs, L., Handy, F., Simons, F.-J., & Roza, L. (2020). A Social Innovation: Addressing Relative Food Insecurity and Social Exclusion. Voluntas , 31 (5), 894–906. https://doi.org/10.1007/s11266-019-00105-8
Meyer, M., & Simsa, R. (2018). Organizing the Unexpected: How Civil Society Organizations Dealt with the Refugee Crisis. Voluntas , 29 (6), 1159–1175. https://doi.org/10.1007/s11266-018-00050-y
Mikołajczak, P. (2020). Social Enterprises’ Hybridity in the Concept of Institutional Logics: Evidence from Polish NGOs. Voluntas , 31 (3), 472–483. https://doi.org/10.1007/s11266-020-00195-9
Milbourn, B., Black, M. H., & Buchanan, A. (2019). Why People Leave Community Service Organizations: A Mixed Methods Study. Voluntas , 30 (1), 272–281. https://doi.org/10.1007/s11266-018-0005-z
Molina, J. L., Valenzuela-García, H., Lubbers, M. J., Escribano, P., & Lobato, M. M. (2018). “The Cowl Does Make The Monk”: Understanding the Emergence of Social Entrepreneurship in Times of Downturn. Voluntas , 29 (4), 725–739. https://doi.org/10.1007/s11266-017-9921-6
Moraes, R. L., & Andion, C. (2018). Civil Society and Social Innovation in Public Arenas in Brazil: Trajectory and Experience of the Movement Against Electoral Corruption (MCCE). Voluntas , 29 (4), 801–818. https://doi.org/10.1007/s11266-017-9867-8
Morais-da-Silva, R. L., Segatto, A. P., & Bezerra-de-Sousa, I. G. (2020). Connecting Two Sides: A Qualitative Study on Social Innovation Ventures and Poor Communities in an Emerging Economy. Voluntas , 31 (5), 966–980. https://doi.org/10.1007/s11266-019-00156-x
Musah-Surugu, I. J., Bawole, J. N., & Ahenkan, A. (2019). The “Third Sector” and Climate Change Adaptation Governance in Sub-Saharan Africa: Experience from Ghana. Voluntas , 30 (2), 312–326. https://doi.org/10.1007/s11266-018-9962-5
Mutongwizo, T. (2018). Comparing NGO Resilience and ‘Structures of Opportunity’ in South Africa and Zimbabwe (2010–2013). Voluntas , 29 (2), 373–387. https://doi.org/10.1007/s11266-017-9881-x
Näslund, H. (2020). Collective Deliberations and Hearts on Fire: Experiential Knowledge Among Entrepreneurs and Organisations in the Mental Health Service User Movement. Voluntas . https://doi.org/10.1007/s11266-020-00233-6
Nimu, A. (2018). Surviving Mechanisms and Strategies of Gender Equality NGOs in Romania and Poland. Voluntas , 29 (2), 310–332. https://doi.org/10.1007/s11266-018-9961-6
Noh, J.-E. (2019). Human Rights-Based Child Sponsorship: A Case Study of ActionAid. Voluntas , 30 (6), 1420–1432. https://doi.org/10.1007/s11266-018-0010-2
Obaze, Y. (2020). Supply Chain Challenges and Shared Value Destruction in the Community-Based Supply Chain. Voluntas , 31 (3), 550–562. https://doi.org/10.1007/s11266-020-00202-z
Onyx, J., Darcy, S., Grabowski, S., Green, J., & Maxwell, H. (2018). Researching the Social Impact of Arts and Disability: Applying a New Empirical Tool and Method. Voluntas , 29 (3), 574–589. https://doi.org/10.1007/s11266-018-9968-z
Pape, U., Brandsen, T., Pahl, J. B., Pieliński, B., Baturina, D., Brookes, N., Chaves-Ávila, R., Kendall, J., Matančević, J., Petrella, F., Rentzsch, C., Richez-Battesti, N., Savall-Morera, T., Simsa, R., & Zimmer, A. (2020). Changing Policy Environments in Europe and the Resilience of the Third Sector. Voluntas , 31 (1), 238–249. https://doi.org/10.1007/s11266-018-00087-z
Parker, M. A., Mook, L., Kao, C.-Y., & Murdock, A. (2020). Accountability and Relationship-Definition Among Food Banks Partnerships. Voluntas , 31 (5), 923–937. https://doi.org/10.1007/s11266-019-00150-3
Peci, A., Oquendo, M. I., & Mendonça, P. (2020). Collaboration, (Dis)trust and Control in Brazilian Manufactured Public/Non-profit Partnerships. Voluntas , 31 (2), 375–389. https://doi.org/10.1007/s11266-018-0027-6
Peralta, K. J., & Vaitkus, E. (2019). Constructing Action: An Analysis of the Roles of Third Sector Actors During the Implementation of the Dominican Republic’s Regularization Plan. Voluntas , 30 (6), 1319–1331. https://doi.org/10.1007/s11266-018-0003-1
Pettigrew, S., Jongenelis, M., Jackson, B., & Newton, R. U. (2019). “Charity Begins at Home”: Informal Caring Barriers to Formal Volunteering Among Older People. Voluntas , 30 (5), 921–931. https://doi.org/10.1007/s11266-018-0017-8
Pfeilstetter, R. (2020). Doing Good and Selling Goods. Voluntas , 31 (3), 511–520. https://doi.org/10.1007/s11266-020-00194-w
Pixová, M. (2018). The Empowering Potential of Reformist Urban Activism in Czech Cities. Voluntas , 29 (4), 670–682. https://doi.org/10.1007/s11266-018-0011-1
Pluciński, P. (2018). Forces of Altermodernization: Urban Social Movements and the New Urban Question in Contemporary Poland. Voluntas , 29 (4), 653–669. https://doi.org/10.1007/s11266-018-0007-x
Popplewell, R. (2018). Civil Society, Legitimacy and Political Space: Why Some Organisations are More Vulnerable to Restrictions than Others in Violent and Divided Contexts. Voluntas , 29 (2), 388–403. https://doi.org/10.1007/s11266-018-9949-2
Puljek-Shank, R. (2018). Civic Agency in Governance: The Role of Legitimacy with Citizens vs. Donors. Voluntas , 29 (4), 870–883. https://doi.org/10.1007/s11266-018-0020-0
Reijnders, M., Schalk, J., & Steen, T. (2018). Services Wanted? Understanding the Non-take-up of Social Support at the Local Level. Voluntas , 29 (6), 1360–1374. https://doi.org/10.1007/s11266-018-00060-w
Ruiz Sportmann, A. S., & Greenspan, I. (2019). Relational Interactions Between Immigrant and Native-Born Volunteers: Trust-Building and Integration or Suspicion and Conflict? Voluntas , 30 (5), 932–946. https://doi.org/10.1007/s11266-019-00108-5
Sandberg, B., Elliott, E., & Petchel, S. (2020). Investigating the Marketization of the Nonprofit Sector: A Comparative Case Study of Two Nonprofit Organizations. Voluntas , 31 (3), 494–510. https://doi.org/10.1007/s11266-019-00159-8
Schmid, H., & Almog-Bar, M. (2020). The Critical Role of the Initial Stages of Cross-Sector Partnerships and Their Implications for Partnerships’ Outcomes. Voluntas , 31 (2), 286–300. https://doi.org/10.1007/s11266-019-00137-0
Sepulveda, L., Lyon, F., & Vickers, I. (2020). Implementing Democratic Governance and Ownership: The Interplay of Structure and Culture in Public Service Social Enterprises. Voluntas , 31 (3), 627–641. https://doi.org/10.1007/s11266-020-00201-0
Shier, M. L., & Handy, F. (2020). Leadership in Nonprofits: Social Innovations and Blurring Boundaries. Voluntas , 31 (2), 333–344. https://doi.org/10.1007/s11266-018-00078-0
Spencer, S. B., & Skalaban, I. A. (2018). Organizational Culture in Civic Associations in Russia. Voluntas , 29 (5), 1080–1097. https://doi.org/10.1007/s11266-017-9925-2
Stewart, A. J., & Twumasi, A. (2020). Minding the Gap: An Exploratory Study Applying Theory to Nonprofit Board Management of Executive Transitions. Voluntas , 31 (6), 1268–1281. https://doi.org/10.1007/s11266-020-00244-3
Stougaard, M. S. (2020). Co-producing Public Welfare Services with Vulnerable Citizens: A Case Study of a Danish-Somali Women’s Association Co-producing Crime Prevention with the Local Authorities. Voluntas . https://doi.org/10.1007/s11266-020-00235-4
Strichman, N., Marshood, F., & Eytan, D. (2018). Exploring the Adaptive Capacities of Shared Jewish–Arab Organizations in Israel. Voluntas , 29 (5), 1055–1067. https://doi.org/10.1007/s11266-017-9904-7
Suter, P., & Gmür, M. (2018). Volunteer Engagement in Housing Co-operatives: Civil Society “en miniature”. Voluntas , 29 (4), 770–789. https://doi.org/10.1007/s11266-018-9959-0
Svensson, K., & Gallo, C. (2018). The Creation of an Unsolicited Organization: Victim Support Sweden. Voluntas , 29 (5), 1008–1018. https://doi.org/10.1007/s11266-018-9978-x
Tadesse, H. A., & Steen, T. (2019). Exploring the Impact of Political Context on State–Civil Society Relations: Actors’ Strategies in a Developmental State. Voluntas , 30 (6), 1256–1269. https://doi.org/10.1007/s11266-018-00077-1
Taylor, R., Torugsa, N. (Ann), & Arundel, A. (2020). Organizational Pathways for Social Innovation and Societal Impacts in Disability Nonprofits. Voluntas , 31 (5), 995–1012. https://doi.org/10.1007/s11266-019-00113-8
Uzcanga, C., & Oiarzabal, P. J. (2019). Associations of Migrants in Spain: An Enquiry into Their Digital Inclusion in the “Network Society” in the 2010s. Voluntas , 30 (5), 947–961. https://doi.org/10.1007/s11266-019-00162-z
van der Veer, L. (2020). Treacherous Elasticity, Callous Boundaries: Aspiring Volunteer Initiatives in the Field of Refugee Support in Rotterdam. Voluntas . https://doi.org/10.1007/s11266-020-00260-3
van Wessel, M., Naz, F., & Sahoo, S. (2021). Complementarities in CSO Collaborations: How Working with Diversity Produces Advantages. Voluntas , 32 (4), 717–730. https://doi.org/10.1007/s11266-020-00227-4
Vandepitte, E., Vandermoere, F., & Hustinx, L. (2019). Civil Anarchizing for the Common Good: Culturally Patterned Politics of Legitimacy in the Climate Justice Movement. Voluntas , 30 (2), 327–341. https://doi.org/10.1007/s11266-018-00073-5
Vuković, D. (2018). The Quest for Government Accountability and Rule of Law: Conflicting Strategies of State and Civil Society in Cambodia and Serbia. Voluntas , 29 (3), 590–602. https://doi.org/10.1007/s11266-018-9984-z
Waardenburg, M. (2021). Understanding the Microfoundations of Government–Civil Society Relations. Voluntas , 32 (3), 548–560. https://doi.org/10.1007/s11266-020-00221-w
Wells, R., & Anasti, T. (2020). Hybrid Models for Social Change: Legitimacy Among Community-Based Nonprofit Organizations. Voluntas , 31 (6), 1134–1147. https://doi.org/10.1007/s11266-019-00126-3
Williamson, A. K., Luke, B., & Furneaux, C. (2021). Ties That Bind: Public Foundations in Dyadic Partnerships. Voluntas , 32 (2), 234–246. https://doi.org/10.1007/s11266-020-00269-8
Yanay-Ventura, G. (2019). “Nothing About Us Without Us” in Volunteerism Too: Volunteering Among People with Disabilities. Voluntas , 30 (1), 147–163. https://doi.org/10.1007/s11266-018-0026-7
Yanay-Ventura, G., Issaq, L., & Sharabi, M. (2020). Civic Service and Social Class: The Case of Young Arab Women in Israel. Voluntas . https://doi.org/10.1007/s11266-020-00210-z
Zhang, Y., Bradtke, M., & Halvey, M. (2020). Anxiety and Ambivalence: NGO–Activist Partnership in China’s Environmental Protests, 2007–2016. Voluntas , 31 (4), 779–792. https://doi.org/10.1007/s11266-020-00237-2
Zihnioğlu, Ö. (2019). The Prospects of Civic Alliance: New Civic Activists Acting Together with Civil Society Organizations. Voluntas , 30 (2), 289–299. https://doi.org/10.1007/s11266-018-0032-9
No funding was received to assist with the preparation of this manuscript.
Declarations
The author declares that they have no conflict of interest.
1 While this approach may have obscured other methods that employ transcription, such as focus groups, the intention of the survey is to provide a snapshot illustration of transcription and qualitative methods rather than a systematic review.
2 Articles reviewed are listed in Appendix 1.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Atia M, Herrold CE. Governing through patronage: The rise of NGOs and the fall of civil society in Palestine and Morocco. VOLUNTAS: International Journal of Voluntary and Nonprofit Organizations. 2018; 29 (5):1044–1054. doi: 10.1007/s11266-018-9953-6. [ CrossRef ] [ Google Scholar ]
Blaxter, L., Hughes, C., & Tight, M. (2001). How to research (2nd ed.). Open University Press.
Bokhove C, Downey C. Automated generation of “good enough” transcripts as a first step to transcription of audio-recorded data. Methodological Innovations. 2018; 11 (2):2059799118790743. doi: 10.1177/2059799118790743. [ CrossRef ] [ Google Scholar ]
Braun V, Clarke V. Using thematic analysis in psychology. Qualitative Research in Psychology. 2006; 3 (2):77–101. doi: 10.1191/1478088706qp063oa. [ CrossRef ] [ Google Scholar ]
Bryman, A. (2016). Social research methods (5th ed.). Oxford University Press.
Bucholtz M. The politics of transcription. Journal of Pragmatics. 2000; 32 (10):1439–1465. doi: 10.1016/S0378-2166(99)00094-6. [ CrossRef ] [ Google Scholar ]
Da Silva J. Producing ‘good enough’ automated transcripts securely: Extending Bokhove and Downey (2018) to address security concerns. Methodological Innovations. 2021; 14 (1):2059799120987766. doi: 10.1177/2059799120987766. [ CrossRef ] [ Google Scholar ]
Davidson C. Transcription: Imperatives for qualitative research. International Journal of Qualitative Methods. 2009; 8 (2):35–52. doi: 10.1177/160940690900800206. [ CrossRef ] [ Google Scholar ]
Dodds S, Hess AC. Adapting research methodology during COVID-19: Lessons for transformative service research. Journal of Service Management. 2020; 32 (2):203–217. doi: 10.1108/JOSM-05-2020-0153. [ CrossRef ] [ Google Scholar ]
Duranti A. Transcripts, like shadows on a wall. Mind, Culture, and Activity. 2006; 13 (4):301–310. doi: 10.1207/s15327884mca1304_3. [ CrossRef ] [ Google Scholar ]
Gibbs, G. R., Friese, S., & Mangabeira, W. C. (2002). View of the use of new technology in qualitative research. Orum Qualitative Sozialforschung/Forum: Qualitative Social Research , 3 (2). https://www.qualitative-research.net/index.php/fqs/article/view/847/1840
Halcomb EJ, Davidson PM. Is verbatim transcription of interview data always necessary? Applied Nursing Research. 2006; 19 (1):38–42. doi: 10.1016/j.apnr.2005.06.001. [ PubMed ] [ CrossRef ] [ Google Scholar ]
Igalla M, Edelenbos J, van Meerkerk I. Citizens in action, what do they accomplish? A systematic literature review of citizen initiatives, their main characteristics, outcomes, and factors. VOLUNTAS: International Journal of Voluntary and Nonprofit Organizations. 2019; 30 (5):1176–1194. doi: 10.1007/s11266-019-00129-0. [ CrossRef ] [ Google Scholar ]
Jaffe A. Variability in transcription and the complexities of representation, authority and voice. Discourse Studies. 2007; 9 (6):831–836. doi: 10.1177/1461445607082584. [ CrossRef ] [ Google Scholar ]
Kvale, S. (1996). Interviews: An introduction to qualitative research interviewing . Sage.
Lapadat JC. Problematizing transcription: Purpose, paradigm and quality. International Journal of Social Research Methodology. 2000; 3 (3):203–219. doi: 10.1080/13645570050083698. [ CrossRef ] [ Google Scholar ]
Laurett R, Ferreira JJ. Strategy in nonprofit organisations: A systematic literature review and agenda for future research. VOLUNTAS: International Journal of Voluntary and Nonprofit Organizations. 2018; 29 (5):881–897. doi: 10.1007/s11266-017-9933-2. [ CrossRef ] [ Google Scholar ]
Loubere, N. (2017). Questioning transcription: The case for the systematic and reflexive interviewing and reporting (SRIR) method. Forum Qualitative Sozialforschung/Forum: Qualitative Social Research , 18 (2), Article 2. 10.17169/fqs-18.2.2739
Markle, D. T., West, R. E., & Rich, P. J. (2011). Beyond transcription: Technology, change, and refinement of method. Forum Qualitative Sozialforschung/Forum: Qualitative Social Research , 12 (3), Article 3. 10.17169/fqs-12.3.1564
Matheson JL. The voice transcription technique: Use of voice recognition software to transcribe digital interview data in qualitative research. Qualitative Report. 2007; 12 (4):547–560. [ Google Scholar ]
McCorkel JA, Myers K. What difference does difference make? Position and privilege in the field. Qualitative Sociology. 2003; 26 (2):199–231. doi: 10.1023/A:1022967012774. [ CrossRef ] [ Google Scholar ]
Mero-Jaffe I. ‘Is that what I Said?’ Interview transcript approval by participants: An aspect of ethics in qualitative research. International Journal of Qualitative Methods. 2011; 10 (3):231–247. doi: 10.1177/160940691101000304. [ CrossRef ] [ Google Scholar ]
Mishler, E. (2003). Representing discourse: The rhetoric of transcription. In N. Fielding (Ed.), Interviewing . Sage.
Moravcsik, A. (2014). Transparency: The revolution in qualitative research. PS: Political Science & Politics , 47 (1), 48–53. 10.1017/S1049096513001789
Oliver DG, Serovich JM, Mason TL. Constraints and opportunities with interview transcription: Towards reflection in qualitative research. Social Forces. 2005; 84 (2):1273–1289. doi: 10.1353/sof.2006.0023. [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
Packer MJ. The science of qualitative research. Cambridge University Press; 2017. [ Google Scholar ]
Parameswaran UD, Ozawa-Kirk JL, Latendresse G. To live (code) or to not: A new method for coding in qualitative research. Qualitative Social Work. 2020; 19 (4):630–644. doi: 10.1177/1473325019840394. [ CrossRef ] [ Google Scholar ]
Quintanilha M, Mayan MJ, Thompson J, Bell RC. Different approaches to cross-lingual focus groups: Lessons from a cross-cultural community-based participatory research project in the ENRICH study. International Journal of Qualitative Methods. 2015; 14 (5):1609406915621419. doi: 10.1177/1609406915621419. [ CrossRef ] [ Google Scholar ]
Schwingel, A., Wiley, A., Teran-Garcia, M., McCaffrey, J., Gálvez, P., Hawn, R., Villegas, E., Coba, S., Vizcarra, M., Luty, G., Montez, R., & The Abriendo Caminos Promotora Project Group. (2017). More than help? Volunteerism in US Latino culture. VOLUNTAS: International Journal of Voluntary and Nonprofit Organizations , 28 (1), 162–183. 10.1007/s11266-016-9731-2
Stelma JH, Cameron LJ. Intonation units in spoken interaction: Developing transcription skills. Text & Talk. 2007; 27 (3):361–393. doi: 10.1515/TEXT.2007.015. [ CrossRef ] [ Google Scholar ]
Tilley SA. “Challenging” research practices: Turning a critical lens on the work of transcription. Qualitative Inquiry. 2003; 9 (5):750–773. doi: 10.1177/1077800403255296. [ CrossRef ] [ Google Scholar ]
Tracy, S. J. (2019). Qualitative research methods: Collecting evidence, crafting analysis (2nd ed.). John Wiley & Sons.
von Schnurbein G, Perez M, Gehringer T. Nonprofit comparative research: Recent agendas and future trends. VOLUNTAS: International Journal of Voluntary and Nonprofit Organizations. 2018; 29 (3):437–453. doi: 10.1007/s11266-017-9877-6. [ CrossRef ] [ Google Scholar ]
Wellard S, McKenna L. Turning tapes into text: Issues surrounding the transcription of interviews. Contemporary Nurse. 2001; 11 (2–3):180–186. doi: 10.5172/conu.11.2-3.180. [ PubMed ] [ CrossRef ] [ Google Scholar ]
Yanay-Ventura, G., Issaq, L., & Sharabi, M. (2020). Civic service and social class: The case of young Arab women in Israel. VOLUNTAS: International Journal of Voluntary and Nonprofit Organizations . 10.1007/s11266-020-00210-z
Home > Blog >
Transcription in qualitative research: a comprehensive guide for ux researchers, theertha raj.
August 15, 2024
As a UX researcher, you're likely familiar with the importance of gathering qualitative data through interviews, focus groups, and observational studies. But what happens after you've collected all that valuable audio or video content? That's where transcription for qualitative research comes into play.
In this article, we'll dive deep into the world of transcription, exploring its importance, types, and best practices for UX researchers.
What is transcription in qualitative research?
Transcription in qualitative research is the process of converting spoken words or recorded audio into written text.
This crucial step allows researchers to analyze, code, and interpret the data collected during interviews, focus groups, or other qualitative research methods.
This written format makes it easier to review, share, and analyze the data, ultimately leading to more informed design choices and improved user experiences.
What are the 4 types of transcription?
When it comes to transcription qualitative research, there are four main types that researchers should be aware of:
Verbatim transcription: This type captures every utterance, including filler words, false starts, and non-verbal sounds. It's the most detailed form of transcription and is often used when analyzing speech patterns or conducting linguistic studies.
Intelligent verbatim transcription: Also known as "clean verbatim," this type removes filler words and false starts while maintaining the essence of the conversation. It's more readable than strict verbatim transcription and is commonly used in qualitative research.
This type focuses on capturing the main ideas and content of the conversation while cleaning up grammar and removing unnecessary repetitions. It's useful when the primary goal is to understand the content rather than analyze speech patterns.
This specialized type uses phonetic symbols to represent the sounds of speech. It's primarily used in linguistic research and is less common in UX research contexts.
What type of transcription is used in qualitative research?
In qualitative research, intelligent verbatim transcription is often the preferred choice . This type of transcription strikes a balance between capturing the essence of the conversation and maintaining readability. It preserves the interviewee's words and intent while removing unnecessary filler words and false starts that can distract from the main content.
This type of transcription in qualitative research makes it easier to identify key themes, pain points, and user needs that can inform design decisions.
What type of transcription is used in thematic analysis?
Thematic analysis , a common method used in qualitative research to identify patterns and themes within data, typically relies on intelligent verbatim transcription . It provides enough detail to capture the nuances of participants' responses while maintaining readability, making it ideal for identifying recurring themes and concepts.
What is the average price for transcription services?
The cost of transcription services for qualitative research can vary widely depending on factors such as turnaround time, audio quality, and the level of detail required. On average, professional qualitative transcription services may charge anywhere from $1 to $3 per audio minute for standard turnaround times (typically 3-5 business days).
For UX researchers working on time-sensitive projects, expedited services are available but often come at a premium, with prices potentially doubling or tripling.
It's worth noting that some of the best transcription services for qualitative research offer discounts for bulk orders or ongoing projects, which can be beneficial for researchers conducting multiple interviews or focus groups.
When considering the cost, it's important to weigh the value of professional qualitative research transcription services against the time and effort required to transcribe in-house. While DIY transcription might seem cost-effective, it can be time-consuming and may not yield the same level of accuracy as professional services.
How to write a transcript for qualitative research
Writing a transcript for qualitative research involves more than just typing out what you hear.
Here are some key steps to ensure your transcripts are accurate, useful, and ready for analysis:
Prepare your tools: Choose reliable transcription software for qualitative research or a word processing program. Ensure you have a good quality audio playback device and headphones for clear listening.
Listen to the entire recording: Before you start transcribing, listen to the entire recording to familiarize yourself with the content, speakers, and any potential audio issues.
Create a template: Set up a consistent format for your transcripts, including headers for participant information, date, time, and any other relevant details.
Transcribe the content: Begin typing out the conversation, following the intelligent verbatim method unless your research requires a different approach. Include speaker labels to differentiate between the interviewer and participant(s).
Add time stamps: Regularly insert timestamps throughout the transcript. This helps in referencing specific parts of the conversation later and syncing the transcript with the original audio if needed.
Note non-verbal cues: When relevant, include descriptions of significant non-verbal communication or environmental factors in square brackets, e.g., [laughs], [long pause], [background noise].
Review and edit: Once you've completed the initial transcription, review it while listening to the audio again. Correct any errors and ensure the transcript accurately represents the conversation.
Format for readability: Use paragraphs to separate distinct topics or questions. While it's best to keep bullet points and lists to a minimum, you can use them sparingly to highlight key points if necessary.
How do you transcribe audio data in qualitative research?
Transcribing audio data in qualitative research is a process that requires careful consideration of several factors.
What are the aims of the research project?
Before you begin transcribing, it's crucial to clearly understand the goals of your research project . Are you looking to gather specific user feedback on a product feature? Or are you conducting a broader study on user behavior and preferences? The aims of your project will influence the level of detail and focus required in your transcriptions.
For example, if you're researching user reactions to a new app interface, you might pay special attention to comments about the layout, navigation, and visual elements. On the other hand, if you're exploring user motivations and decision-making processes, you might focus more on capturing the reasoning and emotions behind their responses.
What level of detail is required?
The level of detail in your transcriptions should align with your research goals and analysis methods. For most UX research projects, intelligent verbatim transcription provides an ideal balance of detail and readability. However, there may be instances where more or less detail is necessary.
If you're conducting a usability test and need to capture specific user actions along with their verbal feedback, you might include more detailed notes about their interactions with the product. Conversely, if you're more interested in high-level themes and general user sentiment, a slightly less detailed transcription might suffice.
Who should do the transcribing?
Deciding who should handle the transcription is an important consideration. You have several options:
DIY transcription: As the researcher, you might choose to transcribe the audio yourself. This can be time-consuming but allows you to immerse yourself in the data and potentially identify themes early on.
Team member transcription: Assigning transcription tasks to other team members can distribute the workload and provide multiple perspectives on the data.
Professional transcription services: Opting for qualitative research transcription services can save time and ensure high-quality, accurate transcripts. Many services specialize in research transcription and understand the specific needs of qualitative researchers.
Transcription software: Using qualitative research transcription software can speed up the process, especially for clear audio recordings. However, it's important to review and edit machine-generated transcripts for accuracy.
What contextual detail is necessary to interpret data?
Context is crucial in qualitative research, and your transcripts should include relevant contextual details that aid in interpreting the data. This might include:
Background information about the participant (e.g., age range, profession, relevant experience)
The setting of the interview or focus group
Any visual aids or prototypes used during the session
Significant non-verbal cues or reactions
How should data be represented?
When it comes to representing data in your transcripts, clarity and consistency are key. Use a clear, consistent format for speaker labels (e.g., "Interviewer:", "Participant 1:"). Include time stamps at regular intervals or at the beginning of new topics. Consider using bold or italics to highlight key quotes or themes, but use this sparingly to maintain readability.
What is an example of a transcription?
Here’s an example of what an AI-generated transcript looks like, with time-stamps and Speaker labels. The transcript also features text highlighted in green for positive responses, and blue for questions.
Best Automated Transcription Services for Qualitative Research
When conducting qualitative research, choosing the right transcription service is crucial for efficient data analysis. Here's a comparison of some popular transcription tools used in qualitative research:
NVivo is primarily a qualitative data analysis tool that offers transcription services as part of its feature set.
Price: NVivo's pricing is on the higher end, with users required to purchase blocks of transcription time (e.g., €80 for 10 hours).
NVivo allows uploading of various audio and video file formats to its online platform.
Allows you to edit and make changes, tag speakers, and ensure proper formatting
Offers encrypted and secure storage, adhering to HIPAA standards and GDPR compliance
Languages Supported: NVivo supports transcription in 42 languages.
Time taken: Specific time is not mentioned, but it's noted to be generally slower compared to other tools.
Accuracy: NVivo's transcription accuracy is lower compared to competitors, especially in noisy environments and with accents.
How much does NVivo transcription cost?
NVivo transcription costs around €80 for 10 hours of transcription time. The pricing structure is based on purchasing blocks of time rather than a subscription model.
Is NVivo transcription free?
No, NVivo transcription is not free. It requires purchasing transcription time.
Is NVivo good at transcription?
NVivo's transcription capabilities are considered less accurate compared to some competitors, especially in challenging audio conditions or with accented speech.
Is NVivo used for qualitative research?
Yes, NVivo is widely used for qualitative research, primarily as a data analysis tool. Its transcription feature is an additional service within this broader qualitative research platform.
Dovetail is a comprehensive research repository that includes transcription, coding, and data analysis features.
Price: Dovetail offers a free plan with 1 project per month, while paid plans start at $29 per user per month.
Does automated transcription of video and audio recordings
Does sentiment analysis of transcripts with highlights for positive and negative responses
Also offers built-in analysis tools for coding and tagging of transcripts
Languages Supported: Supports 41 languages, including Japanese, Finnish, Hindi, and Malay.
Time taken: Transcription is completed within minutes.
Accuracy: While generally considered accurate, specific accuracy metrics are not provided.
Looppanel is an AI-powered research repository tool that can do extremely accurate interview transcription for UX research, among other cool features. It’s special compared to other transcription services on this list, as it also lets you record your calls directly, and receive high-quality transcripts within mere minutes.
Price: Paid plans start at $30 per month, with a 15-day free trial available.
Features:
Collaboratively take notes with colleagues during your user interviews
Save key time-stamps of important quotes as they come up
Sentiment analysis of transcripts with highlights for questions, positive and negative responses
Generate AI-powered notes from your transcript for you, with a dedicated analysis space where you can see all your data by question or tags
Do Google-like search within your research repository to find any quote or data point you need, in minutes.
Languages Supported: Supports 8 languages, including English, Spanish, French, German, Italian, Portuguese, Dutch, and Hindi.
Time taken: Provides near-instant transcripts for recorded calls.
Accuracy: Looppanel boasts over 90% accuracy in transcription.
MAXQDA is a research analysis tool that’s more complex than the others, but is ideal for academics and scientists who need deep, detailed analysis. MAXQDA offers transcription services alongside qualitative analysis tools.
Price: Approximately $20 for 2 hours of transcription, with varying plans based on industry and use case.
MAXQDA offers a customizable dictionary for accuracy
Does automatic speaker detection, and timestamps.
It's GDPR-compliant
Doesn't require a subscription or MAXQDA license for transcription services.
Languages Supported: Supports over 48 languages.
Time taken: Transcription is completed within minutes.
Accuracy: Claims over 90% accuracy
Otter.ai is a transcription tool that doesn’t offer any in-app analysis features, unlike the other tools on this list.
Price: Offers a free tier with 300 minutes of transcription; paid plans start at $8.33 per month.
Features:
Otter.ai can record and transcribe meetings on various platforms in real-time, capture slides, and generate summaries
It also allows for YouTube video transcription
Exports to various file formats.
Languages Supported: Only English
Time taken: Within minutes
Accuracy: Generally high accuracy, especially in structured meeting environments.
Challenges in transcription
Transcription in qualitative research can face several challenges:
Audio quality issues
Multiple speakers or overlapping speech
Accents or dialects
Background noise
Jargon or specialized terminology
Time-consuming nature of manual transcription
Maintaining consistency across multiple transcripts
Best Practices for Transcription in Action
How to do it:
Use high-quality recording equipment
Conduct interviews in quiet environments when possible
Consider using a foot pedal for manual transcription to improve efficiency
Use transcription software or services for larger projects
What to include:
Speaker identification, time stamps, non-verbal cues (laughter, pauses, sighs), contextual information and consistent formatting
How to record for optimal use in your study:
Test your recording equipment before the interview
Use external microphones for better audio quality
Inform participants about the recording
Take brief notes during the interview to supplement the recording
Back up your recordings immediately after the interview
What is the difference between transcription and translation in qualitative research?
Transcription involves converting spoken language into written text in the same language, while translation involves converting text from one language to another. In qualitative research, transcription is typically done first, followed by translation if the research is conducted in a language different from the one used for analysis.
What are the different types of transcription process?
The main types of transcription processes are:
1. Verbatim transcription (including all utterances and sounds) 2. Intelligent verbatim (removing fillers and false starts) 3. Edited transcription (cleaning up grammar and removing repetitions) 4. Phonetic transcription (using phonetic symbols to represent sounds)
What transcription services for qualitative data?
Transcription services for qualitative data include automated tools like NVivo, Dovetail, Looppanel, MAXQDA, and Otter.ai, as well as human transcription services. The choice depends on factors such as budget, accuracy requirements, and the complexity of the audio data.
Can I use NVivo for transcription?
Yes, you can use NVivo for transcription. However, it's important to note that while NVivo offers transcription services, it may not be as accurate or cost-effective as some alternatives, especially for large-scale projects or challenging audio conditions.
What is the alternative to NVivo transcription?
Alternatives to NVivo transcription include Dovetail, Looppanel, MAXQDA, and Otter.ai, each offering different features and pricing structures.
Is NVivo transcription worth it?
The value of NVivo transcription depends on your specific needs. While it integrates well with NVivo's analysis tools, its lower accuracy and higher price point may make it less appealing for some researchers.
Follow us on
Get the best resources for ux research, in your inbox, related articles.
Resources & Guides
How to Transcribe Interviews for UX Research
Best Transcription Services for Market Research
June 8, 2023
The Best Transcription Services for User Research
Looppanel automatically records your calls, transcribes them, and centralizes all your research data in one place
6 Transcription Software For Qualitative Research
Unlock efficiency in research: Discover the top transcription tools that save time, enhance accuracy, and boost productivity.
Ever tried to take meeting notes while someone’s speaking? Difficult to capture everything , isn’t it?
Enter transcription software for qualitative research .
This software generates transcripts for meetings, interviews and lectures. (We sure wish we had this tech in college!)
Suddenly, researchers can dive deeper into their work, analyzing more data. Using transcription audio software increases their productivity.
It doesn’t benefit researchers alone. Automated transcription has a host of applications across industries. UX researchers, Academics, Legal professionals, Journalists and Designers can all leverage this technology.
No more spending hours on end, trying to capture exactly what someone said.
“Look Ma, no hands!”
TL;DR – Top 6 Transcription Software For Qualitative Research
Save time and effort with transcription software. In this article, let’s explore the best software for transcription. We’ll go over the pros and cons of using each of these transcription tools.
Here are six of the best software for transcriptionists:
Fireflies.ai
Did you know?
Marvin transcribes your audio and video files in just minutes. Don’t believe us? Take it for a test drive .
What is Transcription Software?
In a nutshell, transcription software converts speech from audio into editable text.
Now let’s get technical. Transcription apps use Machine Learning (ML) to analyze an audio or video file. Algorithms trained on vast datasets evaluate audio input, breaking it down into smaller segments.
Speech recognition engines analyze segments and identify phonemes (smallest sound units). Neural networks handle sequential data, processing speech into a transcript. Natural Language Processing (NLP) deciphers the structure and meaning of transcribed text.
These layers of technology work in tandem to produce a coherent transcript.
There are several benefits of using transcription software:
Time Savings. Manual transcription is time consuming. Professional transcriptionists take four hours to transcribe an hour-long recording. Transcription software’s turnaround time is only a few minutes. Real-time processing helps companies deal with larger volumes of audio data.
Accuracy. NLP and speech recognition systems capture words with high precision. Systems continuously learn from data you feed it. They continually adapt and produce higher quality transcripts.
Cost-effective. Transcription tooling has advanced, becoming more accessible than ever. Companies are cutting costs by exploring software alternatives to expensive, specialized services. Learn how Microsoft saves thousands of dollars using Marvin’s transcription.
Convenience. Applications nowadays are largely web-based, increasing their reach. Users can access the software anytime, anywhere. No longer are they restricted to one machine or location.
Flexibility. Apps are customizable and allow users to tailor software to their own needs. Add industry terminology, specialized words and phrases to the software. AI incorporates this data, training itself to transcribe these terms accurately in the future.
Accessibility. Transcription software is inclusive, catering to a wider audience. Make transcripts available to people who are deaf or hard of hearing.
Types of Transcription Software
Transcription can be further classified into three broad categories:
Automatic transcription. Uses AI and ML for transcribing audio and video files. Produces accurate (but not perfect) results. Transcripts usually require manual editing once created.
Professional transcription. Used by transcriptionists and professionals who regularly need to transcribe in their work.
Speech-to-text. Transcribes speech with reasonable accuracy in real-time. Provides a file in a text editor for correcting mistakes. Often used for transcribing live events such as conferences, lectures or meetings.
Key Features to Look For in Transcription Software
What will you use transcription software for? Who will use it the most? Consider your business requirements before beginning your search for the perfect tool. What functionality do you need?
Look out for a transcription tool that ticks all (or most) of these boxes. We’ve separated the list into the “must-haves” versus the “nice-to-haves”:
Accuracy. One of the most important factors. Does the application convert speech-to-text accurately? Software that uses ML recognizes speech patterns and identifies words with high precision.
Speed. Choose software that generates transcripts with a faster turnaround time. Save hours of time with transcripts readymade in minutes. Helpful for tight deadlines. Be careful of the speed vs. accuracy tradeoff – don’t sacrifice one for the other.
Compatibility. Does it integrate with other tools? Which applications are essential for your company? Which ones must the tool talk to? Export meeting notes to CRM and project management tools that you use regularly.
Cost. An important consideration. Tools usually offer free and paid versions. Look for tools that meet your requirements first. Establish a budget and zero in on the one that fits within it.
Data Security. Protect confidential user data. Ensure your tool adheres to local data privacy laws. Look for tools with compliance relevant to your industry. Learn more about the different types of data security compliance .
Nice-to-Haves
Language Support. Tools offer transcription services in multiple languages. Helpful for global businesses and communicating across geographies and cultures.
Speaker Identification. Uses speaker diarization technology . This helps distinguish between speakers and labels them correctly in the transcript.
Customization. Tools offer several customization options including Timestamp Generation and Vocabulary Lists . Timestamps make it easy to navigate through a script or recording. Extracte and share quotes with ease. Add industry terms to the vocabulary list to improve its data capture in the future.
User-Friendliness. Choose an application that’s easy to learn. A clean user interface for smooth navigation helps, too! The ability to edit transcripts in-house makes the transcription process more efficient.
Flexibility. Most tools allow you to login remotely. This makes them easily accessible to stakeholders from anywhere.
Additional Features. Some tools go beyond transcription. Equipped with audio intelligence, applications understand and analyze audio files. They’re capable of producing summaries and insights from the data.
Transcription software plays a crucial role in qualitative research, saving researchers time and effort while enhancing data accuracy.
(In case you haven’t noticed, we’re all about freeing up your time. Hop over here to see how AI makes qualitative research powerful .)
By choosing the right tool, researchers can focus on what matters most — discovering valuable insights. Here are six top transcription software options to consider:
A leading light in the universe of transcription software.
Invite Marvin to your meetings or interviews and concentrate fully on participants. Receive a highly accurate and editable transcript in minutes. Collaborative note-taking allows multiple users to add key insights as interviews roll on.
Marvin uses industry-leading AI features. Speaker identification allows you to navigate through a transcript easily. AI generates summaries of transcripts and creates time-stamped insights. A useful starting point from which to begin analysis.
AskAI allows users to interrogate their data across multiple projects. Enter questions in a google-esque search bar, and sit back. AI evaluates your data, producing high quality responses and insights.
Create clips and stitch them together into playlists. Share these with stakeholders to elevate the user voice across the organization.
Marvin integrations connect to tools people rely on. Sync seamlessly with video conferencing apps (Zoom, Google Meet and Microsoft Teams).
A research repository that houses and safeguards all user data. We are GDPR, SOC2 and HIPAA compliant. Anonymize transcripts and blur faces in clips. Your user data stays protected.
With support in over 40 languages, a user-centric transcription software for effortless research collaboration. It’s entirely web-based, so users can access their repository from anywhere at any time.
High Accuracy Transcription
Quick turnaround time
Advanced AI features
Powerful integrations
Robust Data Security
Accepts multiple file formats
Supports over 40 languages
Selective quantitative analysis capabilities
2. Descript
Calling all content creators.
Descript is best suited for audio and video editing. Write, record, transcribe and edit files all on one platform.
Advanced editing features allow you to create powerful soundbites and clips quickly. Cut portions out of the transcript and the app automatically removes them from the clip. AI features help remove background noises and echoes from clips. Overdub your voice to add context to recordings.
The inbuilt video clip maker readies files for social media sharing. Its multicam capability also captures the speaker in video files. Descript is a great solution for editing files, best for content creators who need to edit on the fly. However, it’s more of an editing tool with transcription as a feature .
Video and audio editing capabilities
User-friendly Interface
Lower accuracy compared to other tools
Limited AI capabilities
Mainly a video editing tool
Not designed for qualitative research
3. Fireflies.ai
An AI-powered meeting transcription software. Fireflies uses voice recognition technology to generate actionable transcripts. Their meeting assistant creates action and follow-up items from transcripts. Track quality of conversations with conversational intelligence.
On Fireflies, users can record clips and capture data with live transcription. Edit and highlight your transcript and add comments. Its advanced search functionality allows users to scan text for keywords and themes.
Fireflies integrates with popular video conferencing platforms such as Zoom, Meet and Teams. Additionally, it syncs with CRM and project management tools
Create sound bites or clips
Edit Transcripts — add comments or annotations
Advanced search and filtering options
Chrome browser extension
Free plan has strict usage restrictions
Limited transcription outside meetings
4. Otter.ai
A mobile transcription app that helps generate notes for meetings and interviews. Use its dictation feature to capture what people are saying in real time. Or upload pre-recorded files onto the platform for post-meeting transcription.
Otter allows you to record, organize and save voice notes and files in one place (much like Marvin!). Collaborate with teammates — add comments and highlights to transcripts. Otter has a generous free plan best suited for people who transcribe a few files regularly (without large data volumes).
Produces high audio quality recordings
Collaborative workspace
Searchable by keyword
Mobile application for remote use
Free version works great for small teams
Lower accuracy %
Only supports English
Struggles with accents
Limited integrations
No cross-referencing data across projects
No speaker identification
Unintuitive UI
A popular tool that produces accurate transcripts quickly. Rev offers both human and AI-generated transcription, which costs significantly less. Some companies opt for human transcription for highly sensitive or important data.
Rev has robust editing features. These include creating highlights, adding comments and notes, and enabling read along tracking. It also offers a mobile application from which you can record and upload interviews. While that’s helpful, its interface is a bit clunky and doesn’t sync seamlessly with the platform.
Quick turnaround
Additional features – transcripts, captions and subtitles
Speech to text APIs for greater functionality
User-friendly web interface
Best of both — automated & manual transcription
Limited AI features
Can’t edit comments
Clunky mobile app
Sonix not only automates transcription, it translates speech as well. The platform creates subtitles for different languages, ideal for multilingual video clips. Predictably, it offers multi-language support for these handy features.
Transcription in Sonix has an impressive accuracy rate. It auto-punctuates text and offers timestamps for easy navigation through a transcript. Auto speaker separation helps identify different speakers.
Sonix boasts a host of helpful integrations. To protect user data, it offers “bank-level” security (their words). Fast, accurate and secure, Sonix is a tool suited best to people who deal with multiple languages regularly.
High accuracy
Multi-language support
Embed subtitles and captions in videos
SOC2 compliant
Costly – subscription and per hour fees
User Experience is not up to scratch
Steep learning curve
Best Practices for Using Transcription Software in Research
Ensuring a file has high audio quality helps transcription software capture speech accurately. Use these tips and tricks to get the most out of your transcription software:
During Recording
Minimize Background Noise. Keep your recording environment noise-free. Cut out ambient sounds and echoes. This helps the software accurately capture phrases and words.
Take Turns to Speak. Software might have a tough time if you alternate between speakers too quickly. Don’t have multiple people speaking at the same time — mute everyone who isn’t speaking. Avoid crosstalk.
Setup Microphone Correctly. Ensure the mic is fully functional and of decent quality. Place it close to the speaker(s) — ideally not more than 2 meters away.
Speak Clearly. Interpreting unclear speech is difficult. To all the mumblers out there ( this author included ): Enunciate! Slowly…
Post Recording
Review Transcripts. Proofread system-generated transcripts. Edit any text that the software might’ve missed or transcribed incorrectly. Ensure the transcript captures the audio correctly.
Personalize Vocabulary. Add industry jargon and abbreviations to the software library. Apps learn from this data so they capture data accurately moving forward. Add context with comments to provide more insight.
Ensure Data Security. Last but not least — make sure to protect and encrypt confidential user data. Anonymize user data before storing files.
Frequently Asked Questions (FAQs)
Below we address some frequently asked questions about transcription software:
Is Automated Transcription as Accurate as Manual Transcription?
Manual transcription is more accurate than automated transcription. Transcriptionists spend copious amounts of time poring over every detail. They produce a highly accurate transcript, complete with punctuation, industry terms, etc. However, the turnaround time and costs associated with manual transcription are high.
Automated transcription software uses advanced AI and NLP technology, generating largely accurate transcripts. These tools produce transcripts in minutes, at a fraction of the cost. Inevitably, transcription software will make errors that need correction.
In both cases, we recommend a human review the transcript. A final reviewer can identify mistakes and industry-specific terms.
As we continue to feed language models more data, their accuracy will only improve. A future where automated transcription replaces its manual counterpart isn’t far away.
Can Transcription Software Handle Different Accents and Languages?
Yes, some apps are better than others.
Human speech is nuanced. Accents and dialects might be difficult for the software to understand. This can lead to mistakes in transcription.
Businesses with a global presence deal with multiple different languages and cultures. We recommend using a transcription tool that supports different languages. One that’s trained on regional accents and dialects does a much better job of capturing speech correctly.
Choose a tool that offers language support for ones that you need.
Did you know?
Marvin supports over 40 languages and dialects.
How Does Automated Transcription Enhance the Qualitative Research Process?
Transcription software for qualitative research brings resource efficiency.
It enhances the qualitative research process in two ways:
Speed. Leveraging advanced AI, transcription software processes hours of audio in a fraction of the time. Manual, human transcriptionists take hours or days to transcribe audio.
Cost-Effectiveness. At a fraction of the cost of manual transcription, transcribe large amounts of audio data.
Overall, leveraging automated transcription saves precious resources — time and money. It brings efficiency to the research process. Transcription software frees up a researcher’s time for more analysis. The best transcription tools offer ways to clip insights and share knowledge across an organization.
Recording meeting minutes got a whole lot easier. Cut down the dreaded drudgery of research work with transcription audio software.
This software generates transcripts with astonishing speed and accuracy. Leveraging AI technology, it creates editable transcripts in minutes.
AI has permeated into the transcription industry. This has vast implications not only in UX, but Media and Entertainment, Legal, Medicine, Education and business in general.
It’s important to remember that the field of AI in UX research is at an early stage of its development. It’ll only get better with time. In the future, expect high customization, real-time transcription and industry and geography-specific support.
Implementing transcription software into your workflow is a no-brainer. Especially when you consider manual transcription as the alternative.
Choosing a transcription tool isn’t easy. Try before you buy. Note that many use similar technologies to transcribe files. Evaluate apps on additional features that are helpful to you. You need an application that not only transcribes audio, but houses all your user data. Securely.
One that makes it easily searchable and accessible. And makes insights shareable. What are you waiting for? Put Marvin’s transcription to the test. Set up your free demo today.
Categories:
Leading the Way
Marvin Customers
Marvin Events
Talk to Your Users
Krish Arora
Latest posts
Krish Arora leverages his experience as a finance professional to turn data into insights. A passionate writer with a strong appreciation for language, Krish crafts compelling stories with numbers and words to elevate the practice of user research.
Your Complete Guide to Product Management Customer Feedback
(6 Top Picks) Survey Analysis Software - Complete Guide
(Top 8) Best Qualitative Data Analysis Software
withemes on instagram
Open access
Published: 16 August 2024
Providers’ knowledge and perception of xylazine in the unregulated drug supply: a sequential explanatory mixed-methods study
Xylazine is increasingly prevalent in the unregulated opioid supply in the United States. Exposure to this adulterant can lead to significant harm, including prolonged sedation and necrotic wounds. In the absence of literature describing healthcare providers’ experiences with treating patients who have been exposed to xylazine, we aimed to explore what gaps must be addressed to improve healthcare education and best practices.
From October 2023 to February 2024, we conducted a sequential explanatory mixed-methods study, with (1) a quantitative survey phase utilizing convenience sampling of healthcare providers treating patients in Connecticut and (2) a qualitative semi-structured interview phase utilizing purposive sampling of providers with experience treating patients with xylazine exposure. Summary statistics from the survey were tabulated; interview transcripts were analyzed using thematic analysis.
Seventy-eight eligible healthcare providers participated in our survey. Most participants had heard of xylazine (n = 69, 95.8%) and had some knowledge about this adulterant; however, fewer reported seeing one or more patients exposed to xylazine (n = 46, 59.8%). After sampling from this subgroup, we conducted fifteen in-depth interviews. This qualitative phase revealed five themes: (1) while xylazine is novel and of concern, this is not necessarily exceptional (i.e., there are other emerging issues for patients who use drugs); (2) participants perceived that xylazine was increasingly prevalent in the drug supply, even if they were not necessarily seeing more patients with xylazine-related outcomes (XROs); (3) patients primarily presented with non-XROs, making it difficult to know when conversations about xylazine were appropriate; (4) patients with XROs may experience issues accessing healthcare; (5) providers and their patients are learning together about how to minimize XROs and reduce the sense of helplessness in the face of a novel adulterant.
Conclusions
Xylazine-specific education for healthcare providers is currently insufficient. Improving this education, as well as resources (e.g., drug checking technologies) and data (e.g., research on prevention and treatment of XROs), is crucial to improve care for patients who use drugs.
Across the United States (US), the overdose crisis continues to contribute substantially to premature morbidity and mortality. To exacerbate this crisis, xylazine, a veterinary tranquilizer not approved for use in humans, has emerged as a novel adulterant in the unregulated drug supply and is found almost exclusively in fentanyl [ 1 , 2 , 3 , 4 , 5 , 6 , 7 ]. As an α-2 adrenergic receptor agonist, xylazine’s toxidrome can lead to many serious medical complications, including prolonged sedation, severe hypotension, decreased heart rate, and respiratory depression [ 2 , 4 , 8 , 9 , 10 ]. Further, exposure to xylazine can induce large necrotic wounds that are difficult to manage for people who use drugs (PWUD) and healthcare providers alike [ 9 , 11 , 12 , 13 , 14 ]. In response, the Office of National Drug Control Policy declared xylazine-contaminated fentanyl an emerging threat to the US in April 2023 [ 15 ].
Xylazine was first recognized as an adulterant in the unregulated drug supply in the early 2000’s in Puerto Rico [ 4 , 8 , 16 , 17 ]. After falling off the radar for nearly two decades, xylazine again emerged in post-mortem toxicology and drug seizure data in the Northeastern US before spreading south- and westward [ 1 , 18 , 19 ]. In Connecticut specifically, xylazine is exclusively found in combination with fentanyl in overdose mortality data [ 20 ]. 2019 marked the first year with more than one reported xylazine and fentanyl combination overdose death (n = 71) in Connecticut [ 20 , 21 ]. This number has been on the rise; in 2022 alone, almost 25% of overdose deaths involved a combination of xylazine and fentanyl (n = 353) [ 20 ].
Given the recent emergence and rise of xylazine prevalence in the drug supply in Connecticut, little information about how to mitigate harms from xylazine exposure is readily available for PWUD and providers [ 9 , 21 ]. Funded through the Medical Staff Fund at Yale New Haven Hospital, this study was designed to explore Connecticut-based healthcare providers’ knowledge and perceptions of xylazine exposure to determine key gaps in education for providers and inform medical best practices as they relate to xylazine exposure and associated complications among patients who use drugs. This information was collected to inform the development of targeted medical education for providers about xylazine and the impacts of xylazine exposure.
Recruitment procedures, study sample, and human subjects protections
This sequential explanatory mixed-methods study of Connecticut-based healthcare providers was conducted in two phases: a quantitative survey followed by qualitative interviews. Yale’s Institutional Review Board deemed this study exempt from human subjects review.
Convenience sampling was utilized to recruit a minimum target of 50 study participants for the quantitative phase. Healthcare providers (e.g., MD, DO, RN, etc.) practicing at hospitals, community healthcare centers, harm reduction organizations, and other care settings around Connecticut were informed of this study through medical listservs, word-of-mouth, and social media. All potential participants were provided with information about this study at the beginning of the survey and completion of the survey was accepted as consent to participate. No compensation was awarded for this quantitative phase.
Subsequently, purposive sampling was utilized to recruit participants for the qualitative phase based on select responses to the survey administered during the quantitative phase, including (a) interest in a follow-up interview, and (b) experience treating patients with confirmed or suspected xylazine exposure. Potential participants were contacted for follow-up over email to verify interest in and availability for the interview. We aimed to interview 15 participants during this phase, based on our previous work, with intent to establish the final sample size through discussion of thematic saturation. Prior to interviews, participants were provided an information sheet and consent form via email; these forms described the purpose and procedures of the study, their rights as participants, confidentiality measures, and potential risk. Participants had the option to have the documents verbally reviewed with them by a member of the study team and were given the opportunity to ask questions. Verbal consent to be interviewed and for recording the interview was obtained prior to beginning the qualitative phase and all participants were advised on their right to terminate participation at any time. Participants received a $30 electronic gift card for their time and expertise upon completion of the interview.
Instrument development and data collection
The quantitative phase of this study utilized REDCap (Research Electronic Data Capture, hosted at Yale University, Version 14.0.27) to facilitate a survey composed of 37 questions (Supplement 1 ). The survey included questions on (a) providers’ medical background, (b) experience treating patients with xylazine exposure, (c) a modified Harm Reduction Acceptability Scale, [ 22 ] (d) xylazine knowledge, (e) confidence in medical care for xylazine-related outcomes (XROs), (f) demographic information, and (g) interest in a follow-up interview. The survey was designed to take participants 10–15 min to complete. The qualitative phase comprised one-on-one semi-structured interviews, conducted over the teleconferencing software platform, Zoom, to best accommodate the participants’ schedules. The 10-question interview guide, designed to take approximately 30 min, covered (a) medical experience, (b) xylazine knowledge, (c) perception of xylazine, and (d) education on xylazine (Supplement 2 ).
Data analysis
For the quantitative phase, summary statistics were tabulated for key demographic information, xylazine knowledge and perception, and harm reduction acceptance. All quantitative data analysis was conducted using Microsoft Excel and R (R Core Team, Version 4.2.2,). For the qualitative phase, interview recordings were transcribed using Trint software and verified for accuracy by the first author (K.H.). Transcripts were entered into NVivo software (QSR International, Version 1.7.1) to facilitate thematic analysis [ 23 ]. A codebook with both inductive and deductive codes drawn from the interview guide and existing literature (i.e., “Patient Care Experiences” and “Lack of Supplies”) was developed by K.H.. Subsequently, the codebook was discussed among the full study team, improved iteratively, and applied to all transcripts. Themes were discussed with the study team. Pseudonyms for respondents were created for the qualitative analysis presented below to preserve participant confidentiality.
Survey participant characteristics
From October 5, 2023, to January 24, 2024, n = 83 people expressed interest and began the online survey. After screening, n = 78 respondents were eligible to participate. Table 1 provides the frequency and percentage of select characteristics of survey participants. The mean age of providers was 40.6 years (SD = 12.0), and most participants were White (n = 55, 70.5%) and non-Hispanic (n = 66, 94.3%). Seventy-eight percent of providers were medical doctors, with internal medicine (n = 37, 47.4%) and addiction medicine (n = 27, 34.6%) being the most represented specialties. The mean number of years of experience that providers had treating patients with substance use or substance use disorder was 8.2 (SD = 9.4). Based on a modified Harm Reduction Acceptability Scale, [ 22 ] most providers who answered these questions expressed favorable attitudes towards harm reduction (n = 70, 97.2%).
Findings from the quantitative phase
Table 2 provides the frequency and percentage of providers’ responses to key survey items.
Providers’ awareness and knowledge of xylazine and XROs
Most providers had previously heard of xylazine (n = 69, 95.8%) before taking the survey. The majority of respondents knew that (a) xylazine exposure could lead to severe necrotic wounds (n = 68, 94.4%), (b) xylazine is not FDA-approved for use in humans (n = 72, 100%), (c) naloxone cannot reverse a xylazine overdose (n = 69, 95.8%), and (d) xylazine is added to fentanyl to prolong the prolong the opioid/narcotic effect of the fentanyl (n = 67, 93.1%). A smaller proportion of providers believed that xylazine was not a central-acting opioid (n = 51, 71.8%) and that xylazine is almost exclusively found as an adulterant in fentanyl (n = 55, 76.5%).
Providers’ experience with patients exposed to xylazine
Over half (n = 46, 59.8%) of providers reported seeing one or more patients who have been exposed to xylazine, while 18 providers (23.4%) did not know how many patients they had seen with a known or expected xylazine exposure. Most providers (n = 43, 55.2%) sometimes or rarely had their patients discuss xylazine with them.
Providers’ confidence with care related to xylazine
Few providers reported feeling confident (n = 18, 25.4%) or extremely confident (n = 5, 7.0%) in recognizing XROs in their patients. Instead, most providers only felt some confidence in this ability (n = 27, 38.0%). When reporting confidence in their ability to treat patients with XROs, many providers indicated they had some (n = 22, 31.0%), little (n = 22, 31.0%), or no confidence (n = 12, 16.9%). However, for confidence in counseling patients on how to prevent XROs, more providers felt some confidence (n = 16, 22.5%), confident (n = 19, 26.8%), or extremely confident (n = 8, 11.3%) in their abilities.
Interview participant characteristics
From November 30, 2023, to February 9, 2024, trained members of the study team conducted one-on-one semi-structured interviews with providers via Zoom. After the a priori goal of n = 15 interviews was met, theoretical saturation was discussed by the study team and deemed to be sufficient (i.e., no new themes emerged over the course of the last few interviews conducted; additional interviews were not likely to reveal new themes). The average duration of the interviews was 24.7 min. Participant characteristics for the qualitative phase are detailed in Table 3 .
Findings from the qualitative phase
Theme 1: “the top of a mountain of sad data points”.
While all providers described the many ways xylazine is troublesome for PWUD, most participants asserted that this adulterant is accompanied by other troublesome issues for this patient population. Dr. Rivera, a physician in internal medicine at a federally qualified health center, stated that the potential for xylazine exposure among PWUD is “just an additional sad data point at the top of a mountain of sad data points that these folks have collected about their situation.” In this way, xylazine was non-uniquely unique; while a novel concern for the healthcare of PWUD, it was one more addition to the list of concerns that was already quite crowded. Ultimately, participants identified xylazine exposure as a distinctive harm for many reasons (e.g., necrotic wounds, marked sedation). Further, Dr. Ford, an addiction medicine physician at a community health center, explained:
“Well, [xylazine] is odd… it can cause these scary complications. It doesn't neatly fit into the opioid category… [Clinicians] like to ‘bucket’ things. There is sort of a fentanyl / heroin bucket. We know what to do about that. Xylazine is in its own bucket. It's hard to kind of conceptualize what it is and how best to combat it.”
Here, xylazine’s novelty can be largely attributed to healthcare providers not feeling as though they have experience with substances that have a similar mechanism of action (i.e., a ‘bucket’) currently being used for medical care or on the streets. Without this direct comparator in their metaphorical toolbox, many providers gauged xylazine’s impact on care by using fentanyl as a benchmark or point-of-reference.
Despite the unique mechanism and impact of xylazine as a street drug, providers often cautioned against xylazine exceptionalism, explaining that many issues are unique when it comes to treating the various needs of PWUD. Dr. Bennet, an infectious disease physician at an urban hospital system, stated:
“The opioid epidemic now has been just kind of crushing for ten years… When I was first a resident, it was pretty much just straight heroin. And then we got fentanyl. And then, occasionally, you'll see people who are skin popping, which has a kind of a similar effect in terms of the necrosis, though not as bad as xylazine. And now [xylazine] on top of it? It's just kind of grim. But I don't know if it really changes my attitude much from where it's been. It's been kind of grim for a while.”
Xylazine was described with this level of nuance by many providers—xylazine was perceived as one of many potential harms PWUD face daily.
Theme 2: “we see it every day whether we recognize it or not”
Many providers described a strong desire for access to rapid xylazine testing at the point-of-care (POC) to provide immediate results to patients. In the absence of sufficient POC testing, providers were left making educated guesses as to the magnitude of xylazine’s prevalence in the unregulated drug supply and, accordingly, the impact of this adulterant on their patient population. Dr. Campbell, an addiction and emergency medicine physician at a large academic medical center, stated “we see it every day whether we recognize it or not. [That’s] my strong suspicion based on what we see in our overdose death data.” In this way, many providers recognized that they do not diagnose, treat, or discuss XROs with a number of patients that is congruous with what might be suggested by overdose death data. For example, if approximately 25% of overdose deaths in Connecticut test positive for xylazine, providers might expect about a quarter of their patients to present with XROs, not just a few. Thus, without adequate POC testing, providers are left piecing together whether or not xylazine may be involved in their current patient cases. Dr. Roberts, an addiction medicine physician at a medically supervised withdrawal program, stated:
“The large, crater type wounds? Those we can definitely say are related to xylazine. The rest is often conjecture where somebody just appears to be having a much harder time… It's really only a suspicion. Unfortunately, at this stage, there's no reliable test that we have access to that will give us an answer. I understand there are some in development and I think there's one that's available, but it's a ‘send up’ test… 48 hours later, you get your answer. Which isn't really much help.”
Here, not only did Dr. Roberts believe that the lack of POC testing interfered with what they considered to be patient care best practices, but they also expressed frustration with the temporal delays in receiving information about xylazine exposure.
Even in the face of insufficient testing, most providers perceived that xylazine prevalence is growing in the unregulated drug supply—even if they had personally only seen one or two patients with certain XROs. Dr. Sullivan, an internal medicine physician working at an addiction medicine clinic, explained:
“I think that it's more widespread than we're giving it credit for. I've only seen a very small number of patients with ‘for sure’ complications of it. But I think that it is way more widespread than we know and that our patients know as well.”
Many providers shared Dr. Sullivan’s suspicion that xylazine was more prevalent than currently described. In this way, the available data sources for evaluating xylazine exposure among PWUD (e.g., overdose death data) are temporally delayed at best, but also potentially erroneous or misleading (e.g., counted deaths are just the tip of the iceberg).
Theme 3: “focus on what they are there for”
Participants also described their role in discussing xylazine’s potential harms with their patients. Some providers explained that the initiation of such a conversation was influenced by the reasons a patient sought care, noting that XROs were infrequently the primary reason PWUD sought care and that this can introduce challenges with starting a conversation. For instance, despite perceiving xylazine exposure to be widespread, Dr. Sullivan described how it is difficult to talk to patients about xylazine; they stated “when I bring [xylazine] up, [patients] just want to focus on what they are there for… We know there's cocaine and we know there's fentanyl. They address that rather than something that I can't test for.” Providers described feeling ill-equipped to discuss this novel adulterant—especially in the absence of proper tools to diagnose and treat xylazine exposure. Further, providers described how it was difficult to know when it was appropriate or necessary to discuss this novel adulterant with patients, particularly in the face of competing priorities. For instance, Dr. Rivera explained:
“If I have a patient that's coming in who has very severe heart failure, and they are clearly having an exacerbation right in front of me, and I need to send them to the emergency room? That's something that I have to address right away. And it's not helpful to them for me to also sort of screen them for xylazine exposure. And it's very rare for me to just have a visit where there aren't acute issues happening or something very serious that needs to be addressed that wouldn’t be more threatening to their life than their xylazine exposure, as hard as that might be to believe.”
Thus, despite the seriousness of potential xylazine exposure, PWUD often have more pressing health concerns that must be addressed during medical care. Due to this limitation, providers in high acuity settings may not always serve as the best primary point of education for PWUD on xylazine; in fact, some providers urged the importance of harm reduction organizations and word-of-mouth among networks of PWUD for this information dissemination.
However, some providers did report initiating xylazine-specific conversations with their patients when it was deemed relevant and important. Dr. Baker, an addiction and internal medicine physician employed at an addiction treatment clinic, explained one recent case in which they spurred conversation with a patient:
“We approached her about [her positive xylazine result] and just said, 'hey, I know that you're still using fentanyl and we're just trying to help to give you some extra ammunition for reasons to abstain. And here's one of them,' and we showed her some pictures, actually, on the internet of some of these xylazine associated wounds.”
Here, Dr. Baker utilized a positive screen on a send out test as a conversation starter to introduce xylazine and its related harms to a patient. While this was seen as an opportunity to educate the patient, Dr. Baker additionally considered xylazine to be a lever that could help motivate specific care goals. In this way, some providers perceived that the presence of xylazine in the drug supply might influence drug use behaviors (e.g., reducing drug intake) among specific patients. However, other providers perceived that the discussion of xylazine—in the absence of specific tools or robust information to provide patients—might reinforce stigma, induce fear, and be potentially harmful for patient care, as discussed below.
Theme 4: “afraid to go to the hospital”
Multiple providers lamented that XROs are likely to impact healthcare seeking, healthcare access, and the quality of care for patients who use drugs; further, some providers explained that these impacts may be exacerbated by preexisting stigma around drug use in many medical care settings. One way that xylazine was described to impact patient care was in the context of accessing medical care for wounds and fear around receiving poor management of their substance use disorder. Alex, a nurse practitioner at a behavioral health organization, described:
“Recently, I had a patient with xylazine wounds and abscesses. He was very sick, febrile, and needed to go to the hospital. He was coming into the clinic knowing that he was really sick and knowing he couldn't manage his wounds himself. But also, he was afraid to go to the hospital first because he didn't want to be sick and didn't want to not have that methadone in place before going. That was someone that we initiated on methadone and then sent immediately to the hospital for care.”
In this way, the provider explained how a patient seeking care for wounds might in turn be worried they would receive inadequate treatment for withdrawal symptoms. Here, while a patient may have previously been able to avoid care settings where their substance use was poorly managed, XROs—especially wounds—made it difficult for PWUD to avoid acute care or other medical settings where they may experience fear, stigma, shame, or other negative feelings around their drug use.
Additionally, many providers discussed that PWUD exposed to xylazine might not get proper follow-up for their XROs, largely depending on where they seek care. For instance, Dr. Bennet, who provides inpatient infectious disease consultations, described one patient case where this discontinuity in care was especially relevant:
“Unfortunately, [this patient] would come into the ER when she was very sick, get some antibiotics, and then usually leave the ER not too long after. But she had the worst scarring I'd ever seen. And it was really getting to the point where a good proportion of her upper and lower limbs are now all pretty fairly scarred… and unfortunately, I didn't get much of a chance to build a rapport with her because like I said, I saw her in the ER and by the time I came back the next morning, she was already gone.”
While this patient was accessing some level of care in the emergency department, Dr. Bennet describes that it was unclear whether or how this patient was managing her extensive xylazine-related wounds. Ultimately, numerous providers described a similar pattern wherein patients with XROs were leaving care settings without adequate care plans in place and/or against medical advice; however, the exact mechanism behind this is not yet fully understood (e.g., fear, stigma, pain, etc.). Additionally, in the quote above, Dr. Bennet explains that this abbreviated interaction with the patient also interfered with building a strong patient-provider relationship. In the context of drug use, and xylazine specifically, this building of “rapport” is crucial, as stigma and fear could interfere with their relationships with providers. For example, Dr. Blackwood, an infectious disease physician in an inpatient hospital setting, described a recent patient consultation in which they believed the patient was not being fully truthful about their drug use:
“[This patient] had very extensive wounds on the dorsal aspect of his hands that were kind of red and beefy and had a granulation tissue and raised border around them. He wasn't entirely straightforward about his drug use history but said that he had injected in the past. But not recently… He had tested positive for xylazine on the send-out test… But he was like, 'oh, [this wound] was an allergic reaction to a glove that I had. It wasn't related to any recent injection drug use.'”
In this case, having a pre-existing rapport might have eased the patient's fear and ameliorated stigma in ways that encouraged the patient to disclose their drug use behaviors to their provider.
Even if PWUD have an established care continuum and established rapport with their providers, it is still imperative to try to balance any existing power differentials. For instance, Dr. Baker—who used pictures of xylazine wounds to try to get their patient to abstain from fentanyl—further described that they believed:
“Stigma and shame associated with having these very grotesque wounds [might lead patients to] hide from their providers because they're ashamed of them… If a patient comes in and they're hiding things under their sleeves, so to speak, really make sure that you visualize – with patient consent – their arms and legs… And [my patient] that I was taking care of last summer with all these wounds? She was reporting severe pain all the time. You have to decide how much of that one wanted to believe… she looked quite comfortable.”
Thus, while providers can try to comprehend the impact stigma and shame have on their patients who use drugs, they must also be open to actively dismantling environments in which patients feel stigmatized and shamed. Without access to settings that meet people where they are, patients may delay seeking care. Such delays worsen outcomes that can include loss of limb function and amputation. Further, even once in care, PWUD may not feel comfortable disclosing information about their drug use, showing their wounds, or revealing their true pain levels—especially if they have previously been exposed to care settings where they are marginalized and systematically not believed.
Theme 5: “we are all learning together”
All of the participants, in some aspect, described how they did not always feel as though they had the information or tools necessary to provide high-quality care or counseling for patients with XROs or those at risk for xylazine exposure. As Dr. Rivera stated, “I think there's just a lot that [providers] don't know and, certainly, I think a lot that the folks that we take care of who use intravenous drugs don’t. We're all learning together.” Many other participants recognized that patients who use drugs might have more knowledge about this adulterant than they do as providers. This creates a learning opportunity for providers; while providers may have asymmetric information about current medical care best practices and proposed mechanisms of action, patients may have asymmetric information as well as it relates to street-based medicine and recognizing if xylazine is in their drug supply. Dr. Ford explained that:
“This is one of those examples in medical care where I think patients know more about it than we do. And so, whereas about maybe a year ago there were more like, 'Doc, what the heck is this?' types of conversations, now, oftentimes, I am learning from my patients about xylazine.”
Learning about novel adulterants like xylazine from patients who use drugs could inform best medical best practices over time and develop community-informed research questions. Providers might be encouraged to be open to this learning opportunity from patients, as Drs. Ford and Rivera were.
Without all of the knowledge and tools providers need and want, xylazine’s evolving medical landscape has created a sense of helplessness among providers. Many participants indicated that xylazine’s presence in the unregulated drug supply led to feelings of worry and fear both on (a) behalf of their patients and (b) for their own ability to provide care. Gabrielle, a nurse practitioner at a methadone clinic, stated that xylazine has “definitely changed the game of addiction… it's worrisome.” To mitigate such feelings of worry and to ensure quality care, providers not only looked to patients for closing information gaps, but also leaned on the specific expertise of other medical specialties to fill information or resource gaps in patient care. Dr. Thompson, an infectious disease and internal medicine physician, explained some of the resources available at their healthcare setting:
“We have excellent plastic surgeons who have been really good partners in kind of debriding the wounds as needed. And then if there is a wound, in addition to a general infectious disease follow up, we have a wound care center. And the nursing staff there is really meticulous. And there's a plastic surgeon in that clinic, there's a nurse practitioner who specializes in wound care. And then, of course, we have addiction medicine, so we really do have wraparound services to manage that.”
Here, the participant was able to utilize referrals and collaboration with a multidisciplinary team to ensure the best treatment for their patients with xylazine exposure. Ultimately, many providers described how having multiple specialties and areas of expertise involved in patient care reduced their feelings of helplessness and worry.
Our mixed-methods study to explore healthcare providers’ knowledge and perception of xylazine in the unregulated drug supply highlighted the need for targeted research and purposeful information dissemination to fill crucial gaps as they relate to xylazine exposure among PWUD. The quantitative phase revealed that although our sample of Connecticut-based healthcare providers had some baseline knowledge on xylazine, this knowledge did not necessarily translate into confidence in recognizing, treating, or counseling patients with XROs. The qualitative phase of our study, focusing on providers who perceived they had pre-existing knowledgeable and experience with xylazine and XROs, elucidated the possible mechanisms behind this, as providers highlighted the need for (a) continuing medical education on xylazine and XROs, (b) improved resources for managing XROs, such as more rapid xylazine testing at the POC and (c) access to quality data and research on the prevalence of xylazine in the local drug supply, and (d) information of the best evidence-based practices for treating XROs. Our study also found that healthcare providers who serve PWUD are not solely or uniquely concerned with xylazine, as other pressing health issues and even other adulterants are also of growing concern.
This study highlighted key areas where further medical education is needed, even among providers with high acceptability of harm reduction principles and general familiarity with xylazine as an adulterant. For instance, while providers noted that they felt xylazine was unique in terms of its mechanism of action and they did not have experience with similar substances, medical education could point to similar α-2 agonists they likely have experience with medically, such as clonidine [ 24 ]. However, not only did providers point to a need for more information about xylazine’s mechanism of action and impacts on health for themselves and their patients, they also called for improved data sources and research for understanding xylazine in the context of their patient population. Unfortunately, providers are currently left relying on delayed or biased data sources (e.g., overdose death data, drug seizure data) to establish the prevalence of xylazine and its potential for exposure in their patient populations [ 18 , 25 , 26 ]. To overcome this, one potential solution would be to improve funding for community-based drug checking programs that would provide more rapid and accurate results for patients.
It is important to elucidate if, and how, xylazine impacts perceived and experienced stigma among PWUD. While there are numerous ways drug use and bodily markings related to drug use have been shown to contribute to stigma among PWUD, it is crucial to understand how XROs—especially wounds—may novelly impact patient care and healthcare seeking among PWUD [ 27 , 28 , 29 , 30 ]. In lieu of specific research aimed at understanding XRO-associated stigma, providers should continuously strive to create safe environments for their patients who use drugs. This is especially critical given that PWUD may wait until their condition becomes serious before seeking medical care [ 29 , 31 , 32 ]. For instance, patients with necrotic wounds may have waited a significant period of time before presenting for care; while it is still unclear how painful xylazine wounds are at the various stages of development and healing, providers should heed caution and make every effort to ensure patients are able to access a continuity of care.
On a more positive note, we found that providers reported working with PWUD to build knowledge and practice bases to address xylazine and XROs. Certainly, this finding is likely influenced by our sample of providers who were mostly harm reduction-oriented; regardless, future efforts to build knowledge around xylazine and XROs should be collaborative with opportunities for information exchange with a wide range of providers and community members. For instance, people with lived experience should be incorporated into—and compensated for—medical training for providers who serve PWUD. Additionally, providers could explore how existing social networks of PWUD might be harnessed to encourage information dissemination about XROs and prevention of unwanted xylazine exposure.
Ultimately, without addressing these key information and practice gaps, providers may continue to feel fear, worry, and helplessness when it comes to serving patients with XROs. Funding training programs for medical providers and others who serve PWUD with XROs (e.g., harm reduction outreach workers) could serve as a key intervention for improving patient care and limiting the harms caused by xylazine in the unregulated drug supply.
Limitations
While our study fills a research gap and responds to the urgent need for more research on xylazine, some limitations should be mentioned. First, our study was not designed to be representative of all healthcare providers and should not be interpreted this way; instead, our goal was to examine a diversity of provider experiences, not make population-level generalizations. For instance, those with some baseline knowledge of xylazine were more likely to self-select for participation (i.e., most providers in our sample had previously heard of xylazine). It is very likely that providers in geographic regions with a lower prevalence of xylazine in the drug supply and specialties not represented here may be unaware of xylazine and its impact. However, our study shows that even amongst those with some xylazine knowledge, providers still lack confidence and knowledge in certain areas of patient care related to xylazine.
Further, most providers we surveyed and subsequently interviewed expressed attitudes favorable towards harm reduction (as opposed to abstinence-focused approaches); this almost certainly influenced how providers perceived xylazine and measures to address XROs. Accordingly, providers without such attitudes would likely perceive of xylazine and XROs differently. It is worth exploring in future studies how providers with an abstinence-focused mindset, and those simply unfamiliar with the philosophy and practice of harm reduction, might perceive of xylazine in the unregulated supply.
Additionally, our study utilized self-reported information about xylazine knowledge and perceptions, so resulting information may be misclassified if participants experienced poor recall or other errors. Lastly, due to the cross-sectional and provider-focused nature of our study design, we cannot make any temporal conclusions (e.g., about how certain areas of provider knowledge impacts patient outcomes, etc.).
There are key knowledge and practice gaps related to xylazine for healthcare providers, even if they have experience serving PWUD who have been exposed to this adulterant. Future research should focus on mechanisms to improve care for PWUD, including informing harm reduction and medical care best practices to limit the harms associated with xylazine exposure (i.e., prolonged sedation, overdose, wounds). Additionally, policy and funding should support evidence-based harm reduction strategies that can mitigate XROs (e.g., wound care supply provision, etc.). Without filling such research gaps and providing PWUD access to harm reduction resources, providers will likely continue to feel powerless in the face of this pressing health issue.
Availability of data and materials
The datasets generated and/or analyzed during the current study are not publicly available to protect participant privacy and confidentiality.
Kariisa M, O’Donnell J, Kumar S, Mattson CL, Goldberger BA. Illicitly manufactured fentanyl-involved overdose deaths with detected xylazine—United States, January 2019–June 2022. MMWR Morb Mortal Wkly Rep. 2023;72(26):721–7. https://doi.org/10.15585/mmwr.mm7226a4 .
Article CAS PubMed PubMed Central Google Scholar
Kacinko SL, Mohr ALA, Logan BK, Barbieri EJ. Xylazine: pharmacology review and prevalence and drug combinations in forensic toxicology casework. J Anal Toxicol. 2022;46(8):911–7. https://doi.org/10.1093/jat/bkac049 .
Article CAS PubMed Google Scholar
Ayub S, Parnia S, Poddar K, et al. Xylazine in the opioid epidemic: a systematic review of case reports and clinical implications. Cureus. 2023. https://doi.org/10.7759/cureus.36864 .
Article PubMed PubMed Central Google Scholar
Alexander RS, Canver BR, Sue KL, Morford KL. Xylazine and overdoses: trends, concerns, and recommendations. Am J Public Health. 2022;112(8):1212–6. https://doi.org/10.2105/AJPH.2022.306881 .
Gardner EA, McGrath SA, Dowling D, Bai D. The opioid crisis: prevalence and markets of opioids. Forensic Sci Rev. 2022;34(1):43–70.
CAS PubMed Google Scholar
Wide-Ranging Online Data for Epidemiologic Research (WONDER) . CDC, National Center for Health Statistics; 2021. http://wonder.cdc.gov
Ciccarone D. The triple wave epidemic: Supply and demand drivers of the US opioid overdose crisis. Int J Drug Policy. 2019;71:183–8. https://doi.org/10.1016/j.drugpo.2019.01.010 .
Ruiz-Colón K, Chavez-Arias C, Díaz-Alcalá JE, Martínez MA. Xylazine intoxication in humans and its importance as an emerging adulterant in abused drugs: a comprehensive review of the literature. Forensic Sci Int. 2014;240:1–8. https://doi.org/10.1016/j.forsciint.2014.03.015 .
Sue KL, Hawk K. Clinical considerations for the management of xylazine overdoses and xylazine-related wounds. Addiction. 2023. https://doi.org/10.1111/add.16388 .
Dowton A, Doernberg M, Heiman E, et al. Recognition and treatment of wounds in persons using xylazine: a case report from New Haven, Connecticut. J Addict Med. 2023. https://doi.org/10.1097/ADM.0000000000001198 .
O’Malley PA. Rising xylazine drug abuse in humans: a deep and lingering high with wounds, amputations, and death. Clin Nurse Spec. 2023;37(4):164–5. https://doi.org/10.1097/NUR.0000000000000758 .
Pennsylvania Department of Health. Xylazine and Wound Care for Healthcare Providers. 2023. https://www.health.pa.gov/topics/Documents/Opioids/Xylazine%20Provider%20Info.pdf
McFadden R, Wallace-Keeshen S, Petrillo Straub K, et al. Xylazine-associated wounds: clinical experience from a low-barrier wound care clinic in Philadelphia. J Addict Med. 2023. https://doi.org/10.1097/ADM.0000000000001245 .
Gupta R. Biden-Harris Administration Designates Fentanyl Combined with Xylazine as an Emerging Threat to the United States. 2023. https://www.whitehouse.gov/ondcp/briefing-room/2023/04/12/biden-harris-administration-designates-fentanyl-combined-with-xylazine-as-an-emerging-threat-to-the-united-states/
Torruella RA. Xylazine (veterinary sedative) use in Puerto Rico. Subst Abuse Treat Prev Policy. 2011;6(1):7. https://doi.org/10.1186/1747-597X-6-7 .
Reyes JC, Negrón JL, Colón HM, et al. The emerging of xylazine as a new drug of abuse and its health consequences among drug users in Puerto Rico. J Urban Health. 2012;89(3):519–26. https://doi.org/10.1007/s11524-011-9662-6 .
Holt AC, Schwope DM, Le K, Schrecker JP, Heltsley R. Widespread distribution of xylazine detected throughout the United States in healthcare patient samples. J Addict Med. 2023. https://doi.org/10.1097/ADM.0000000000001132 .
DEA. PUBLIC SAFETY ALERT: DEA Reports Widespread Threat of Fentanyl Mixed with Xylazine. https://www.dea.gov/alert/dea-reports-widespread-threat-fentanyl-mixed-xylazine
CTDPH. Connecticut Department of Public Health Drug Overdose Monthly Report. https://portal.ct.gov/-/media/DPH/Injury-and-Violence-Prevention/Opioid-Overdose-Data/Monthly-Death-Reports/2019-March-2023_Drug-Overdose-Deaths-Monthly-Report_Connecticut_updated-on-4-18-2023_Final.pdf
Quijano T, Crowell J, Eggert K, et al. Xylazine in the drug supply: emerging threats and lessons learned in areas with high levels of adulteration. Int J Drug Policy. 2023;120:104154. https://doi.org/10.1016/j.drugpo.2023.104154 .
Goddard P. Changing attitudes towards harm reduction among treatment professionals: a report from the American Midwest. Int J Drug Policy. 2003;14(3):257–60. https://doi.org/10.1016/S0955-3959(03)00075-6 .
Article Google Scholar
Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. https://doi.org/10.1191/1478088706qp063oa .
Gallanosa AG, Spyker DA, Shipe JR, Morris DL. Human xylazine overdose: a comparative review with clonidine, phenothiazines, and tricyclic antidepressants. Clin Toxicol. 1981;18(6):663–78. https://doi.org/10.3109/15563658108990293 .
Jones HE, Harris RJ, Downing BC, et al. Estimating the prevalence of problem drug use from drug-related mortality data. Addiction. 2020;115(12):2393–404. https://doi.org/10.1111/add.15111 .
Law MG, Degenhardt L, McKetin R. Methods estimating the prevalence of problem drug use. Int J Drug Policy. 2006;17(3):154–8. https://doi.org/10.1016/j.drugpo.2005.02.010 .
Muncan B, Walters SM, Ezell J, Ompad DC. “They look at us like junkies”: influences of drug use stigma on the healthcare engagement of people who inject drugs in New York City. Harm Reduct J. 2020;17(1):53. https://doi.org/10.1186/s12954-020-00399-8 .
Fong C, Mateu-Gelabert P, Ciervo C, et al. Medical provider stigma experienced by people who use drugs (MPS-PWUD): development and validation of a scale among people who currently inject drugs in New York City. Drug Alcohol Depend. 2021;221:108589. https://doi.org/10.1016/j.drugalcdep.2021.108589 .
Biancarelli DL, Biello KB, Childs E, et al. Strategies used by people who inject drugs to avoid stigma in healthcare settings. Drug Alcohol Depend. 2019;198:80–6. https://doi.org/10.1016/j.drugalcdep.2019.01.037 .
Paquette CE, Syvertsen JL, Pollini RA. Stigma at every turn: Health services experiences among people who inject drugs. Int J Drug Policy. 2018;57:104–10. https://doi.org/10.1016/j.drugpo.2018.04.004 .
Meyerson BE, Russell DM, Kichler M, Atkin T, Fox G, Coles HB. I don’t even want to go to the doctor when I get sick now: Healthcare experiences and discrimination reported by people who use drugs, Arizona 2019. Int J Drug Policy. 2021;93:103112. https://doi.org/10.1016/j.drugpo.2021.103112 .
Nolen S, Wilson T, Jacka BP, Li Y, Beaudoin FL, Marshall BDL. Prevalence and correlates of experiencing drug-related discrimination among people who use drugs presenting at emergency department at high risk of opioid overdose. Addict Behav Rep. 2023;17:100496. https://doi.org/10.1016/j.abrep.2023.100496 .
Download references
Acknowledgements
We would like to thank Sami Hamdan, MD, MPH, for his assistance with conducting interviews.
This project was funded by the Medical Staff Fund at Yale New Haven Hospital.
Author information
Authors and affiliations.
Department of Epidemiology of Microbial Diseases, Yale School of Public Health, New Haven, CT, USA
Katherine Hill & Robert Heimer
Yale Program in Addiction Medicine, Yale School of Medicine, New Haven, CT, USA
Rebecca Minahan-Rowley, Emma T. Biegacki & Kimberly L. Sue
Department of General Internal Medicine, Yale School of Medicine, New Haven, CT, USA
You can also search for this author in PubMed Google Scholar
Contributions
KH, KLS, and RH conceived of the project idea. KH led quantitative and qualitative instrument development, and all authors provided feedback on instruments. KH organized the quantitative phase in REDCap. KH, RM-R, and EB conducted qualitative interviews. KH conducted quantitative data analysis and qualitative thematic analysis and led manuscript creation. All authors contributed to the final version of the manuscript.
Corresponding author
Correspondence to Katherine Hill .
Ethics declarations
Ethics approval and consent to participate.
Yale’s Institutional Review Board deemed this study exempt from human subjects review. All potential participants in the quantitative phase were provided with information about this study at the beginning of the survey and completion of the survey was accepted as consent to participate. Prior to interviews in the qualitative phase, participants were provided an information sheet and consent form via email; these forms described the purpose and procedures of the study, their rights as participants, confidentiality measures, and potential risk. Participants had the option to have the documents verbally reviewed with them by a member of the study team and were given the opportunity to ask questions. Verbal consent to be interviewed and for recording the interview was obtained prior to beginning the qualitative phase and all participants were advised on their right to terminate participation at any time.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Supplement 1. , supplement 2. , rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/ .
Reprints and permissions
About this article
Cite this article.
Hill, K., Minahan-Rowley, R., Biegacki, E.T. et al. Providers’ knowledge and perception of xylazine in the unregulated drug supply: a sequential explanatory mixed-methods study. Harm Reduct J 21 , 148 (2024). https://doi.org/10.1186/s12954-024-01052-4
Download citation
Received : 13 May 2024
Accepted : 30 June 2024
Published : 16 August 2024
DOI : https://doi.org/10.1186/s12954-024-01052-4
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
How To Transcribe An Interview Qualitative Research
How To Write A Good Interview Script From Qualitative Research
Interview Transcript Template
(PDF) A method of analysing interview transcripts in qualitative
A Complete Guide to Interview Transcription for Beginners
Transcript Example (with Microsoft Word and PDF Templates)
COMMENTS
Interviewee Transcript Review as a Tool to Improve Data Quality and
Any researcher designing and undertaking interview-based research must make various decisions. In my research, a major consideration was that I would be undertaking semi-structured interviews in the context of domestic abuse, a field that is considered sensitive (Buchanan & Wendt, 2018).Sensitive research can be defined as any research that poses a potential risk to those being researched and ...
PDF Transcription as a Form of Qualitative Inquiry
work for qualitative inquiry (Charmaz, 2014, 2017; Locke, Golden-Biddle, & Feldman, 2004). In this chapter, I review the research on transcription and discuss the symbols and Microsoft Word formatting commands I used to transcribe a set of narrative interviews for my dissertation research. I share the results of two different tran-
Transcription & Qualitative Interview Data Analysis
As a researcher, you need to make the most of recorded interviews. Interview transcripts allow you to use the best qualitative analysis methods. Plus, you can focus only on tasks that add value to your research effort. Transcription is Essential to Qualitative Research Analysis. Qualitative data is often elusive to researchers.
Transcribing interviews for qualitative research
How to transcribe an interview for qualitative research. For qualitative research, transcription of interviews is a painstaking procedure that needs time and close attention to detail. It requires turning spoken words from your recorded audio or video into text. In qualitative research, this transcribing procedure is essential to data processing.
'Is that what I Said?' Interview Transcript Approval by Participants
Kvale (1996), who published explicit interviews in his book, Interviews: An introduction to qualitative research interviewing. admitted that this method of transcription was cause for incoherency in the text. He mentioned that a teacher who read a draft of the chapter in which his interview appeared, demanded that corrections be made to the ...
Transforming Transcripts Into Stories: A Multimethod Approach to
The pragmatic narratives found in transcripts represent human experience as it unfolds. Analyzing the narratives found in interview transcripts thus moves beyond providing descriptions and thematic developments as found in most qualitative studies. Crafting stories from interview transcripts involves a complex set of analytic processes.
How To Analyze Qualitative Research Interview Transcriptions
Coding. One of the most essential techniques for analyzing qualitative research interview transcripts is Coding. This refers to the procedure of categorizing and tagging individual pieces of data (in this case, segments of interview transcripts) with labels that signify specific themes or ideas.
Data Analysis in Qualitative Research: A Brief Guide to Using Nvivo
Data analysis in qualitative research is defined as the process of systematically searching and arranging the interview transcripts, observation notes, or other non-textual materials that the researcher accumulates to increase the understanding of the phenomenon.7 The process of analysing qualitative data predominantly involves coding or ...
How to Analyze Interview Transcripts in Qualitative Research
Qualitative research is a critical part of any successful study. Unlike quantitative data, a qualitative analysis adds color to academic and business reports. Interview transcripts are among the ...
How to Transcribe Interviews for Qualitative Research
Our ultimate guide to transcribe interviews for qualitative research. 1. Decide the important interview information. 2. Confirm what kind of transcript you need. 3. Have your tools ready.
Transcripts in Research
Introduction to transcripts in qualitative research. Qualitative data transcription holds a key role in research, acting as the building blocks from which findings are derived and conclusions are drawn.They are the textual representation of verbal data gathered through interviews, focus groups, and observational studies.Given their significance, it's essential to grasp why they are fundamental ...
Interviewee Transcript Review: assessing the impact on qualitative research
This paper assesses interviewee transcript review (ITR) as a technique for improving the rigour of interview-based, qualitative research. ITR is a process whereby interviewees are provided with verbatim transcripts of their interviews for the purposes of verifying accuracy, correcting errors or inaccuracies and providing clarifications. ITR, in various forms, is widely used among qualitative ...
Interviewee Transcript Review: assessing the impact on qualitative research
An accurate interview transcript can still represent poor quality data if the interviewee has inaccurately conveyed his or her knowledge or beliefs. Existing guidelines and methods protocols which address quality and rigour in qualitative research provide only limited and indirect guidance on how ITR techniques impact on data quality[10,19-22 ...
6 Tips on Transcribing Interviews for Qualitative Research
Transcribing interviews for qualitative research offers several benefits that contribute to the overall depth and success of the research process. Here are its key advantages: Comprehensive analysis: Transcripts capture every word, nuance and non-verbal cue, which is a goldmine for data analysis.
Constraints and Opportunities with Interview Transcription: Towards
Interviews, and then the transcripts, are methodological tools used to capture these discourses. ... In qualitative research, diction concerns how interviewers and participants choose words, especially with regard to correctness, clearness or effectiveness. A common feature of diction is the dropping of the "g" behind words.
From "Listen and Repeat" to "Listen and Revise": How to Transcribe
This is because whilst during an in-person interview the researcher can affect the quality of the transcript by choosing an empty venue, bringing a good quality recorder and placing it close to the interviewee(s), the accuracy of transcripts in the case of online interviews depends instead on the quality of the audio of the computer's or ...
6 Easy Steps in Learning How to Analyze Interview Data in Qualitative
Here are some steps to follow: 1. Gather Qualitative Data. Qualitative data can be collected through various means. For one, you can record the interview and take advantage of legal-grade transcription services. Taking this approach will help you avoid data loss and inaccuracies.
"The interviews were transcribed", but how? Reflections on management
In qualitative research, it is recurrent to conduct data collection through interviews, which must be first transcribed for the data to be analyzed. ... two transcripts from the same interview and its respective recording may present different words, putting in risk the meaning of the transcription and, consequently, the result of the data ...
A method of analysing interview transcripts in qualitative research
A method of analysing qualitative interview data is outlined as a stage-by-stage process. Some of the problems associated with the method are identified. ... A method of analysing interview transcripts in qualitative research Nurse Educ Today. 1991 Dec;11(6):461-6. doi: 10.1016/0260-6917(91)90009-y. Author P Burnard. PMID: ...
Analysing interview transcripts in qualitative research: How to
Thematic analysis serves as a vital tool in qualitative research, guiding researchers through complex interview transcripts to uncover underlying patterns and themes. By systematically organizing and interpreting qualitative data, thematic analysis enables researchers to identify significant narratives and insights that may otherwise remain hidden.
Three sample interview transcripts
The following three transcripts have been provided to help you test your coding skills. Please note these will open in a new window. Interview Transcript: Digestive Disorders - Brenda. Interview Transcript - A Teacher's Observations of Child Oppression. Interview Transcript: Digestive Disorders - Sam.
Transcription and Qualitative Methods: Implications for Third Sector
Qualitative research and transcription. While quantitative research seeks to explain, generalize and predict patterns through the analysis of variables, qualitative research questions are more interested in understanding and interpreting the socially constructed world around us (Bryman, 2016).This means that data are collected through documents, observation and interviews, and the latter are ...
Why Is It Common For Researchers To Transcribe Qualitative Interviews?
Transcribing qualitative sessions plays a significant role in ensuring confidentiality and adhering to ethical practices in research. One of the key aspects of research ethics is the protection of the participant's privacy. Interpretations allow experimenters to store and manage participants' responses while ensuring anonymity securely.
Transcription in Qualitative Research: A Comprehensive Guide for UX
Writing a transcript for qualitative research involves more than just typing out what you hear. ... Looppanel is an AI-powered research repository tool that can do extremely accurate interview transcription for UX research, among other cool features. It's special compared to other transcription services on this list, as it also lets you ...
6 Transcription Software For Qualitative Research
Enter transcription software for qualitative research. This software generates transcripts for meetings, interviews and lectures. (We sure wish we had this tech in college!) Suddenly, researchers can dive deeper into their work, analyzing more data. Using transcription audio software increases their productivity. It doesn't benefit ...
Providers' knowledge and perception of xylazine in the unregulated drug
For the qualitative phase, interview recordings were transcribed using Trint software and verified for accuracy by the first author (K.H.). Transcripts were entered into NVivo software (QSR International, Version 1.7.1) to facilitate thematic analysis . A codebook with both inductive and deductive codes drawn from the interview guide and ...








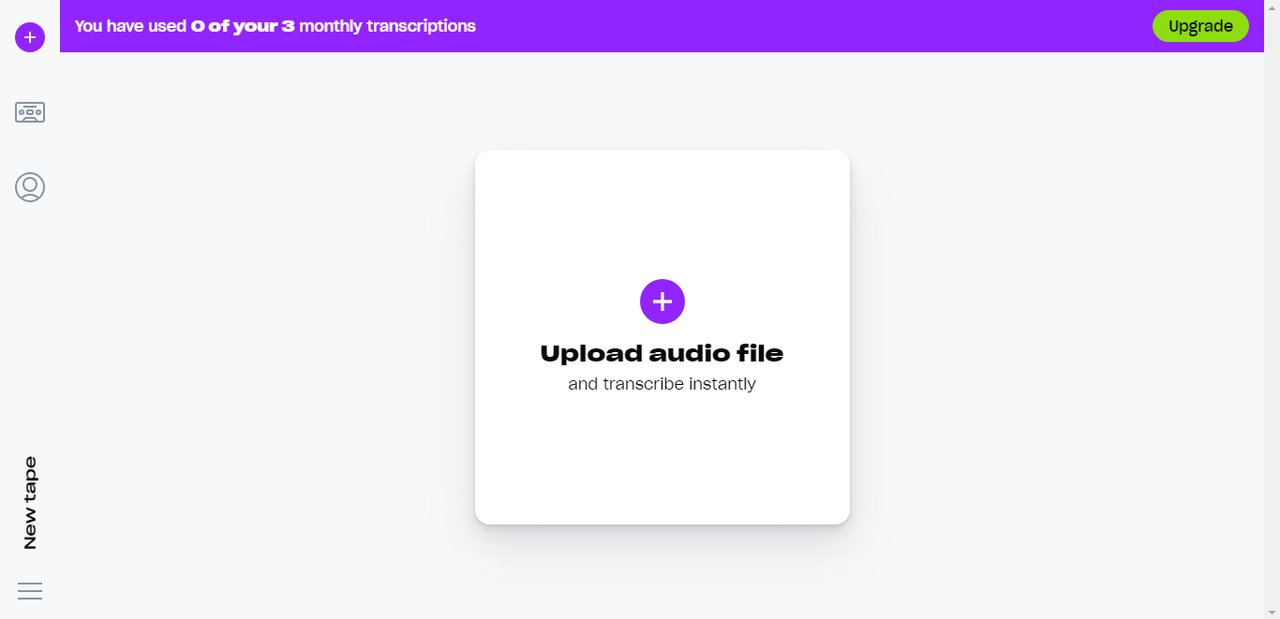
































.png)















IMAGES
COMMENTS
Any researcher designing and undertaking interview-based research must make various decisions. In my research, a major consideration was that I would be undertaking semi-structured interviews in the context of domestic abuse, a field that is considered sensitive (Buchanan & Wendt, 2018).Sensitive research can be defined as any research that poses a potential risk to those being researched and ...
work for qualitative inquiry (Charmaz, 2014, 2017; Locke, Golden-Biddle, & Feldman, 2004). In this chapter, I review the research on transcription and discuss the symbols and Microsoft Word formatting commands I used to transcribe a set of narrative interviews for my dissertation research. I share the results of two different tran-
As a researcher, you need to make the most of recorded interviews. Interview transcripts allow you to use the best qualitative analysis methods. Plus, you can focus only on tasks that add value to your research effort. Transcription is Essential to Qualitative Research Analysis. Qualitative data is often elusive to researchers.
How to transcribe an interview for qualitative research. For qualitative research, transcription of interviews is a painstaking procedure that needs time and close attention to detail. It requires turning spoken words from your recorded audio or video into text. In qualitative research, this transcribing procedure is essential to data processing.
Kvale (1996), who published explicit interviews in his book, Interviews: An introduction to qualitative research interviewing. admitted that this method of transcription was cause for incoherency in the text. He mentioned that a teacher who read a draft of the chapter in which his interview appeared, demanded that corrections be made to the ...
The pragmatic narratives found in transcripts represent human experience as it unfolds. Analyzing the narratives found in interview transcripts thus moves beyond providing descriptions and thematic developments as found in most qualitative studies. Crafting stories from interview transcripts involves a complex set of analytic processes.
Coding. One of the most essential techniques for analyzing qualitative research interview transcripts is Coding. This refers to the procedure of categorizing and tagging individual pieces of data (in this case, segments of interview transcripts) with labels that signify specific themes or ideas.
Data analysis in qualitative research is defined as the process of systematically searching and arranging the interview transcripts, observation notes, or other non-textual materials that the researcher accumulates to increase the understanding of the phenomenon.7 The process of analysing qualitative data predominantly involves coding or ...
Qualitative research is a critical part of any successful study. Unlike quantitative data, a qualitative analysis adds color to academic and business reports. Interview transcripts are among the ...
Our ultimate guide to transcribe interviews for qualitative research. 1. Decide the important interview information. 2. Confirm what kind of transcript you need. 3. Have your tools ready.
Introduction to transcripts in qualitative research. Qualitative data transcription holds a key role in research, acting as the building blocks from which findings are derived and conclusions are drawn.They are the textual representation of verbal data gathered through interviews, focus groups, and observational studies.Given their significance, it's essential to grasp why they are fundamental ...
This paper assesses interviewee transcript review (ITR) as a technique for improving the rigour of interview-based, qualitative research. ITR is a process whereby interviewees are provided with verbatim transcripts of their interviews for the purposes of verifying accuracy, correcting errors or inaccuracies and providing clarifications. ITR, in various forms, is widely used among qualitative ...
An accurate interview transcript can still represent poor quality data if the interviewee has inaccurately conveyed his or her knowledge or beliefs. Existing guidelines and methods protocols which address quality and rigour in qualitative research provide only limited and indirect guidance on how ITR techniques impact on data quality[10,19-22 ...
Transcribing interviews for qualitative research offers several benefits that contribute to the overall depth and success of the research process. Here are its key advantages: Comprehensive analysis: Transcripts capture every word, nuance and non-verbal cue, which is a goldmine for data analysis.
Interviews, and then the transcripts, are methodological tools used to capture these discourses. ... In qualitative research, diction concerns how interviewers and participants choose words, especially with regard to correctness, clearness or effectiveness. A common feature of diction is the dropping of the "g" behind words.
This is because whilst during an in-person interview the researcher can affect the quality of the transcript by choosing an empty venue, bringing a good quality recorder and placing it close to the interviewee(s), the accuracy of transcripts in the case of online interviews depends instead on the quality of the audio of the computer's or ...
Here are some steps to follow: 1. Gather Qualitative Data. Qualitative data can be collected through various means. For one, you can record the interview and take advantage of legal-grade transcription services. Taking this approach will help you avoid data loss and inaccuracies.
In qualitative research, it is recurrent to conduct data collection through interviews, which must be first transcribed for the data to be analyzed. ... two transcripts from the same interview and its respective recording may present different words, putting in risk the meaning of the transcription and, consequently, the result of the data ...
A method of analysing qualitative interview data is outlined as a stage-by-stage process. Some of the problems associated with the method are identified. ... A method of analysing interview transcripts in qualitative research Nurse Educ Today. 1991 Dec;11(6):461-6. doi: 10.1016/0260-6917(91)90009-y. Author P Burnard. PMID: ...
Thematic analysis serves as a vital tool in qualitative research, guiding researchers through complex interview transcripts to uncover underlying patterns and themes. By systematically organizing and interpreting qualitative data, thematic analysis enables researchers to identify significant narratives and insights that may otherwise remain hidden.
The following three transcripts have been provided to help you test your coding skills. Please note these will open in a new window. Interview Transcript: Digestive Disorders - Brenda. Interview Transcript - A Teacher's Observations of Child Oppression. Interview Transcript: Digestive Disorders - Sam.
Qualitative research and transcription. While quantitative research seeks to explain, generalize and predict patterns through the analysis of variables, qualitative research questions are more interested in understanding and interpreting the socially constructed world around us (Bryman, 2016).This means that data are collected through documents, observation and interviews, and the latter are ...
Transcribing qualitative sessions plays a significant role in ensuring confidentiality and adhering to ethical practices in research. One of the key aspects of research ethics is the protection of the participant's privacy. Interpretations allow experimenters to store and manage participants' responses while ensuring anonymity securely.
Writing a transcript for qualitative research involves more than just typing out what you hear. ... Looppanel is an AI-powered research repository tool that can do extremely accurate interview transcription for UX research, among other cool features. It's special compared to other transcription services on this list, as it also lets you ...
Enter transcription software for qualitative research. This software generates transcripts for meetings, interviews and lectures. (We sure wish we had this tech in college!) Suddenly, researchers can dive deeper into their work, analyzing more data. Using transcription audio software increases their productivity. It doesn't benefit ...
For the qualitative phase, interview recordings were transcribed using Trint software and verified for accuracy by the first author (K.H.). Transcripts were entered into NVivo software (QSR International, Version 1.7.1) to facilitate thematic analysis . A codebook with both inductive and deductive codes drawn from the interview guide and ...