
An official website of the United States government
The .gov means it's official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you're on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
- Browse Titles
NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health.
StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-.


StatPearls [Internet].
Delivery, face and brow presentation.
Julija Makajeva ; Mohsina Ashraf .
Affiliations
Last Update: January 9, 2023 .
- Continuing Education Activity
Face and brow presentation is a malpresentation during labor when the presenting part is either the face or, in the case of brow presentation, it is the area between the orbital ridge and the anterior fontanelle. This activity reviews the evaluation and management of these two presentations and explains the role of the interprofessional team in managing delivery safely for both the mother and the baby.
- Describe the mechanism of labor in the face and brow presentation.
- Summarize potential maternal and fetal complications during the face and brow presentations.
- Review different management approaches for the face and brow presentation.
- Outline some interprofessional strategies that will improve patient outcomes in delivery cases with face and brow presentation issues.
- Introduction
The term presentation describes the leading part of the fetus or the anatomical structure closest to the maternal pelvic inlet during labor. The presentation can roughly be divided into the following classifications: cephalic, breech, shoulder, and compound. Cephalic presentation is the most common and can be further subclassified as vertex, sinciput, brow, face, and chin. The most common presentation in term labor is the vertex, where the fetal neck is flexed to the chin, minimizing the head circumference.
Face presentation – an abnormal form of cephalic presentation where the presenting part is mentum. This typically occurs because of hyperextension of the neck and the occiput touching the fetal back. Incidence of face presentation is rare, accounting for approximately 1 in 600 of all presentations. [1] [2] [3]
In brow presentation, the neck is not extended as much as in face presentation, and the leading part is the area between the anterior fontanelle and the orbital ridges. Brow presentation is considered the rarest of all malpresentation with a prevalence of 1 in 500 to 1 in 4000 deliveries. [3]
Both face and brow presentations occur due to extension of the fetal neck instead of flexion; therefore, conditions that would lead to hyperextension or prevent flexion of the fetal neck can all contribute to face or brow presentation. These risk factors may be related to either the mother or the fetus. Maternal risk factors are preterm delivery, contracted maternal pelvis, platypelloid pelvis, multiparity, previous cesarean section, black race. Fetal risk factors include anencephaly, multiple loops of cord around the neck, masses of the neck, macrosomia, polyhydramnios. [2] [4] [5]
These malpresentations are usually diagnosed during the second stage of labor when performing a digital examination. It is possible to palpate orbital ridges, nose, malar eminences, mentum, mouth, gums, and chin in face presentation. Based on the position of the chin, face presentation can be further divided into mentum anterior, posterior, or transverse. In brow presentation, anterior fontanelle and face can be palpated except for the mouth and the chin. Brow presentation can then be further described based on the position of the anterior fontanelle as frontal anterior, posterior, or transverse.
Diagnosing the exact presentation can be challenging, and face presentation may be misdiagnosed as frank breech. To avoid any confusion, a bedside ultrasound scan can be performed. [6] The ultrasound imaging can show a reduced angle between the occiput and the spine or, the chin is separated from the chest. However, ultrasound does not provide much predicting value in the outcome of the labor. [7]
- Anatomy and Physiology
Before discussing the mechanism of labor in the face or brow presentation, it is crucial to highlight some anatomical landmarks and their measurements.
Planes and Diameters of the Pelvis
The three most important planes in the female pelvis are the pelvic inlet, mid pelvis, and pelvic outlet.
Four diameters can describe the pelvic inlet: anteroposterior, transverse, and two obliques. Furthermore, based on the different landmarks on the pelvic inlet, there are three different anteroposterior diameters, named conjugates: true conjugate, obstetrical conjugate, and diagonal conjugate. Only the latter can be measured directly during the obstetric examination. The shortest of these three diameters is obstetrical conjugate, which measures approximately 10.5 cm and is a distance between the sacral promontory and 1 cm below the upper border of the symphysis pubis. This measurement is clinically significant as the fetal head must pass through this diameter during the engagement phase. The transverse diameter measures about 13.5cm and is the widest distance between the innominate line on both sides.
The shortest distance in the mid pelvis is the interspinous diameter and usually is only about 10 cm.
Fetal Skull Diameters
There are six distinguished longitudinal fetal skull diameters:
- Suboccipito-bregmatic: from the center of anterior fontanelle (bregma) to the occipital protuberance, measuring 9.5 cm. This is the presenting diameter in vertex presentation.
- Suboccipito-frontal: from the anterior part of bregma to the occipital protuberance, measuring 10 cm
- Occipito-frontal: from the root of the nose to the most prominent part of the occiput, measuring 11.5cm
- Submento-bregmatic: from the center of the bregma to the angle of the mandible, measuring 9.5 cm. This is the presenting diameter in face presentation where the neck is hyperextended.
- Submento-vertical: from the midpoint between fontanelles and the angle of the mandible, measuring 11.5cm
- Occipito-mental: from the midpoint between fontanelles and the tip of the chin, measuring 13.5 cm. It is the presenting diameter in brow presentation.
Cardinal Movements of Normal Labor
- Neck flexion
- Internal rotation
- Extension (delivers head)
- External rotation (Restitution)
- Expulsion (delivery of anterior and posterior shoulders)
Some of the key movements are not possible in the face or brow presentations.
Based on the information provided above, it is obvious that labor will be arrested in brow presentation unless it spontaneously changes to face or vertex, as the occipito-mental diameter of the fetal head is significantly wider than the smallest diameter of the female pelvis. Face presentation can, however, be delivered vaginally, and further mechanisms of face delivery will be explained in later sections.
- Indications
As mentioned previously, spontaneous vaginal delivery can be successful in face presentation. However, the main indication for vaginal delivery in such circumstances would be a maternal choice. It is crucial to have a thorough conversation with a mother, explaining the risks and benefits of vaginal delivery with face presentation and a cesarean section. Informed consent and creating a rapport with the mother is an essential aspect of safe and successful labor.
- Contraindications
Vaginal delivery of face presentation is contraindicated if the mentum is lying posteriorly or is in a transverse position. In such a scenario, the fetal brow is pressing against the maternal symphysis pubis, and the short fetal neck, which is already maximally extended, cannot span the surface of the maternal sacrum. In this position, the diameter of the head is larger than the maternal pelvis, and it cannot descend through the birth canal. Therefore the cesarean section is recommended as the safest mode of delivery for mentum posterior face presentations.
Attempts to manually convert face presentation to vertex, manual or forceps rotation of the persistent posterior chin to anterior are contraindicated as they can be dangerous.
Persistent brow presentation itself is a contraindication for vaginal delivery unless the fetus is significantly small or the maternal pelvis is large.
Continuous electronic fetal heart rate monitoring is recommended for face and brow presentations, as heart rate abnormalities are common in these scenarios. One study found that only 14% of the cases with face presentation had no abnormal traces on the cardiotocograph. [8] It is advised to use external transducer devices to prevent damage to the eyes. When internal monitoring is inevitable, it is suggested to place monitoring devices on bony parts carefully.
People who are usually involved in the delivery of face/ brow presentation are:
- Experienced midwife, preferably looking after laboring woman 1:1
- Senior obstetrician
- Neonatal team - in case of need for resuscitation
- Anesthetic team - to provide necessary pain control (e.g., epidural)
- Theatre team - in case of failure to progress and an emergency cesarean section will be required.
- Preparation
No specific preparation is required for face or brow presentation. However, it is essential to discuss the labor options with the mother and birthing partner and inform members of the neonatal, anesthetic, and theatre co-ordinating teams.
- Technique or Treatment
Mechanism of Labor in Face Presentation
During contractions, the pressure exerted by the fundus of the uterus on the fetus and pressure of amniotic fluid initiate descent. During this descent, the fetal neck extends instead of flexing. The internal rotation determines the outcome of delivery, if the fetal chin rotates posteriorly, vaginal delivery would not be possible, and cesarean section is permitted. The approach towards mentum-posterior delivery should be individualized, as the cases are rare. Expectant management is acceptable in multiparous women with small fetuses, as a spontaneous mentum-anterior rotation can occur. However, there should be a low threshold for cesarean section in primigravida women or women with large fetuses.
When the fetal chin is rotated towards maternal symphysis pubis as described as mentum-anterior; in these cases further descend through the vaginal canal continues with approximately 73% cases deliver spontaneously. [9] Fetal mentum presses on the maternal symphysis pubis, and the head is delivered by flexion. The occiput is pointing towards the maternal back, and external rotation happens. Shoulders are delivered in the same manner as in vertex delivery.
Mechanism of Labor in Brow Presentation
As this presentation is considered unstable, it is usually converted into a face or an occiput presentation. Due to the cephalic diameter being wider than the maternal pelvis, the fetal head cannot engage; thus, brow delivery cannot take place. Unless the fetus is small or the pelvis is very wide, the prognosis for vaginal delivery is poor. With persistent brow presentation, a cesarean section is required for safe delivery.
- Complications
As the cesarean section is becoming a more accessible mode of delivery in malpresentations, the incidence of maternal and fetal morbidity and mortality during face presentation has dropped significantly. [10]
However, there are still some complications associated with the nature of labor in face presentation. Due to the fetal head position, it is more challenging for the head to engage in the birth canal and descend, resulting in prolonged labor.
Prolonged labor itself can provoke foetal distress and arrhythmias. If the labor arrests or signs of fetal distress appear on CTG, the recommended next step in management is an emergency cesarean section, which in itself carries a myriad of operative and post-operative complications.
Finally, due to the nature of the fetal position and prolonged duration of labor in face presentation, neonates develop significant edema of the skull and face. Swelling of the fetal airway may also be present, resulting in respiratory distress after birth and possible intubation.
- Clinical Significance
During vertex presentation, the fetal head flexes, bringing the chin to the chest, forming the smallest possible fetal head diameter, measuring approximately 9.5cm. With face and brow presentation, the neck hyperextends, resulting in greater cephalic diameters. As a result, the fetal head will engage later, and labor will progress more slowly. Failure to progress in labor is also more common in both presentations compared to vertex presentation.
Furthermore, when the fetal chin is in a posterior position, this prevents further flexion of the fetal neck, as browns are pressing on the symphysis pubis. As a result, descend through the birth canal is impossible. Such presentation is considered undeliverable vaginally and requires an emergency cesarean section.
Manual attempts to change face presentation to vertex, manual or forceps rotation to mentum anterior are considered dangerous and are discouraged.
- Enhancing Healthcare Team Outcomes
A multidisciplinary team of healthcare experts supports the woman and her child during labor and the perinatal period. For a face or brow presentation to be appropriately diagnosed, an experienced midwife and obstetrician must be involved in the vaginal examination and labor monitoring. As fetal anomalies, such as anencephaly or goiter, can contribute to face presentation, sonographers experienced in antenatal scanning should also be involved in the care. It is advised to inform the anesthetic and neonatal teams in advance of the possible need for emergency cesarean section and resuscitation of the neonate. [11] [12]
- Review Questions
- Access free multiple choice questions on this topic.
- Comment on this article.
Disclosure: Julija Makajeva declares no relevant financial relationships with ineligible companies.
Disclosure: Mohsina Ashraf declares no relevant financial relationships with ineligible companies.
This book is distributed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0) ( http://creativecommons.org/licenses/by-nc-nd/4.0/ ), which permits others to distribute the work, provided that the article is not altered or used commercially. You are not required to obtain permission to distribute this article, provided that you credit the author and journal.
- Cite this Page Makajeva J, Ashraf M. Delivery, Face and Brow Presentation. [Updated 2023 Jan 9]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-.
In this Page
Bulk download.
- Bulk download StatPearls data from FTP
Related information
- PubMed Links to PubMed
Similar articles in PubMed
- Sonographic diagnosis of fetal head deflexion and the risk of cesarean delivery. [Am J Obstet Gynecol MFM. 2020] Sonographic diagnosis of fetal head deflexion and the risk of cesarean delivery. Bellussi F, Livi A, Cataneo I, Salsi G, Lenzi J, Pilu G. Am J Obstet Gynecol MFM. 2020 Nov; 2(4):100217. Epub 2020 Aug 18.
- Review Sonographic evaluation of the fetal head position and attitude during labor. [Am J Obstet Gynecol. 2022] Review Sonographic evaluation of the fetal head position and attitude during labor. Ghi T, Dall'Asta A. Am J Obstet Gynecol. 2022 Jul 6; . Epub 2022 Jul 6.
- Stages of Labor. [StatPearls. 2024] Stages of Labor. Hutchison J, Mahdy H, Hutchison J. StatPearls. 2024 Jan
- Leopold Maneuvers. [StatPearls. 2024] Leopold Maneuvers. Superville SS, Siccardi MA. StatPearls. 2024 Jan
- Review Labor with abnormal presentation and position. [Obstet Gynecol Clin North Am. ...] Review Labor with abnormal presentation and position. Stitely ML, Gherman RB. Obstet Gynecol Clin North Am. 2005 Jun; 32(2):165-79.
Recent Activity
- Delivery, Face and Brow Presentation - StatPearls Delivery, Face and Brow Presentation - StatPearls
Your browsing activity is empty.
Activity recording is turned off.
Turn recording back on
Connect with NLM
National Library of Medicine 8600 Rockville Pike Bethesda, MD 20894
Web Policies FOIA HHS Vulnerability Disclosure
Help Accessibility Careers
Planning for a baby?
- Preconception Health
- Preparing for Pregnancy
- Assisted Pregnancy
- Second Pregnancy
Already Pregnant?
- Pregnancy Week by Week
- Health & Safety
- Live life better
- Preparing for the baby
- Pregnancy Diet & Fitness
Have a Baby?
- Baby Milestones
- Baby Basics
- Mother Care
- Activity & Fun
Have a Toddler?
- Toddler Mile Stones
- Toddler Basics
- Food & Feeding
- Child Safety & Health
- Games & Playtime
- Special Child
Positive Parenting
- Health & Hyginie
- Learning and Development
- Family Basics
Child Safety
- Special child Care
- Planning for Future
- Play, Games, activity & Fun
Life Skills
Premature baby, baby products, health & safety, what is brow presentation what are its complications.
Written by Editorial Team
Editorial Team
With a rich experience in pregnancy and parenting, our team of experts create insightful, well-curated, and easy-to-read content for our to-be-parents and parents at all stages of parenting..
What Is Brow Presentation?
What leads to brow presentation, diagnosis of brow presentation, how to avoid c-section if baby is in brow presentation, what complications can arise due to brow presentation.

- Polyhydramnios : Excess amniotic fluid can make it difficult for the baby’s head to take a flexed position
- Size and shape of the pelvis: Abnormally shaped and sized pelvis can make it difficult for the baby to pick up a vertex presentation. Android pelvis, which has a triangular or heart-shaped inlet with a narrower front part, is usually behind most of the brow presentations. Similarly, contracted pelvis, a pelvis that is abnormally small, can cause brow presentation
- Fetal abnormality: Fetal abnormalities such as hydrocephalus, anencephaly and neck masses accounts for the majority of brow presentations
- Premature birth/low birth weight baby: If the baby is born prematurely or if the baby is having low birth weight , the chances of brow presentation increases
- Big baby : If the baby is larger than normal size, the baby tends to extend its head instead of curling inward
- Multiple pregnancies: Multiple pregnancies also increase the risk of brow presentation
- Multiple nuchal cords: If the umbilical cord wraps around the baby’s neck, obviously, it cannot tuck its chin into the chest. In such cases, the baby tends to be brow or face presentations
- Laxity of the uterus: If the uterine wall loses its firmness, the baby may not able to hold its chin tucked to the chest firmly and the baby tends to be in brow presentation
- Cephalopelvic disproportion (CPD): If the mother’s pelvis and the baby’s head are not proportionate to each other, brow presentation can happen

- Manual rotation: Doctor inserts his hand through the cervix and tries to flex the baby’s head
- The baby’s head should be engaged in the pelvis and should be in a front anterior position
- The pelvis should have sufficient room to permit the ventouse cup to be inserted posteriorly and to reach the occiput
- Ability and experience of the obstetrician
- How favorable is the position of the baby’s head inside the pelvis
- Available space inside the pelvis
- Increased chances of spinal cord injury are associated with brow presentation
- Fetal distress
- Abnormal shape of the baby’s head after delivery
- Prolonged labor
- Increased chances of using forceps which in turn increases the chances of facial trauma
- Obstructed labor
Advantages Of Saffron During Pregnancy
Saffron is the dried stigma of Crocus Sativus flower, i.e. the thread-like part at the centre which contains pollen.
Editorial Team,
With a rich experience in pregnancy and parenting, our team of experts create insightful, well-curated, and easy-to-read content for our to-be-parents and parents at all stages of parenting. Read more.

Responses (0)
Want curated content sharply tailored for your exact stage of parenting, read this next, related articles.

500 Popular Telugu Baby Boy Names With Meaning

Is it Safe to Watch Movies in Theater During Pregnancy?

Breastfeeding Classes During Pregnancy – Top Benefits and Importance

Can High Stress Cause a Miscarriage?

Cleaning During Pregnancy – Do’s And Don’ts

Bowling During Pregnancy – Is it Safe to Go?
Sponsored content
Discover great local businesses around you for your kids..
Get regular updates, great recommendations and other right stuff at the right time.
Premium Access
Join our community of 50K+ Moms and get access to exclusive features & resources in our app.
Pay Rs 25/- and read this article (One time access)

Our site uses cookies to make your experience on this site even better. We hope you think that is sweet.
Create account
Focus your wanderlust. create your account to get curated stories and recommendations., already have an account sign in.
Don't have an account? Sign up forgot password?
Get curated personalized content., articles and resources served personalized as per the stage of your parenting., already have an account login, choose one..

Enter dates
Learn how UpToDate can help you.
Select the option that best describes you
- Medical Professional
- Resident, Fellow, or Student
- Hospital or Institution
- Group Practice
- Patient or Caregiver
- Find in topic
RELATED TOPICS
INTRODUCTION
Diagnosis and management of face and brow presentations will be reviewed here. Other cephalic malpresentations are discussed separately. (See "Occiput posterior position" and "Occiput transverse position" .)
Prevalence — Face and brow presentation are uncommon. Their prevalences compared with other types of malpresentations are shown below [ 1-9 ]:
● Occiput posterior – 1/19 deliveries
● Breech – 1/33 deliveries
Medical Information

Delivery, Face Presentation, and Brow Presentation: Understanding Fetal Positions and Birth Scenarios
Introduction:.
During childbirth, the position of the baby plays a significant role in the delivery process. While the most common fetal presentation is the head-down position (vertex presentation), variations can occur, such as face presentation and brow presentation. This comprehensive article aims to provide a thorough understanding of delivery, face presentation, and brow presentation, including their definitions, causes, complications, and management approaches.
Delivery Process:
- Normal Vertex Presentation: In a typical delivery, the baby is positioned head-down, with the back of the head (occiput) leading the way through the birth canal.
- Engagement and Descent: Prior to delivery, the baby's head engages in the pelvis and gradually descends, preparing for birth.
- Cardinal Movements: The baby undergoes a series of cardinal movements, including flexion, internal rotation, extension, external rotation, and restitution, which facilitate the passage through the birth canal.
Face Presentation:
- Definition: Face presentation occurs when the baby's face is positioned to lead the way through the birth canal instead of the vertex (head).
- Causes: Face presentation can occur due to factors such as abnormal fetal positioning, multiple pregnancies, uterine abnormalities, or maternal pelvic anatomy.
- Complications: Face presentation is associated with an increased risk of prolonged labor, difficulties in delivery, increased fetal malposition, birth injuries, and the need for instrumental delivery.
- Management: The management of face presentation depends on several factors, including the progression of labor, the size of the baby, and the expertise of the healthcare provider. Options may include closely monitoring the progress of labor, attempting a vaginal delivery with careful maneuvers, or considering a cesarean section if complications arise.
Brow Presentation:
- Definition: Brow presentation occurs when the baby's head is partially extended, causing the brow (forehead) to lead the way through the birth canal.
- Causes: Brow presentation may result from abnormal fetal positioning, poor engagement of the fetal head, or other factors that prevent full flexion or extension.
- Complications: Brow presentation is associated with a higher risk of prolonged labor, difficulty in descent, increased chances of fetal head entrapment, birth injuries, and the potential need for instrumental delivery or cesarean section.
- Management: The management of brow presentation depends on various factors, such as cervical dilation, progress of labor, fetal size, and the presence of complications. Close monitoring, expert assessment, and a multidisciplinary approach may be necessary to determine the safest delivery method, which can include vaginal delivery with careful maneuvers, instrumental assistance, or cesarean section if warranted.
Delivery Techniques and Intervention:
- Obstetric Maneuvers: In certain situations, skilled healthcare providers may use obstetric maneuvers, such as manual rotation or the use of forceps or vacuum extraction, to facilitate delivery, reposition the baby, or prevent complications.
- Cesarean Section: In cases where vaginal delivery is not possible or poses risks to the mother or baby, a cesarean section may be performed to ensure a safe delivery.
Conclusion:
Delivery, face presentation, and brow presentation are important aspects of childbirth that require careful management and consideration. Understanding the definitions, causes, complications, and appropriate management approaches associated with these fetal positions can help healthcare providers ensure safe and successful deliveries. Individualized care, close monitoring, and multidisciplinary collaboration are crucial in optimizing maternal and fetal outcomes during these unique delivery scenarios.
Hashtags: #Delivery #FacePresentation #BrowPresentation #Childbirth #ObstetricDelivery
On the Article

Krish Tangella MD, MBA

Alexander Enabnit

Alexandra Warren
Please log in to post a comment.
Related Articles
Test your knowledge, asked by users, related centers, related specialties, related physicians, related procedures, related resources, join dovehubs.
and connect with fellow professionals
Related Directories
At DoveMed, our utmost priority is your well-being. We are an online medical resource dedicated to providing you with accurate and up-to-date information on a wide range of medical topics. But we're more than just an information hub - we genuinely care about your health journey. That's why we offer a variety of products tailored for both healthcare consumers and professionals, because we believe in empowering everyone involved in the care process. Our mission is to create a user-friendly healthcare technology portal that helps you make better decisions about your overall health and well-being. We understand that navigating the complexities of healthcare can be overwhelming, so we strive to be a reliable and compassionate companion on your path to wellness. As an impartial and trusted online resource, we connect healthcare seekers, physicians, and hospitals in a marketplace that promotes a higher quality, easy-to-use healthcare experience. You can trust that our content is unbiased and impartial, as it is trusted by physicians, researchers, and university professors around the globe. Importantly, we are not influenced or owned by any pharmaceutical, medical, or media companies. At DoveMed, we are a group of passionate individuals who deeply care about improving health and wellness for people everywhere. Your well-being is at the heart of everything we do.
For Patients
For professionals, for partners.
- Getting pregnant
- Preschooler
- Life as a parent
- Baby essentials
- Find your birth club
- Free antenatal classes
- Meet local parents & parents-to-be
- See all in Community
- Ovulation calculator
- Am I pregnant quiz
- How to get pregnant fast
- Best sex positions
- Signs of pregnancy
- How many days after your period can you get pregnant?
- How age affects fertility
- Very early signs of pregnancy
- What fertile cervical mucus looks like
- Think you're pregnant but the test is negative?
- Faint line on pregnancy test
- See all in Getting pregnant
- Pregnancy week by week
- How big is my baby?
- Due date calculator
- Baby movements week by week
- Symptoms you should never ignore
- Hospital bag checklist
- Signs of labour
- Your baby's position in the womb
- Baby gender predictor
- Vaginal spotting
- Fetal development chart
- See all in Pregnancy
- Baby names finder
- Baby name inspiration
- Popular baby names 2022
- Numerology calculator
- Gender-neutral names
- Old-fashioned names
- See all in Baby names
- Your baby week by week
- Baby milestones by month
- Baby rash types
- Baby poop chart
- Ways to soothe a crying baby
- Safe co-sleeping
- Teething signs
- Growth spurts
- See all in Baby
- Your toddler month by month
- Toddler development milestones
- Dealing with tantrums
- Toddler meals
- Food & fussy eating
- When to start potty training
- Moving from a cot to a bed
- Help your child sleep through
- Games & activities
- Vomiting: what's normal?
- See all in Toddler
- Your child month by month
- Food ideas & nutrition
- How kids learn to share
- Coping with aggression
- Bedtime battles
- Anxiety in children
- Dealing with public tantrums
- Great play ideas
- Is your child ready for school?Top tips for starting school
- See all in Preschooler
- Postnatal symptoms to watch out for
- Stitches after birth
- Postpartum blood clots
- Baby showers
- Sex secrets for parents
- See all in Life as a parent
- Best baby products
- Best formula and bottles for a windy baby
- Best car seats if you need three to fit
- Best nappies
- Best Moses baskets
- Best baby registries
- Best baby sleeping bags
- Best baby humidifier
- Best baby monitors
- Best baby bath seat
- Best baby food
- See all in Baby essentials
- Back pain in pregnancy
- Pelvic girdle pain
- Perineal massage
- Signs you're having a boy
- Signs you're having a girl
- Can you take fish oil while pregnant?
- 18 weeks pregnant bump
- Can you eat salami when pregnant?
- Edwards' syndrome
- Missed miscarriage
- Should I harvest my colostrum?
- Rhesus positive vs. Rhesus negative
- What do contractions feel like?
- Hunger in early pregnancy
- First poop after birth
- When do babies sit up?
- When can babies have salt?
- MMR vaccine rash
- Vaping while breastfeeding
- How to transition from formula to milk
- When do babies start grabbing things?
- Sperm allergy: can sperm cause itching?
- How long after taking folic acid can I get pregnant?
What is brow presentation?

- the size or shape of your pelvis
- because your baby is premature
- an abnormality that prevents your baby from tucking in her chin
- having too much amniotic fluid ( polyhydramnios )
Was this article helpful?
What is asynclitic presentation?

Forceps and ventouse (assisted birth)

Would you use complementary therapies during labour?
10 things your midwife will do after birth.

Where to go next

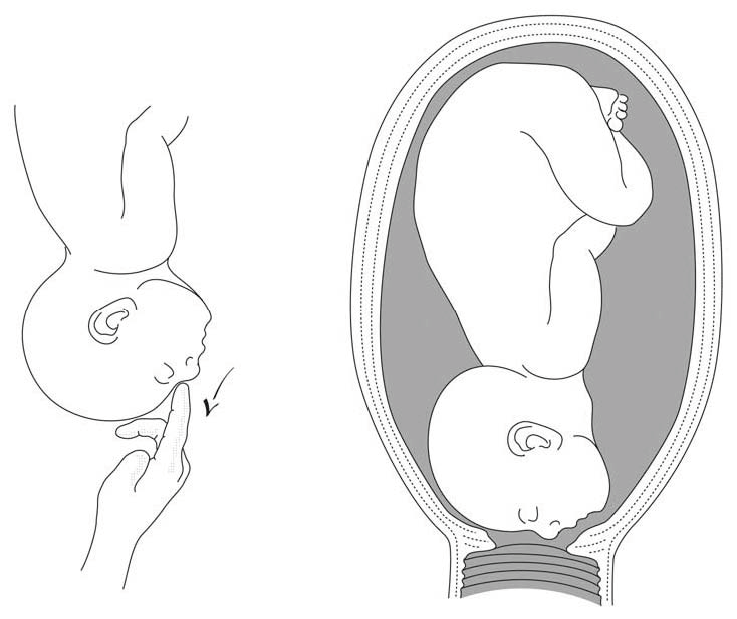
7.10 Brow presentation
Brow presentation constitutes an absolute foeto-pelvic disproportion, and vaginal delivery is impossible (except with preterm birth or extremely low birth weight).
This is an obstetric emergency, because labour is obstructed and there is a risk of uterine rupture and foetal distress.
7.10.1 Diagnosis
- Head is high; as with a face presentation, there is a cleft between the head and back, but it is less marked.
- the chin (it is not a face presentation),
- the posterior fontanelle (it is not a vertex presentation).
Figures 7.9 - Brow presentation

Any mobile presenting part can subsequently flex. The diagnosis of brow presentation is, therefore, not made until after the membranes have ruptured and the head has begun to engage in a fixed presentation. Some brow presentations will spontaneously convert to a vertex or, more rarely, a face presentation.
During delivery, the presenting part is slow to descend: the brow is becoming impacted.
7.10.2 Management
Foetus alive.
- Perform a caesarean section. When performing the caesarean section, an assistant must be ready to free the head by pushing it upward with a hand in the vagina.
- Convert the brow presentation to a face presentation: between contractions, insert the fingers through the cervix and move the head, encouraging extension (Figures 7.10).
- Attempt internal podalic version ( Section 7.9 ).
Both these manoeuvres pose a significant risk of uterine rupture. Vacuum extraction, forceps and symphysiotomy are contra-indicated.
Foetus dead
Perform an embryotomy if the cervix is sufficiently dilated (Chapter 9, Section 9.7 ) otherwise, a caesarean section.

- Physician Physician Board Reviews Physician Associate Board Reviews CME Lifetime CME Free CME
- Student USMLE Step 1 USMLE Step 2 USMLE Step 3 COMLEX Level 1 COMLEX Level 2 COMLEX Level 3 96 Medical School Exams Student Resource Center NCLEX - RN NCLEX - LPN/LVN/PN 24 Nursing Exams
- Nurse Practitioner APRN/NP Board Reviews CNS Certification Reviews CE - Nurse Practitioner FREE CE
- Nurse RN Certification Reviews CE - Nurse FREE CE
- Pharmacist Pharmacy Board Exam Prep CE - Pharmacist
- Allied Allied Health Exam Prep Dentist Exams CE - Social Worker CE - Dentist
- Point of Care
- Free CME/CE
Delivery, Face and Brow Presentation
Introduction.
The term presentation describes the leading part of the fetus or the anatomical structure closest to the maternal pelvic inlet during labor. The presentation can roughly be divided into the following classifications: cephalic, breech, shoulder, and compound. Cephalic presentation is the most common and can be further subclassified as vertex, sinciput, brow, face, and chin. The most common presentation in term labor is the vertex, where the fetal neck is flexed to the chin, minimizing the head circumference.
Face presentation – an abnormal form of cephalic presentation where the presenting part is mentum. This typically occurs because of hyperextension of the neck and the occiput touching the fetal back. Incidence of face presentation is rare, accounting for approximately 1 in 600 of all presentations. [1] [2] [3]
In brow presentation, the neck is not extended as much as in face presentation, and the leading part is the area between the anterior fontanelle and the orbital ridges. Brow presentation is considered the rarest of all malpresentation with a prevalence of 1 in 500 to 1 in 4000 deliveries. [3]
Both face and brow presentations occur due to extension of the fetal neck instead of flexion; therefore, conditions that would lead to hyperextension or prevent flexion of the fetal neck can all contribute to face or brow presentation. These risk factors may be related to either the mother or the fetus. Maternal risk factors are preterm delivery, contracted maternal pelvis, platypelloid pelvis, multiparity, previous cesarean section, black race. Fetal risk factors include anencephaly, multiple loops of cord around the neck, masses of the neck, macrosomia, polyhydramnios. [2] [4] [5]
These malpresentations are usually diagnosed during the second stage of labor when performing a digital examination. It is possible to palpate orbital ridges, nose, malar eminences, mentum, mouth, gums, and chin in face presentation. Based on the position of the chin, face presentation can be further divided into mentum anterior, posterior, or transverse. In brow presentation, anterior fontanelle and face can be palpated except for the mouth and the chin. Brow presentation can then be further described based on the position of the anterior fontanelle as frontal anterior, posterior, or transverse.
Diagnosing the exact presentation can be challenging, and face presentation may be misdiagnosed as frank breech. To avoid any confusion, a bedside ultrasound scan can be performed. [6] The ultrasound imaging can show a reduced angle between the occiput and the spine or, the chin is separated from the chest. However, ultrasound does not provide much predicting value in the outcome of the labor. [7]
Anatomy and Physiology
Register for free and read the full article, learn more about a subscription to statpearls point-of-care.
Before discussing the mechanism of labor in the face or brow presentation, it is crucial to highlight some anatomical landmarks and their measurements.
Planes and Diameters of the Pelvis
The three most important planes in the female pelvis are the pelvic inlet, mid pelvis, and pelvic outlet.
Four diameters can describe the pelvic inlet: anteroposterior, transverse, and two obliques. Furthermore, based on the different landmarks on the pelvic inlet, there are three different anteroposterior diameters, named conjugates: true conjugate, obstetrical conjugate, and diagonal conjugate. Only the latter can be measured directly during the obstetric examination. The shortest of these three diameters is obstetrical conjugate, which measures approximately 10.5 cm and is a distance between the sacral promontory and 1 cm below the upper border of the symphysis pubis. This measurement is clinically significant as the fetal head must pass through this diameter during the engagement phase. The transverse diameter measures about 13.5cm and is the widest distance between the innominate line on both sides.
The shortest distance in the mid pelvis is the interspinous diameter and usually is only about 10 cm.
Fetal Skull Diameters
There are six distinguished longitudinal fetal skull diameters:
- Suboccipito-bregmatic: from the center of anterior fontanelle (bregma) to the occipital protuberance, measuring 9.5 cm. This is the presenting diameter in vertex presentation.
- Suboccipito-frontal: from the anterior part of bregma to the occipital protuberance, measuring 10 cm
- Occipito-frontal: from the root of the nose to the most prominent part of the occiput, measuring 11.5cm
- Submento-bregmatic: from the center of the bregma to the angle of the mandible, measuring 9.5 cm. This is the presenting diameter in face presentation where the neck is hyperextended.
- Submento-vertical: from the midpoint between fontanelles and the angle of the mandible, measuring 11.5cm
- Occipito-mental: from the midpoint between fontanelles and the tip of the chin, measuring 13.5 cm. It is the presenting diameter in brow presentation.
Cardinal Movements of Normal Labor
- Neck flexion
- Internal rotation
- Extension (delivers head)
- External rotation (Restitution)
- Expulsion (delivery of anterior and posterior shoulders)
Some of the key movements are not possible in the face or brow presentations.
Based on the information provided above, it is obvious that labor will be arrested in brow presentation unless it spontaneously changes to face or vertex, as the occipito-mental diameter of the fetal head is significantly wider than the smallest diameter of the female pelvis. Face presentation can, however, be delivered vaginally, and further mechanisms of face delivery will be explained in later sections.
Indications
As mentioned previously, spontaneous vaginal delivery can be successful in face presentation. However, the main indication for vaginal delivery in such circumstances would be a maternal choice. It is crucial to have a thorough conversation with a mother, explaining the risks and benefits of vaginal delivery with face presentation and a cesarean section. Informed consent and creating a rapport with the mother is an essential aspect of safe and successful labor.
Contraindications
Vaginal delivery of face presentation is contraindicated if the mentum is lying posteriorly or is in a transverse position. In such a scenario, the fetal brow is pressing against the maternal symphysis pubis, and the short fetal neck, which is already maximally extended, cannot span the surface of the maternal sacrum. In this position, the diameter of the head is larger than the maternal pelvis, and it cannot descend through the birth canal. Therefore the cesarean section is recommended as the safest mode of delivery for mentum posterior face presentations.
Attempts to manually convert face presentation to vertex, manual or forceps rotation of the persistent posterior chin to anterior are contraindicated as they can be dangerous.
Persistent brow presentation itself is a contraindication for vaginal delivery unless the fetus is significantly small or the maternal pelvis is large.
Continuous electronic fetal heart rate monitoring is recommended for face and brow presentations, as heart rate abnormalities are common in these scenarios. One study found that only 14% of the cases with face presentation had no abnormal traces on the cardiotocograph. [8] It is advised to use external transducer devices to prevent damage to the eyes. When internal monitoring is inevitable, it is suggested to place monitoring devices on bony parts carefully.
People who are usually involved in the delivery of face/ brow presentation are:
- Experienced midwife, preferably looking after laboring woman 1:1
- Senior obstetrician
- Neonatal team - in case of need for resuscitation
- Anesthetic team - to provide necessary pain control (e.g., epidural)
- Theatre team - in case of failure to progress and an emergency cesarean section will be required.
Preparation
No specific preparation is required for face or brow presentation. However, it is essential to discuss the labor options with the mother and birthing partner and inform members of the neonatal, anesthetic, and theatre co-ordinating teams.
Technique or Treatment
Mechanism of Labor in Face Presentation
During contractions, the pressure exerted by the fundus of the uterus on the fetus and pressure of amniotic fluid initiate descent. During this descent, the fetal neck extends instead of flexing. The internal rotation determines the outcome of delivery, if the fetal chin rotates posteriorly, vaginal delivery would not be possible, and cesarean section is permitted. The approach towards mentum-posterior delivery should be individualized, as the cases are rare. Expectant management is acceptable in multiparous women with small fetuses, as a spontaneous mentum-anterior rotation can occur. However, there should be a low threshold for cesarean section in primigravida women or women with large fetuses.
When the fetal chin is rotated towards maternal symphysis pubis as described as mentum-anterior; in these cases further descend through the vaginal canal continues with approximately 73% cases deliver spontaneously. [9] Fetal mentum presses on the maternal symphysis pubis, and the head is delivered by flexion. The occiput is pointing towards the maternal back, and external rotation happens. Shoulders are delivered in the same manner as in vertex delivery.
Mechanism of Labor in Brow Presentation
As this presentation is considered unstable, it is usually converted into a face or an occiput presentation. Due to the cephalic diameter being wider than the maternal pelvis, the fetal head cannot engage; thus, brow delivery cannot take place. Unless the fetus is small or the pelvis is very wide, the prognosis for vaginal delivery is poor. With persistent brow presentation, a cesarean section is required for safe delivery.
Complications
As the cesarean section is becoming a more accessible mode of delivery in malpresentations, the incidence of maternal and fetal morbidity and mortality during face presentation has dropped significantly. [10]
However, there are still some complications associated with the nature of labor in face presentation. Due to the fetal head position, it is more challenging for the head to engage in the birth canal and descend, resulting in prolonged labor.
Prolonged labor itself can provoke foetal distress and arrhythmias. If the labor arrests or signs of fetal distress appear on CTG, the recommended next step in management is an emergency cesarean section, which in itself carries a myriad of operative and post-operative complications.
Finally, due to the nature of the fetal position and prolonged duration of labor in face presentation, neonates develop significant edema of the skull and face. Swelling of the fetal airway may also be present, resulting in respiratory distress after birth and possible intubation.
Clinical Significance
During vertex presentation, the fetal head flexes, bringing the chin to the chest, forming the smallest possible fetal head diameter, measuring approximately 9.5cm. With face and brow presentation, the neck hyperextends, resulting in greater cephalic diameters. As a result, the fetal head will engage later, and labor will progress more slowly. Failure to progress in labor is also more common in both presentations compared to vertex presentation.
Furthermore, when the fetal chin is in a posterior position, this prevents further flexion of the fetal neck, as browns are pressing on the symphysis pubis. As a result, descend through the birth canal is impossible. Such presentation is considered undeliverable vaginally and requires an emergency cesarean section.
Manual attempts to change face presentation to vertex, manual or forceps rotation to mentum anterior are considered dangerous and are discouraged.
Enhancing Healthcare Team Outcomes
A multidisciplinary team of healthcare experts supports the woman and her child during labor and the perinatal period. For a face or brow presentation to be appropriately diagnosed, an experienced midwife and obstetrician must be involved in the vaginal examination and labor monitoring. As fetal anomalies, such as anencephaly or goiter, can contribute to face presentation, sonographers experienced in antenatal scanning should also be involved in the care. It is advised to inform the anesthetic and neonatal teams in advance of the possible need for emergency cesarean section and resuscitation of the neonate. [11] [12]
Gardberg M,Leonova Y,Laakkonen E, Malpresentations--impact on mode of delivery. Acta obstetricia et gynecologica Scandinavica. 2011 May; [PubMed PMID: 21501123]
Tapisiz OL,Aytan H,Altinbas SK,Arman F,Tuncay G,Besli M,Mollamahmutoglu L,Danışman N, Face presentation at term: a forgotten issue. The journal of obstetrics and gynaecology research. 2014 Jun; [PubMed PMID: 24888918]
Zayed F,Amarin Z,Obeidat B,Obeidat N,Alchalabi H,Lataifeh I, Face and brow presentation in northern Jordan, over a decade of experience. Archives of gynecology and obstetrics. 2008 Nov; [PubMed PMID: 18283473]
Bashiri A,Burstein E,Bar-David J,Levy A,Mazor M, Face and brow presentation: independent risk factors. The journal of maternal-fetal [PubMed PMID: 18570114]
Shaffer BL,Cheng YW,Vargas JE,Laros RK Jr,Caughey AB, Face presentation: predictors and delivery route. American journal of obstetrics and gynecology. 2006 May; [PubMed PMID: 16647888]
Bellussi F,Ghi T,Youssef A,Salsi G,Giorgetta F,Parma D,Simonazzi G,Pilu G, The use of intrapartum ultrasound to diagnose malpositions and cephalic malpresentations. American journal of obstetrics and gynecology. 2017 Dec; [PubMed PMID: 28743440]
Ghi T,Eggebø T,Lees C,Kalache K,Rozenberg P,Youssef A,Salomon LJ,Tutschek B, ISUOG Practice Guidelines: intrapartum ultrasound. Ultrasound in obstetrics [PubMed PMID: 29974596]
Benedetti TJ,Lowensohn RI,Truscott AM, Face presentation at term. Obstetrics and gynecology. 1980 Feb; [PubMed PMID: 7352081]
Ducarme G,Ceccaldi PF,Chesnoy V,Robinet G,Gabriel R, [Face presentation: retrospective study of 32 cases at term]. Gynecologie, obstetrique [PubMed PMID: 16630740]
Cruikshank DP,Cruikshank JE, Face and brow presentation: a review. Clinical obstetrics and gynecology. 1981 Jun; [PubMed PMID: 7307363]
Domingues AP,Belo A,Moura P,Vieira DN, Medico-legal litigation in Obstetrics: a characterization analysis of a decade in Portugal. Revista brasileira de ginecologia e obstetricia : revista da Federacao Brasileira das Sociedades de Ginecologia e Obstetricia. 2015 May; [PubMed PMID: 26107576]
. Intrapartum care for healthy women and babies. 2022 Dec 14:(): [PubMed PMID: 32212591]
Use the mouse wheel to zoom in and out, click and drag to pan the image
Brow Presentation
- First Online: 02 August 2023
Cite this chapter

- Syeda Batool Mazhar 2 &
- Zahra Ahmed Muslim 2
406 Accesses
Brow presentation is the rarest of all malpresentations. Anencephaly, neck masses in fetus, polyhydramnios, multiple loops of cord around neck are the fetal factors leading to brow presentation. Contracted pelvis, preterm labour, platypelloid pelvis are some of the contributory maternal factors for brow presentation. Diagnosis is usually made during second stage of labour during prevaginal examination when anterior frontanelle and face are palpated. Cesarean section is performed in brow presentation as it is unusual to get conversion in average sized fetus once membranes have ruptured.
This is a preview of subscription content, log in via an institution to check access.
Access this chapter
- Available as PDF
- Read on any device
- Instant download
- Own it forever
- Available as EPUB and PDF
- Durable hardcover edition
- Dispatched in 3 to 5 business days
- Free shipping worldwide - see info
Tax calculation will be finalised at checkout
Purchases are for personal use only
Institutional subscriptions
Arulkumaran S, Robson M, editors. Munro Kerr operative obstetrics. 13th ed. Elsevier, Amsterdam; 2019. p. 89–93.
Google Scholar
Malvasi A, Barbera A, Di Vagno G, Gimovsky A, Berghella V, Ghi T, Di Renzo GC, Tinelli A. Asynclitism: a literature review of an often forgotten clinical condition. J Matern Fetal Neonatal Med. 2015;28(16):1890–4. https://doi.org/10.3109/14767058.2014.972925 . Epub 2014 Oct 29.PMID: 25283847.
Article PubMed Google Scholar
Bellussi F, Ghi T, Youssef A, Salsi G, Giorgetta F, Parma D, Simonazzi G, Gianluigi P. The use of intrapartum ultrasound to diagnose malpositions and cephalic malpresentations. Am J Obstet Gynecol. 2017;217(6):633–41.
Lanni SM, Gherman R, Gonik B. Malpresentations. Amsterdam: Elsevier; 2017.
Book Google Scholar
Bashiri A, Burstein E, Bar-David J, et al. Face and brow presentation: independent risk factors. J Matern Fetal Neonatal Med. 2008;21(6):357–60.
Hawkins JL, Koffel BL. Chapter 35. In: Chestnut’s obstetric anesthesia: principles and practice: abnormal presentation & multiple gestation. 6th ed; 2020. p. 830.
Meltzer RM, Sactleben MR, Friedman EA. Brow presentation. Obstet Gynecol Surv. 1968;23(6):255–63.
Article Google Scholar
Borell U, Fernstrom I. The mechanism of labour in face and brow presentation: a radiological study. Acta Obstet Gynecol Scand. 1960;39:626–44.
Article CAS PubMed Google Scholar
Levy DL. Persistent brow presentation: a new approach to management. South Med J. 1976;69(2):191–2.
Download references
Author information
Authors and affiliations.
MCH Centre, PIMS, Islamabad, Pakistan
Syeda Batool Mazhar & Zahra Ahmed Muslim
You can also search for this author in PubMed Google Scholar
Editor information
Editors and affiliations.
Department of Obstetrics and Gynecology, Sarojini Naidu Medical College, Agra, Uttar Pradesh, India
Ruchika Garg
Rights and permissions
Reprints and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Singapore Pte Ltd.
About this chapter
Mazhar, S.B., Muslim, Z.A. (2023). Brow Presentation. In: Garg, R. (eds) Labour and Delivery. Springer, Singapore. https://doi.org/10.1007/978-981-19-6145-8_8
Download citation
DOI : https://doi.org/10.1007/978-981-19-6145-8_8
Published : 02 August 2023
Publisher Name : Springer, Singapore
Print ISBN : 978-981-19-6144-1
Online ISBN : 978-981-19-6145-8
eBook Packages : Medicine Medicine (R0)
Share this chapter
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Publish with us
Policies and ethics
- Find a journal
- Track your research
Enter search terms to find related medical topics, multimedia and more.
Advanced Search:
- Use “ “ for exact phrases.
- For example: “pediatric abdominal pain”
- Use – to remove results with certain keywords.
- For example: abdominal pain -pediatric
- Use OR to account for alternate keywords.
- For example: teenager OR adolescent
Fetal Presentation, Position, and Lie (Including Breech Presentation)
, MD, Children's Hospital of Philadelphia
- 3D Models (0)
- Calculators (0)

Abnormal fetal lie or presentation may occur due to fetal size, fetal anomalies, uterine structural abnormalities, multiple gestation, or other factors. Diagnosis is by examination or ultrasonography. Management is with physical maneuvers to reposition the fetus, operative vaginal delivery Operative Vaginal Delivery Operative vaginal delivery involves application of forceps or a vacuum extractor to the fetal head to assist during the second stage of labor and facilitate delivery. Indications for forceps... read more , or cesarean delivery Cesarean Delivery Cesarean delivery is surgical delivery by incision into the uterus. The rate of cesarean delivery was 32% in the United States in 2021 (see March of Dimes: Delivery Method). The rate has fluctuated... read more .
Terms that describe the fetus in relation to the uterus, cervix, and maternal pelvis are
Fetal presentation: Fetal part that overlies the maternal pelvic inlet; vertex (cephalic), face, brow, breech, shoulder, funic (umbilical cord), or compound (more than one part, eg, shoulder and hand)
Fetal position: Relation of the presenting part to an anatomic axis; for transverse presentation, occiput anterior, occiput posterior, occiput transverse
Fetal lie: Relation of the fetus to the long axis of the uterus; longitudinal, oblique, or transverse
Normal fetal lie is longitudinal, normal presentation is vertex, and occiput anterior is the most common position.
Abnormal fetal lie, presentation, or position may occur with
Fetopelvic disproportion (fetus too large for the pelvic inlet)
Fetal congenital anomalies
Uterine structural abnormalities (eg, fibroids, synechiae)
Multiple gestation
Several common types of abnormal lie or presentation are discussed here.

Transverse lie
Fetal position is transverse, with the fetal long axis oblique or perpendicular rather than parallel to the maternal long axis. Transverse lie is often accompanied by shoulder presentation, which requires cesarean delivery.
Breech presentation
There are several types of breech presentation.
Frank breech: The fetal hips are flexed, and the knees extended (pike position).
Complete breech: The fetus seems to be sitting with hips and knees flexed.
Single or double footling presentation: One or both legs are completely extended and present before the buttocks.
Types of breech presentations
Breech presentation makes delivery difficult ,primarily because the presenting part is a poor dilating wedge. Having a poor dilating wedge can lead to incomplete cervical dilation, because the presenting part is narrower than the head that follows. The head, which is the part with the largest diameter, can then be trapped during delivery.
Additionally, the trapped fetal head can compress the umbilical cord if the fetal umbilicus is visible at the introitus, particularly in primiparas whose pelvic tissues have not been dilated by previous deliveries. Umbilical cord compression may cause fetal hypoxemia.

Predisposing factors for breech presentation include
Preterm labor Preterm Labor Labor (regular uterine contractions resulting in cervical change) that begins before 37 weeks gestation is considered preterm. Risk factors include prelabor rupture of membranes, uterine abnormalities... read more
Multiple gestation Multifetal Pregnancy Multifetal pregnancy is presence of > 1 fetus in the uterus. Multifetal (multiple) pregnancy occurs in up to 1 of 30 deliveries. Risk factors for multiple pregnancy include Ovarian stimulation... read more
Uterine abnormalities
Fetal anomalies
If delivery is vaginal, breech presentation may increase risk of
Umbilical cord prolapse

Perinatal death
It is best to detect abnormal fetal lie or presentation before delivery. During routine prenatal care, clinicians assess fetal lie and presentation with physical examination in the late third trimester. Ultrasonography can also be done. If breech presentation is detected, external cephalic version can sometimes move the fetus to vertex presentation before labor, usually at 37 or 38 weeks. This technique involves gently pressing on the maternal abdomen to reposition the fetus. A dose of a short-acting tocolytic ( terbutaline 0.25 mg subcutaneously) may help. The success rate is about 50 to 75%. For persistent abnormal lie or presentation, cesarean delivery is usually done at 39 weeks or when the woman presents in labor.

Face or brow presentation
In face presentation, the head is hyperextended, and position is designated by the position of the chin (mentum). When the chin is posterior, the head is less likely to rotate and less likely to deliver vaginally, necessitating cesarean delivery.
Brow presentation usually converts spontaneously to vertex or face presentation.
Occiput posterior position
The most common abnormal position is occiput posterior.
The fetal neck is usually somewhat deflexed; thus, a larger diameter of the head must pass through the pelvis.
Progress may arrest in the second phase of labor. Operative vaginal delivery Operative Vaginal Delivery Operative vaginal delivery involves application of forceps or a vacuum extractor to the fetal head to assist during the second stage of labor and facilitate delivery. Indications for forceps... read more or cesarean delivery Cesarean Delivery Cesarean delivery is surgical delivery by incision into the uterus. The rate of cesarean delivery was 32% in the United States in 2021 (see March of Dimes: Delivery Method). The rate has fluctuated... read more is often required.
Position and Presentation of the Fetus
If a fetus is in the occiput posterior position, operative vaginal delivery or cesarean delivery is often required.
In breech presentation, the presenting part is a poor dilating wedge, which can cause the head to be trapped during delivery, often compressing the umbilical cord.
For breech presentation, usually do cesarean delivery at 39 weeks or during labor, but external cephalic version is sometimes successful before labor, usually at 37 or 38 weeks.
Drugs Mentioned In This Article
Was This Page Helpful?

Test your knowledge
Brought to you by Merck & Co, Inc., Rahway, NJ, USA (known as MSD outside the US and Canada) — dedicated to using leading-edge science to save and improve lives around the world. Learn more about the Merck Manuals and our commitment to Global Medical Knowledge.
- Permissions
- Cookie Settings
- Terms of use
- Veterinary Manual

- IN THIS TOPIC
Uptodate Reference Title
Face and brow presentations in labor.
INTRODUCTION — The vast majority of fetuses at term are in cephalic presentation. Approximately 5 percent of these fetuses are in a cephalic malpresentation, such as occiput posterior or transverse, face ( figure 1A-B ), or brow ( figure 2 ) [ 1 ].
Diagnosis and management of face and brow presentations will be reviewed here. Other cephalic malpresentations are discussed separately. (See "Occiput posterior position" and "Occiput transverse position" .)
Prevalence — Face and brow presentation are uncommon. Their prevalences compared with other types of malpresentations are shown below [ 1-9 ]:
● Occiput posterior – 1/19 deliveries
● Breech – 1/33 deliveries
● Face – 1/600 to 1/800 deliveries
● Brow – 1/500 to 1/4000 deliveries
● Transverse lie – 1/833 deliveries
● Compound – 1/1500 deliveries
The prevalence of face presentation at Parkland Memorial Hospital in Texas (United States) has decreased to 1/2000 deliveries in recent years [ 10 ], possibly because of fewer deliveries of fetuses with anomalies such as anencephaly [ 11,12 ]; however, others have not observed a decline [ 9,12,13 ].
Clinical significance — During labor in the occiput anterior presentation, the neck normally flexes to bring the chin to the chest, resulting in the relatively small suboccipito-bregmatic diameter (average length 9.5 cm) as the widest cephalic diameter that needs to negotiate the pelvis. This diameter is generally able to traverse the obstetric conjugate (average length 10.5 cm) ( figure 3 ), which is the shortest anteroposterior pelvic diameter. By comparison, the neck is extended in brow and face presentations, which present larger fetal cephalic diameters that need to negotiate the pelvis ( figure 4 ). Thus, protraction or arrest of descent is more likely, which increases the chances of maternal and neonatal morbidity from vaginal birth and the frequency for cesarean birth. Brow and mentum posterior face presentations are most likely to exhibit cephalopelvic dystocia unless the fetus is very small or the maternal pelvis is very large or both. (See 'Neonatal outcome' below and 'Neonatal outcome' below.)
Fetal heart rate abnormalities are more common than with occiput anterior position [ 2,14 ]. They may be due to more head compression or a higher frequency of cord compression.
Risk factors — Maternal or fetal anatomic factors that prevent flexion or favor extension of the fetal neck increase the risk for face/brow presentation. These factors include anencephaly, severe hydrocephalus with cephalomegaly, anterior neck mass, multiple nuchal cords, cephalopelvic disproportion, preterm birth/low birth weight, macrosomia, contracted maternal pelvis, platypelloid pelvis ( figure 5 ), multiparity, polyhydramnios, previous cesarean birth, and Black race [ 2,5,8,9,11-13 ].
In multiparous patients, poor abdominal muscle tone may permit the uterine fundus and fetal trunk to swing anteriorly, which may extend the cervical spine, leading to a face or brow presentation [ 13 ]. Alternatively, late engagement of the vertex in multiparous patients, often after the onset of labor, may be the predisposing factor [ 12 ].
A contracted maternal pelvis predisposes to malpresentation [ 12 ]. The increased risk of face/brow presentation in Black patients may be due to differences in pelvic dimensions between White and Black females and a higher rate of preterm birth in Black individuals [ 13,15-17 ]. The differences in pelvic dimensions may be related to environmental differences (eg, locomotion, load carrying, health, nutrition) [ 18 ].
Although preterm birth has been linked to face/brow presentation, possibly because a very small fetus can descend with the neck partially extended, the association between preterm birth and face presentation is weak [ 9,13 ].
Pregnancies with polyhydramnios may be at risk secondary to impaired swallowing due to a fetal anomaly (particularly anencephaly) [ 12 ] or to obstruction of the fetal trachea and esophagus from a hyperextended fetal neck [ 5 ].
FACE PRESENTATION
Definition — Face presentation refers to a fetal presentation in which the fetal face from forehead to chin is the leading fetal body part descending into the birth canal ( figure 1B ). The fetal neck is highly extended (sharply deflexed), such that the occiput may touch the back.
Diagnosis — The intrapartum diagnosis of face presentation is made by vaginal examination in the late first or the second stage of labor [ 5 ]. Palpation of the orbital ridge and orbits, saddle of the nose, mouth, and chin is diagnostic of face presentation. The fontanelles and sutures are not generally palpable [ 19 ]. At diagnosis, nearly 60 percent of face presentations are mentum anterior, 26 percent are mentum posterior, and 15 percent are mentum transverse, and may be designated as left or right ( figure 1A ) [ 11 ].
Intrapartum transabdominal, translabial, and/or transvaginal sonography of a face presentation will show a hyperextended fetal neck, with the orbits and nasal bridge at the center of the presenting part in the mid-sagittal plane [ 20 ]. Although imaging studies can be performed to confirm the diagnosis if it is uncertain, imaging is not mandatory, and results do not have prognostic value for predicting the outcome of labor [ 21 ].
Differential diagnosis — Face presentation may be misdiagnosed as a frank breech presentation on digital examination since the latter is more commonly encountered (and therefore expected). Both presentations are characterized by soft tissues with an orifice; however, careful palpation will identify the bony facial structures and lead to the correct diagnosis. With ultrasound readily available in most delivery units, confirmation of the type of malpresentation (breech or face) is easily obtained if needed.
Labor and delivery management
Fetal heart rate monitoring — The fetal heart rate is monitored continuously, ideally with an external device. An internal device may cause facial or ophthalmic injuries if improperly placed [ 22-24 ]. If internal monitoring is required, the electrode should be carefully applied over a bony structure such as the forehead, mandible, or zygomatic bones to minimize the risk of trauma [ 25 ].
Abnormalities of the fetal heart rate occur more frequently with face presentations [ 4,25,26 ]. In one series, severe variable and late decelerations developed in 29 and 24 percent of labors, respectively [ 25 ]. Only 14 percent of pregnancies had normal tracings. Moreover, 13 percent of the newborns had a low five-minute Apgar score.
Interpretation and management of abnormal fetal heart rate tracings are not affected by fetal presentation and are reviewed separately. We perform amnioinfusion for patients with variable decelerations (category 2 tracing), regardless of presentation, as long as vaginal birth is anticipated. (See "Intrapartum category I, II, and III fetal heart rate tracings: Management" .)
Mentum anterior — In mentum anterior face presentation, the fetal chin needs to pass under the symphysis pubis. For this to occur, the extended fetal neck may need to extend even more. After the chin clears the symphysis, further descent and fetal expulsion can occur [ 5 ]. Over 75 percent of mentum anterior fetuses are born vaginally [ 2,3,13,26,27 ].
The parturient may begin pushing at full dilation. Labor progress should be closely monitored as arrest of descent may occur, although not inevitably as in persistent mentum posterior position.
Oxytocin augmentation and cesarean birth are performed for standard obstetric indications [ 26 ]. (See "Labor: Overview of normal and abnormal progression" .)
Attempts at version or vacuum- or midforceps-assisted delivery should be avoided as they are associated with unnecessary maternal trauma and neonatal injury [ 28 ].
An outlet forceps-assisted delivery when the face is distending the perineum is not contraindicated if delivery must be facilitated but should only be performed by experienced clinicians familiar with the particular considerations involved. For example, in contrast to the occiput anterior position, engagement does not occur until the face is at +2 station [ 5 ]; the chin rather than the occiput is the focal point for orientation; and if Kielland forceps are applied, the left blade is applied to the right side of the head and the right blade to the left side [ 29,30 ]. The technique of forceps delivery is beyond the scope of this review.
Mentum posterior — In the mentum posterior face presentation, the fetal neck is already maximally extended and cannot extend further to allow the occiput to pass under the symphysis. Therefore, the mentum posterior face presentation will not deliver vaginally unless spontaneous rotation to mentum anterior occurs ( figure 6 ), often late in the second stage of labor [ 14 ], or the fetus is very small, or the pelvis is very large. If the fetal status is reassuring and there is normal labor progress, mentum posterior presentation can be managed expectantly to see if spontaneous rotation will occur [ 14 ].
Patients with abnormal labor progression are delivered by cesarean. We individualize management when labor is progressing. For example, in multiparous patients with an adequate pelvis and fetus estimated to weigh less than their prior newborns, we would follow labor progress closely and maintain a low threshold for abandoning attempts at vaginal birth if labor does not progress normally in the first or second stage. However, if the fetus is estimated to be larger than their prior newborns, or in nulliparous patients, we would recommend cesarean birth early in the labor course. There is consensus that assisted vaginal delivery is contraindicated for mentum posterior presentations [ 14,31,32 ].
In the past, manual version of the mentum posterior face to an occiput anterior or mentum anterior position was attempted using internal and external manipulation [ 33,34 ]. Although some clinicians have been successful with no serious neonatal or maternal complications, others have reported maternal deaths from uterine rupture, cord prolapse resulting in neonatal asphyxia, and cervical spine trauma resulting in severe neonatal neurologic sequelae [ 28 ]. Given the safety and ready availability of cesarean birth, we believe internal version should be reserved for occasions when cesarean birth is unable to be accomplished due to lack of surgical facilities and inability to arrange maternal transport, or absolute maternal refusal to allow a cesarean birth [ 34 ].
Mentum transverse — There are minimal published data on management of the mentum transverse position. Our management is the same as for mentum posterior.
Neonatal outcome — Prior to 1955, increased rates of intrapartum fetal death and perinatal mortality (approximately 10 percent) were reported for face presentation [ 5 ]. Perinatal mortality decreased to 2 to 3 percent by 1980, likely due to the increased use of cesarean birth, as well as other advances in obstetric and neonatal care [ 5 ]. Recent perinatal mortality data are not available.
Neonates who were in face presentation often have significant facial edema, facial bruising/ecchymosis, and skull molding [ 35 ]. This usually resolves within the first 24 to 48 hours of life. Personnel and equipment for performing endotracheal intubation should be readily available at birth [ 25 ]. Difficulty in ventilation during resuscitation has been reported and attributed to tracheal and laryngeal trauma and edema.
Facial trauma and spinal cord injury have also been described in case reports and are often associated with version, extraction, and midforceps rotations [ 2,23-25,36 ]. Appropriate management of face presentation, as described above, typically does not result in increased serious maternal or neonatal morbidity [ 2 ].
BROW PRESENTATION
Definition — Brow presentation refers to a presentation in which the fetal surface presenting in the birth canal extends from the anterior fontanelle to the brow (orbital ridge), but does not include the mouth and chin ( figure 2 ). The fetal neck is extended, but not to the degree of a face presentation.
Diagnosis — The diagnosis of brow presentation is made by vaginal examination in the second stage of labor [ 5 ]. Palpation of the forehead, orbital ridge, orbits, and saddle of the nose, but not the mouth and chin, is diagnostic of brow presentation. The anterior fontanelle is palpable, but the sagittal suture generally is not [ 19 ]. The brow may be anterior or posterior and described by the position or the anterior fontanelle as frontal anterior, transverse, or posterior [ 14 ].
There is increasing evidence that ultrasound is more accurate than vaginal examination for determining fetal position and can be used to determine or confirm abnormal presentation [ 37,38 ]. On transabdominal examination, if the occiput is anterior, the main finding is a reduction in occiput-spinal angle, usually around 90 degrees rather than over 120 degrees; if the occiput is posterior, the chin is separate from chest, and the cervical spine is curved (convex) anteriorly [ 19 ]. If a transperineal examination is performed, the fetal orbits are seen at the same level as the pubic symphysis.
Labor and delivery management — The fetal heart rate is monitored continuously during labor, ideally with an external device, since fetal heart rate abnormalities are more common than with occiput anterior position. An internal device may cause facial or ophthalmic injuries if improperly placed [ 22-24 ]. If internal monitoring is required, the electrode should be cautiously applied over a bony structure, such as the forehead, to minimize the risk of trauma [ 25 ].
Patients with a clinically adequate or proven pelvis can undergo a trial of labor since many brow presentations are transitional. In one review, when brow presentation was diagnosed early in labor, 67 to 75 percent of fetuses spontaneously converted to a more favorable presentation and delivered vaginally. When diagnosed late in labor, 50 percent spontaneously converted and delivered vaginally: in 30 percent, the neck extended further resulting in mentum anterior face presentation; in 20 percent, the neck flexed resulting in an occiput posterior presentation [ 2,5,39 ]. Conversion to occiput anterior is rare.
If the brow presentation persists, labor progress is usually protracted or arrests, necessitating cesarean birth. Oxytocin augmentation is not recommended in this setting, given the association between brow presentation and cephalopelvic disproportion [ 5,26,33 ]. Version or vacuum- or forceps-assisted delivery are not recommended, as the risks for maternal and fetal injury are high [ 5,14,31,32 ]. However, in settings where cesarean birth is not readily available, vacuum-assisted flexion of the fetal head may be considered [ 40 ].
In a minority of cases, spontaneous vaginal birth may be possible if the fetus is extremely small or macerated or the maternal pelvis is unusually large.
Neonatal outcome — Recognition and appropriate management of brow presentation, as described above, typically do not result in increased serious maternal or neonatal morbidity.
SOCIETY GUIDELINE LINKS — Links to society and government-sponsored guidelines from selected countries and regions around the world are provided separately. (See "Society guideline links: Labor" .)
SUMMARY AND RECOMMENDATIONS
Issues common to face and brow presentations
● Risk factors – Face and brow presentations are associated with multiparity, cephalopelvic disproportion, preterm birth, polyhydramnios, and fetal anomalies (eg, anencephaly, anterior neck mass). (See 'Risk factors' above.)
● Clinical significance – The deflexed neck in face or brow presentation inhibits head engagement and subsequent fetal descent. (See 'Clinical significance' above.)
● Cautions – The fetal heart rate is monitored continuously during labor, ideally with an external device, because of the increased prevalence of fetal heart rate decelerations. An internal device may cause facial or ophthalmic injuries if improperly placed. If internal monitoring is required, the electrode should be carefully applied over a bony structure to minimize the risk of trauma. (See 'Labor and delivery management' above.)
● Definition – In face presentation, the fetal face from forehead to chin is the leading fetal body part descending into the birth canal ( figure 1B ). The fetal neck is sharply deflexed and the occiput may touch the back. Nearly 60 percent of face presentations are mentum anterior, 26 percent are mentum posterior, and 15 percent are mentum transverse, and may be designated as left or right ( figure 1A ). (See 'Definition' above.)
● Diagnosis – The diagnosis of face presentation is made by vaginal examination. Palpation of the orbital ridge and orbits, saddle of the nose, mouth, and chin is diagnostic of face presentation ( figure 1A ). Ultrasound can be used to confirm or clarify the type of malpresentation if the clinical examination findings are unclear. (See 'Diagnosis' above.)
● Management
• Mentum anterior – Over 75 percent of mentum anterior fetuses deliver vaginally; this rate is similar to that for all fetuses in cephalic presentations. For face presentation with the mentum anterior, we suggest a trial of labor rather than cesarean birth ( Grade 2C ). Oxytocin augmentation may be administered in the setting of a normal fetus with protracted labor, as long as the fetal heart rate pattern remains reassuring. (See 'Labor and delivery management' above.)
• Mentum posterior – The mentum posterior face presentation will not deliver vaginally unless spontaneous rotation occurs, which is infrequent and occurs late in the second stage of labor, or the fetus is very small or the pelvis very large or both. As mentum posterior presentations are rare, we individualize management of such situations. In a multiparous patient with an adequate pelvis and fetus estimated to weigh less than her prior newborns, we follow labor progress closely and maintain a low threshold for abandoning attempts at vaginal birth if labor does not progress normally in the first or second stage. We recommend cesarean birth rather than manual rotation ( Grade 1C ).
If the fetus is estimated to be larger than the patient’s prior newborns or the patient is nulliparous, we perform cesarean birth early in the labor course. (See 'Labor and delivery management' above.)
● Definition – In brow presentation, the fetal surface presenting in the birth canal extends from the anterior fontanelle to the brow (orbital ridge), but does not include the mouth and chin ( figure 2 ). The fetal neck is extended, but not to the degree of a face presentation. (See 'Definition' above.)
● Diagnosis – The diagnosis of brow presentation is made by vaginal examination. Palpation of the forehead, orbital ridge, orbits, and saddle of the nose, but not the mouth and chin, is diagnostic of brow presentation ( figure 2 ). Ultrasound can be used to confirm or clarify the type of malpresentation if the clinical examination findings are unclear. (See 'Diagnosis' above.)
● Management – Patients with a fetus in brow presentation and a clinically adequate or proven pelvis can undergo a trial of labor, with close monitoring and delivery by cesarean for standard indications. The brow presentation is often a transitional state: 50 percent will spontaneously convert to a face or occipital presentation. Fetuses with persistent brow presentation should be delivered by cesarean since vaginal birth is not possible unless the fetus is very small, the pelvis is very large, or both. Operative vaginal delivery is contraindicated for brow presentation. (See 'Labor and delivery management' above.)
- Gardberg M, Leonova Y, Laakkonen E. Malpresentations--impact on mode of delivery. Acta Obstet Gynecol Scand 2011; 90:540.
- Duff P. Diagnosis and management of face presentation. Obstet Gynecol 1981; 57:105.
- Ducarme G, Ceccaldi PF, Chesnoy V, et al. [Face presentation: retrospective study of 32 cases at term]. Gynecol Obstet Fertil 2006; 34:393.
- Bhal PS, Davies NJ, Chung T. A population study of face and brow presentation. J Obstet Gynaecol 1998; 18:231.
- Cruikshank DP, Cruikshank JE. Face and brow presentation: a review. Clin Obstet Gynecol 1981; 24:333.
- Weissberg SM, O'Leary JA. Compound presentation of the fetus. Obstet Gynecol 1973; 41:60.
- Ingólfsson A. Brow presentations. Acta Obstet Gynecol Scand 1969; 48:486.
- Tapisiz OL, Aytan H, Altinbas SK, et al. Face presentation at term: a forgotten issue. J Obstet Gynaecol Res 2014; 40:1573.
- Zayed F, Amarin Z, Obeidat B, et al. Face and brow presentation in northern Jordan, over a decade of experience. Arch Gynecol Obstet 2008; 278:427.
- Cunningham FG, Leveno KJ, Bloom SL, et al. Williams Obstetrics, 25th ed, McGraw-Hill Education, New York 2018.
- Cruikshank DP, White CA. Obstetric malpresentations: twenty years' experience. Am J Obstet Gynecol 1973; 116:1097.
- Bashiri A, Burstein E, Bar-David J, et al. Face and brow presentation: independent risk factors. J Matern Fetal Neonatal Med 2008; 21:357.
- Shaffer BL, Cheng YW, Vargas JE, et al. Face presentation: predictors and delivery route. Am J Obstet Gynecol 2006; 194:e10.
- Sharshiner R, Silver RM. Management of fetal malpresentation. Clin Obstet Gynecol 2015; 58:246.
- Handa VL, Lockhart ME, Fielding JR, et al. Racial differences in pelvic anatomy by magnetic resonance imaging. Obstet Gynecol 2008; 111:914.
- Işcan MY. Assessment of race from the pelvis. Am J Phys Anthropol 1983; 62:205.
- Patriquin ML, Steyn M, Loth SR. Metric analysis of sex differences in South African black and white pelves. Forensic Sci Int 2005; 147:119.
- Kurki HK, Decrausaz SL. Shape variation in the human pelvis and limb skeleton: Implications for obstetric adaptation. Am J Phys Anthropol 2016; 159:630.
- Bellussi F, Ghi T, Youssef A, et al. The use of intrapartum ultrasound to diagnose malpositions and cephalic malpresentations. Am J Obstet Gynecol 2017; 217:633.
- Lau WL, Cho LY, Leung WC. Intrapartum translabial ultrasound demonstration of face presentation during first stage of labor. J Obstet Gynaecol Res 2011; 37:1868.
- Ghi T, Eggebø T, Lees C, et al. ISUOG Practice Guidelines: intrapartum ultrasound. Ultrasound Obstet Gynecol 2018; 52:128.
- Lauer AK, Rimmer SO. Eyelid laceration in a neonate by fetal monitoring spiral electrode. Am J Ophthalmol 1998; 125:715.
- Miyashiro MJ, Mintz-Hittner HA. Penetrating ocular injury with a fetal scalp monitoring spiral electrode. Am J Ophthalmol 1999; 128:526.
- Cheng BT, Laurenti KD, Kurup SP. Neonatal eyelid penetration from insertion of a fetal scalp electrode: a case report. BMC Pregnancy Childbirth 2022; 22:878.
- Benedetti TJ, Lowensohn RI, Truscott AM. Face presentation at term. Obstet Gynecol 1980; 55:199.
- Schwartz Z, Dgani R, Lancet M, Kessler I. Face presentation. Aust N Z J Obstet Gynaecol 1986; 26:172.
- Westgren M, Svenningsen NW. Face presentation in modern obstetrics--a study with special reference to fetal long term morbidity. Z Geburtshilfe Perinatol 1984; 188:87.
- Vialle R, Piétin-Vialle C, Ilharreborde B, et al. Spinal cord injuries at birth: a multicenter review of nine cases. J Matern Fetal Neonatal Med 2007; 20:435.
- Dennen PC. Dennen's Forceps Deliveries, 3rd edition, FA Davis, Philadelphia 1989. p.127.
- Laufe LE. Obstetric Forceps, Harper & Row, Hagerstown 1968. p.117.
- Yeomans ER, Hoffman BL, Gilstrap LC, Cunningham FG. Operative vaginal delivery. In: Cunningham and Gilstrap's Operative Obstetrics, 3rd ed, McGraw-Hill Education, New York 2017.
- Shabib G, Black, A. Operative vaginal delivery. In: Oxorn-Foote Human Labor and Birth, 6th ed, Posner G (Ed), McGraw-Hill Medical, New York 2013.
- Levy DL. Persistent brow presentation: a new approach to management. South Med J 1976; 69:191.
- Neuman M, Beller U, Lavie O, et al. Intrapartum bimanual tocolytic-assisted reversal of face presentation: preliminary report. Obstet Gynecol 1994; 84:146.
- Williams Obstetrics, 23rd Ed, Cunningham, FG, Leveno, KJ, Bloom, JC, et al (Eds), McGraw-Hill, 2010.
- Vialle R, Piétin-Vialle C, Vinchon M, et al. Birth-related spinal cord injuries: a multicentric review of nine cases. Childs Nerv Syst 2008; 24:79.
- Lau WL, Leung WC, Chin R. Intrapartum translabial ultrasound demonstrating brow presentation during the second stage of labor. Int J Gynaecol Obstet 2009; 107:62.
- Wiafe YA, Whitehead B, Venables H, Nakua EK. The effectiveness of intrapartum ultrasonography in assessing cervical dilatation, head station and position: A systematic review and meta-analysis. Ultrasound 2016; 24:222.
- Jennings PN. Brow presentation with vaginal delivery. Aust N Z J Obstet Gynaecol 1968; 8:219.
- Luker R. Vaginal delivery of two cases of brow presentation using multiple Kiwi Omnicups. J Obstet Gynaecol 2005; 25:601.
1 : Malpresentations--impact on mode of delivery.
2 : Diagnosis and management of face presentation.
3 : [Face presentation: retrospective study of 32 cases at term].
4 : A population study of face and brow presentation.
5 : Face and brow presentation: a review.
6 : Compound presentation of the fetus.
7 : Brow presentations.
8 : Face presentation at term: a forgotten issue.
9 : Face and brow presentation in northern Jordan, over a decade of experience.
10 : Face and brow presentation in northern Jordan, over a decade of experience.
11 : Obstetric malpresentations: twenty years' experience.
12 : Face and brow presentation: independent risk factors.
13 : Face presentation: predictors and delivery route.
14 : Management of fetal malpresentation.
15 : Racial differences in pelvic anatomy by magnetic resonance imaging.
16 : Assessment of race from the pelvis.
17 : Metric analysis of sex differences in South African black and white pelves.
18 : Shape variation in the human pelvis and limb skeleton: Implications for obstetric adaptation.
19 : The use of intrapartum ultrasound to diagnose malpositions and cephalic malpresentations.
20 : Intrapartum translabial ultrasound demonstration of face presentation during first stage of labor.
21 : ISUOG Practice Guidelines: intrapartum ultrasound.
22 : Eyelid laceration in a neonate by fetal monitoring spiral electrode.
23 : Penetrating ocular injury with a fetal scalp monitoring spiral electrode.
24 : Neonatal eyelid penetration from insertion of a fetal scalp electrode: a case report.
25 : Face presentation at term.
26 : Face presentation.
27 : Face presentation in modern obstetrics--a study with special reference to fetal long term morbidity.
28 : Spinal cord injuries at birth: a multicenter review of nine cases.
29 : Spinal cord injuries at birth: a multicenter review of nine cases.
30 : Spinal cord injuries at birth: a multicenter review of nine cases.
31 : Spinal cord injuries at birth: a multicenter review of nine cases.
32 : Spinal cord injuries at birth: a multicenter review of nine cases.
33 : Persistent brow presentation: a new approach to management.
34 : Intrapartum bimanual tocolytic-assisted reversal of face presentation: preliminary report.
35 : Intrapartum bimanual tocolytic-assisted reversal of face presentation: preliminary report.
36 : Birth-related spinal cord injuries: a multicentric review of nine cases.
37 : Intrapartum translabial ultrasound demonstrating brow presentation during the second stage of labor.
38 : The effectiveness of intrapartum ultrasonography in assessing cervical dilatation, head station and position: A systematic review and meta-analysis.
39 : Brow presentation with vaginal delivery.
40 : Vaginal delivery of two cases of brow presentation using multiple Kiwi Omnicups.
آیا می خواهید مدیلیب را به صفحه اصلی خود اضافه کنید؟
اضافه کردن مدیلیب به صفحه اصلی

GFMER Geneva Foundation for Medical Education and Research
- Annual reports
- GFMER members
- Country coordinators
- Obstetric fistula
- Cervical cancer
- Emergency and surgical care
- Picture of the week
- Social media
- Free medical journals
Obstetrics Simplified - Diaa M. EI-Mowafi
Brow Presentation
It is a cephalic presentation in which the head is midway between flexion and extension.
About 1:1000 labour.
As face presentation.
- It is difficult.
- The occiput and sinciput may be felt at the same level.
- Ultrasonography and X-ray may be helpful.
- frontal bones,
- supra-orbital ridges, and
- root of the nose but not the chin.
Mechanism of Labour
- The engagement diameter is the mento-vertical 13.5 cm which is longer than any diameter of the inlet so there is no mechanism of labour and labour is obstructed.
- may occur during conversion of vertex into face presentation. So if brow is flexed to become vertex or extended to become face it may be delivered.
- Exclude contracted pelvis, if present do caesarean section.
- The case is considered as transient brow, observed carefully and given a chance for spontaneous conversion into either face or vertex.
- The rest of management as other malpresentation.
- Caesarean section is done if the foetus is living.
- Craniotomy if the foetus is dead.
- Dystocia : Guidelines, reviews
- Child Health
- Heart Health
- Men's Health
- Mental Health
- Sexual Health
- Skin Conditions
- Travel Vaccinations
- Treatment and Medication
- Women's Health
- View all categories
- Bones and Joints
- Digestive Health
- Healthy Living
- Signs and Symptoms
Try our Symptom Checker Got any other symptoms?
- Nervous System
- Heart Disease
- Inflammation
- Painkillers
- Muscle Pain
- View all Medicines and Drugs
- Type 2 Diabetes
- Bacterial Vaginosis
- View all Treatments
- BMI Calculator
- Pregnancy Due Date Calculator
- Screening Tests
- Blood Tests
- Liver Function Tests
- Am I Pregnant?
- Am I Depressed?
- View all Tools
- Latest Features
- Health Videos
- Bronchiolitis
- Molluscum Contagiosum
- Actinic Keratosis
- Abdominal Pain in Children
- Subdural Haematoma
- Obesity in Adults
- View all Pro Articles
- View all Medical Calculators
- Login / Register
- Patient Access
- Professional Articles
Malpresentations and Malpositions
Remove from Saved
Professional Reference articles are designed for health professionals to use. They are written by UK doctors and based on research evidence, UK and European Guidelines. You may find one of our health articles more useful.
Treatment of almost all medical conditions has been affected by the COVID-19 pandemic. NICE has issued rapid update guidelines in relation to many of these. This guidance is changing frequently. Please visit https://www.nice.org.uk/covid-19 to see if there is temporary guidance issued by NICE in relation to the management of this condition, which may vary from the information given below.
In this article
Malpresentation, malposition.
Usually the fetal head engages in the occipito-anterior position (more often left occipito-anterior (LOA) rather than right) and then undergoes a short rotation to be directly occipito-anterior in the mid-cavity. Malpositions are abnormal positions of the vertex of the fetal head relative to the maternal pelvis. Malpresentations are all presentations of the fetus other than vertex.
Obstetrics - the pelvis and head

Predisposing factors to malpresentation include:
- Prematurity.
- Multiple pregnancy.
- Abnormalities of the uterus - eg, fibroids.
- Partial septate uterus.
- Abnormal fetus.
- Placenta praevia.
- Primiparity.
Breech presentation
See the separate Breech Presentations article for more detailed discussion.
- Breech presentation is the most common malpresentation, with the majority discovered before labour. Breech presentation is much more common in premature labour.
- Approximately one third are diagnosed during labour when the fetus can be directly palpated through the cervix.
- After 37 weeks, external cephalic version can be attempted whereby an attempt is made to turn the baby manually by manipulating the pregnant mother's abdomen. This reduces the risk of non-cephalic delivery [ 1 ] .
- Maternal postural techniques have also been tried but there is insufficient evidence to support these [ 2 ] .
- Many women who have a breech presentation can deliver vaginally. Factors which make this less likely to be successful include [ 3 ] :
- Hyperextended neck on ultrasound.
- High estimated fetal weight (more than 3.8 kg).
- Low estimated weight (less than tenth centile).
- Footling presentation.
- Evidence of antenatal fetal compromise.
Transverse lie [ 4 ]
- When the fetus is positioned with the head on one side of the pelvis and the buttocks in the other (transverse lie), vaginal delivery is impossible.
- This requires caesarean section unless it converts or is converted late in pregnancy. The surgeon may be able to rotate the fetus through the wall of the uterus once the abdominal wall has been opened. Otherwise, a transverse uterine incision is needed to gain access to a fetal pole.
- Internal podalic version is no longer attempted.
- Transverse lie is associated with a risk of cord prolapse of up to 20%.
Occipito-posterior position
- This is the most common malposition where the head initially engages normally but then the occiput rotates posteriorly rather than anteriorly. 5.2% of deliveries are persistent occipito-posterior [ 5 ] .
- The occipito-posterior position results from a poorly flexed vertex. The anterior fontanelle (four radiating sutures) is felt anteriorly. The posterior fontanelle (three radiating sutures) may also be palpable posteriorly.
- It may occur because of a flat sacrum, poorly flexed head or weak uterine contractions which may not push the head down into the pelvis with sufficient strength to produce correct rotation.
- As occipito-posterior-position pregnancies often result in a long labour, close maternal and fetal monitoring are required. An epidural is often recommended and it is essential that adequate fluids be given to the mother.
- The mother may get the urge to push before full dilatation but this must be discouraged. If the head comes into a face-to-pubis position then vaginal delivery is possible as long as there is a reasonable pelvic size. Otherwise, forceps or caesarean section may be required.
Occipito-transverse position
The head initially engages correctly but fails to rotate and remains in a transverse position.
Alternatives for delivery include manual rotation of fetal head using Kielland's forceps, or delivery using vacuum extraction. This is inappropriate if there is any fetal acidosis because of the risk of cerebral haemorrhage.
Therefore, there must be provision for a failure of forceps delivery to be changed immediately to a caesarean. The trial of forceps is therefore often performed in theatre. Some centres prefer to manage by caesarean section without trial of forceps.
Face presentations
- Face presents for delivery if there is complete extension of the fetal head.
- Face presentation occurs in 1 in 1,000 deliveries [ 5 ] .
- With adequate pelvic size, and rotation of the head to the mento-anterior position, vaginal delivery should be achieved after a long labour.
- Backwards rotation of the head to a mento-posterior position requires a caesarean section.
Brow positions
- The fetal head stays between full extension and full flexion so that the biggest diameter (the mento-vertex) presents.
- Brow presentation occurs in 0.14% of deliveries [ 5 ] .
- Brow presentation is usually only diagnosed once labour is well established.
- The anterior fontanelle and super orbital ridges are palpable on vaginal examination.
- Unless the head flexes, a vaginal delivery is not possible, and a caesarean section is required.
Are you protected against flu?
See if you are eligible for a free NHS flu jab today.
Join our weekly wellness digest
from the best health experts in the business
Further reading and references
Hofmeyr GJ, Kulier R, West HM ; External cephalic version for breech presentation at term. Cochrane Database Syst Rev. 2015 Apr 1(4):CD000083. doi: 10.1002/14651858.CD000083.pub3.
Hofmeyr GJ, Kulier R ; Cephalic version by postural management for breech presentation. Cochrane Database Syst Rev. 2012 Oct 1710:CD000051. doi: 10.1002/14651858.CD000051.pub2.
Management of Breech Presentation ; Royal College of Obstetricians and Gynaecologists (Mar 2017)
Szaboova R, Sankaran S, Harding K, et al ; PLD.23 Management of transverse and unstable lie at term. Arch Dis Child Fetal Neonatal Ed. 2014 Jun99 Suppl 1:A112-3. doi: 10.1136/archdischild-2014-306576.324.
Gardberg M, Leonova Y, Laakkonen E ; Malpresentations - impact on mode of delivery. Acta Obstet Gynecol Scand. 2011 May90(5):540-2. doi: 10.1111/j.1600-0412.2011.01105.x.
Related Information
- Dystocia (Causes, Types, and Treatment)
Have had surgery twice for fibroid. One time was laparoscopic. Now surgery has been suggested due to fibroid. No children. Will it affect my uterus? Another surgery if I am pregnant Does anyone have... prasy86293
Feeling unwell?
Assess your symptoms online with our free symptom checker.
Disclaimer: This article is for information only and should not be used for the diagnosis or treatment of medical conditions. Egton Medical Information Systems Limited has used all reasonable care in compiling the information but make no warranty as to its accuracy. Consult a doctor or other health care professional for diagnosis and treatment of medical conditions. For details see our conditions .
- Vishal's account
- Complications
Brow Presentation – An Overview

What Is Brow Presentation?
How can you get to know if your baby is in this position, what are the causes of brow presentation, how is the diagnosis made, complications of brow presentation delivery, alternatives for labor during brow presentation, precautions to take before and after labour, how will brow presentation affect your baby during labor.
Pregnancy is a beautiful experience that is also fraught with a host of complications and risks. One of them concerns the normal orientation of your baby inside your uterus, which is essential for a smooth delivery. This article will explain all about abnormal forehead presentation and its associated causes, complications, diagnosis, treatment and precautions.
Babies assume a fixed position in the uterus, that is with their chins tucked firmly into their chests. This position is ideal to exit the uterus smoothly. However, in some cases, the baby’s head and neck will extend backwards away from their chest. This is known as a brow presentation or forehead presentation. It is an extremely rare condition, occurring once in 1500 births. Brow presentation might obstruct vaginal births from occurring as there is less space for the baby to drop down towards the pelvic girdle. However, if brow presentation occurs early in labour, there is still time for them to flex their neck back to the right position. If not, labour might be hindered, causing stress for both, the mother and the baby. In these instances, your doctor might recommend a caesarean section. A brow baby tends to occur in women pregnant for the second or third time, or due to physical defects like an abnormally developed spine.
Brow babies are rarely detected before labor begins, but around half of them will shift to a face-first or crown-first presentation suitable for delivery. A brow presentation delivery will take much longer than normal, which is usually when the condition is discovered.
There are several potential reasons for your baby to assume this orientation. Some of them are:
- Fetal Size: Babies born preterm, or with low birth weights, raise the likelihood of them presenting brow first. This is also observed in large babies, who usually flex their head outwards rather than in towards their chest. Brow presentation can also be caused if your pelvic girdle and your baby’s head are disproportionate to each other.
- Polyhydramnios: Polyhydramnios is the condition in which there is too much amniotic fluid in your uterus. Thus, it might be tricky for your baby to fix their heads in the correct position.
- Multiple Pregnancy: Carrying twins or more in your womb decreases the amount of space available, making your babies take alternative positions to fit properly.
- Maternal Defects: If your pelvis is not the right shape and size, it might be difficult for your fetus to assume normal presentations. The most common cause of brow presentation is the triangle-shaped android pelvis and the atypically small contracted pelvis. Another maternal defect is a lax uterus, which is not firm enough to hold the baby in place, resulting in different presentations.
- Fetal Defects: If your baby has conditions such as anencephaly and hydrocephalus, their abnormally large heads will not be able to take the right position.
To diagnose brow presentation, an experienced doctor will be able to help. Ultrasound scans are compulsory for monitoring the situation. Your doctor might even conduct a digital examination to check the orientation of the baby’s facial features. If they find that the baby’s head does not rotate enough for a natural birth, they might recommend a caesarean section.
Several risks come with brow presentation birth. Some of them are:
- Labor time might be extended as the baby would have a hard time getting past the pelvis.
- Forceps might be required, which could cause cranial damage.
- Baby’s head shape might be altered due to difficulty while moving through the birth canal.
- Baby may go through stress during delivery as it would be difficult birth and may require a caesarean.
- Injuries may occur to the baby’s spinal cord due to trauma.
- Increased risk of cerebral hemorrhage in the baby as the head may take in damage.
As explained already, a baby in brow presentation might not have enough space to move downwards towards the cervix. If this happens, there are a few methods your doctor might implement to reduce the complications of natural birth. These methods require medical skill and enough space within the cervix to be attempted.
- Ventouse Birth: In this case, your doctor will use a small vacuum extraction device known as a ventouse to pull the baby’s head towards their chest. This method can be used even after you have begun to push.
- Manual Rotation: After the cervix undergoes complete dilation, your doctor might attempt to move the baby’s head into the correct position using their hands.
As there are several complications linked with brow presentations, here are some precautions for you to take before and after labour to have a successful pregnancy.
- Choose a doctor who is accomplished in obstetrics and gynaecology, so they are experienced in dealing with any potential outcome.
- Visit your doctor regularly, especially at the end of your third trimester.
- If you have been diagnosed with brow presentation, do not hesitate to go for a caesarean if strongly recommended by your doctor, as it dramatically reduces the risks involved.
Babies might end up with abnormally shaped heads if they go through vaginal birth with a brow presentation. However, as their heads are malleable, they will return to a normal shape in a few days. Extended labor might cause stress in your baby who has been stuck in an uncomfortable position the whole time. This might also lead to vertebral problems, so consult a paediatric osteopath if you are concerned.
Brow presentation can happen to anyone, so not encountering it in your first pregnancy does not mean you will not see during later pregnancies. Consume a balanced, nutritious diet, stay hydrated and get enough sleep. Avoiding tension and anxiety will help you stay strong for when your baby arrives.
Also Read : Preparing for Labour & Delivery – Smart Ways to Prepare for Childbirth

- RELATED ARTICLES
- MORE FROM AUTHOR

Depression After Miscarriage - Signs and Tips to Deal With It
 During Pregnancy")
8 Home Remedies for a Urinary Tract Infection (UTI) During Pregnancy

Incomplete Miscarriage - Causes, Symptoms and Treatment

This Mother Wishes Her Child Dies At Birth. The Reason Will Shock and Sadden You...

Why Should You Visit a Gynaecologist?

Cervical Incompetence
Popular on parenting.

245 Rare Boy & Girl Names with Meanings

Top 22 Short Moral Stories For Kids

170 Boy & Girl Names That Mean 'Gift from God'

800+ Unique & Cute Nicknames for Boys & Girls
Latest posts.

Cookie Monster Coloring Pages - Free Printable Pages For Kids

Robot Coloring Pages - Free Printable Pages For Kids

Cheerleading Coloring Pages - Free Printable Pages For Kids

Essay On Holi - 10 lines, Short and Long Essay for Students and Children
Abnormal Fetal Position and Presentation
Under normal circumstances, a baby is in the vertex (cephalic) position before delivery. In the vertex position, the baby’s head is at the lower part of the abdomen, and the baby is born head-first. However, some babies present differently before delivery. In these cases, abnormal presentations may place the baby at risk of experiencing umbilical cord problems and/or a birth trauma (1). Types of abnormal fetal positions and presentations include the following. We’ll cover each in more detail on this page.
What is the difference between fetal presentation and position?
In the womb, a fetus has both a presentation and a position . Presentation refers to the baby’s body that leads, or is expected to lead, out of the birth canal (9). For example, if a baby’s rear is set to come out of the birth canal first, the baby is said to be in “breech presentation.” Position refers to the direction the baby is facing in relation to the mother’s spine (9). A baby could be lying face-first against a mother’s spine, or face up towards the mother’s belly.
What way should a baby come out during birth?
Vertex presentation is the ‘normal’ way that a baby is positioned for birth and the lowest-risk presentation for vaginal birth (1). In vertex presentation, the baby is positioned head-first with their occiput (the part of the head close to the base of the skull) entering the birth canal first. In this position, the baby’s chin is tucked into their chest and they are facing the mother’s back (occipito-anterior position). Any position other than vertex position is abnormal and can make vaginal delivery much more difficult or sometimes impossible (2). If a baby’s chin isn’t tucked into their chest, they may come out face-first (face presentation), which can cause birth injury (1).
What happens if a baby isn’t in the standard vertex position during birth?
Before delivery, it is critical that the fetus is in the standard vertex presentation and within the normal range for weight and size. This helps ensure the safety of both baby and mother during labor. When the baby’s size or position is abnormal, physician intervention is usually warranted (1). This may mean simple manual procedures to help reposition the baby or, in many cases, a planned C-section delivery . The failure of healthcare professionals to identify and quickly resolve issues related to fetal size, weight, and presentation is medical malpractice . There are numerous complications related to abnormal weight, size, abnormal position, or abnormal presentation.
Compound presentation
In the safest presentation (vertex presentation), the baby is born head first, with the rest of the body following. In a compound presentation, however, there are multiple presenting parts. Most commonly, this means that the baby’s head and an arm come out first at the same time. Sometimes compound presentation can occur with twins where the head of the first twin presents with the extremity of the second twin (3).
Risk factors for compound presentation include (3):
- Prematurity
- Intrauterine growth restriction (IUGR)
- Multiple gestations ( twins , triplets, etc.)
- Polyhydramnios
- A large pelvis
- External cephalic version
- Rupture of membranes at high station
Compound presentations can be detected via ultrasound before the mother’s water breaks. During labor, compound presentation is identified as an irregular finding during a cervical examination (3).
If a mother has polyhydramnios, the risk of compound presentation is higher, as the flow of amniotic fluid when the membranes rupture can sweep extremities into the birth canal, or cause a cord prolapse , which is a medical emergency (3). If compound presentation continues, it is likely to cause dystocia (the baby becoming stuck in the birth canal), which is also a medical emergency (3). Often, the safest way to deliver a baby with compound presentation is C-section, because complications like dystocia and cord prolapse carry risks of severe adverse outcomes, including cerebral palsy , intellectual and developmental disabilities, and hypoxic-ischemic encephalopathy (HIE) (3).
Limb presentation
Limb presentation during childbirth means that the part of the baby’s body that emerges first is a limb – an arm or a leg. Babies with limb presentation cannot be delivered safely via vaginal delivery; they must be delivered quickly by emergency C-section (4). Limb presentation poses a large risk for dystocia (the baby getting stuck on the mother’s pelvis), which is a medical emergency.
Occipitoposterior (OP) position
Approximately 1 out of 19 babies present in a posterior position rather than an anterior position. This is called an occipitoposterior (OP) position or occiput posterior position (3) In OP position, the baby is head-first with the back part of the head turned towards the mother’s back, rotated to the right (right occipitoposterior position, or ROP), or to the left (left occipitoposterior position, or LOP) of the sacroiliac joint. Occipitoposterior position increases the baby’s risk of experiencing prolonged labor , prolapsed umbilical cord , and use of delivery instruments, such as forceps and vacuum extractors (5). These conditions can cause brain bleeds , a lack of oxygen to the brain, and birth asphyxia .
When OP position is present, if a manual rotation cannot be quickly and effectively performed in the face of fetal distress, the baby should be delivered via C-section (5). A C-section can help prevent oxygen deprivation caused by prolonged labor, umbilical cord prolapse, or forceps and vacuum extractor use.
A nurse explains posterior position
Breech presentation
Breech presentation is normal throughout pregnancy. However, by the 37th week, the baby should turn to the cephalic position in time for labor. Breech presentation occurs when a baby’s buttocks or legs are positioned to descend the birth canal first. Breech positions are dangerous because when vaginal delivery is attempted, a baby is at increased risk for prolapsed umbilical cord, traumatic head injury, spinal cord fracture, fatality, and other serious problems with labor (6).
There are 4 types of breech positions:
- Footling breech presentation : In footling position, one or both feet enter the birth canal first, with the buttocks at a higher position than the feet.
- Kneeling breech presentation : This is when the baby has one or both legs extended at the hips and flexed at the knees.
- Frank breech presentation : This is when the baby’s buttocks present first, the legs are flexed at the hip and extended at the knees, and the feet are near the ears.
- Complete breech presentation : In this position, the baby’s hips and knees are flexed so that the baby is sitting cross-legged, with the feet beside the buttocks.
When a baby is in breech position, physicians often try to maneuver the baby into a head-first position. This should only be attempted if fetal heart tracings are normal (the baby is not in distress ) (7). The only type of breech position that may allow for a vaginal delivery is frank breech , and the following conditions must be met:
- The baby’s heart rate is being closely monitored and the baby is not in distress.
- Cephalopelvic disproportion (CPD) is not present; x-rays and ultrasound show that the size of the mother’s pelvis will allow a safe vaginal birth.
- The hospital is equipped for and the physician is skilled in performing an emergency C-section .
If these conditions are not present, vaginal birth should not be attempted. Most experts recommend C-section delivery for all types of breech positions because it is the safest method of delivery and it helps avoid birth injuries (6). Mismanaged breech birth can result in the following conditions:
- Brain bleeds, intracranial hemorrhages
- Spinal cord fractures
- Hypoxic-ischemic encephalopathy (HIE)
- Cerebral palsy
- Intellectual disabilities
- Developmental delays
Face presentation
A face presentation occurs when the face is the presenting part of the baby. In this position, the baby’s neck is deflexed (extended backward) so that the back of the head touches the baby’s back. This prevents head engagement and descent of the baby through the birth canal. In some cases of face presentation, the trauma of a vaginal delivery causes face deformation and fluid build-up (edema) in the face and upper airway, which often means the baby will need a breathing tube placed in the airway to maintain airway patency and assist breathing (1).
Image by healthhand.com
There are three types of face presentation:
- Mentum anterior (MA) : In this position, the chin is facing the front of the mother.
- Mentum posterior (MP) : The chin is facing the mother’s back, pointing down towards her buttocks in mentum posterior position. In this position, the baby’s head, neck, and shoulders enter the pelvis at the same time, and the pelvis is usually not large enough to accommodate this. Also, an open fetal mouth can push against the bone (sacrum) at the upper and back part of the pelvis, which also can prevent descent of the baby through the birth canal.
- Mentum transverse (MT) : The baby’s chin is facing the side of the birth canal in this position.
Trauma is very common during vaginal delivery of a baby in face presentation, so parents must be warned that their baby may be bruised and that a C-section is available to avoid this trauma.
Babies presenting face-first can sometimes be delivered vaginally, as long as the baby is in MA position (1). Safe vaginal delivery of a term-sized infant in persistent MP position is impossible due to the presenting part of the baby compared to the size of the mother’s pelvis (1). Babies in MP position must be delivered by C-section. Babies in MT position must also be delivered by C-section. Some babies in the MP and MT positions will spontaneously convert to the MA position during the course of labor, which makes vaginal delivery a possibility. If the baby is in the MA position and vaginal delivery is able to proceed, engagement of the presenting part of the baby probably will not occur until the face is at a +2 station (1).
The management of face presentation requires close observation of the progress of labor due to the high incidence of CPD with face presentation. In face presentation, the diameter of the presenting part of the head is, on average, 0.7 cm greater than in the normal vertex position (1).
In any face presentation situation, if progress in dilation and descent ceases despite adequate contractions, delivery must occur by C-section. In fact, when face presentation occurs, experts recommend liberal use of C-section (1).
Since there is an increased risk of trauma to the baby when the face presents, the physician should not try to rotate the baby internally. In addition, the physician must not use vacuum extractors or manual extraction (grasping the baby with hands) to extract the baby from the uterine cavity. Outlet forceps should only be used by experienced physicians; these forceps increase the risk of trauma and brain bleeds. In almost all clinical circumstances a cesarean delivery is the safest method of delivery.
Listed below are complications that can occur if face presentation is mismanaged by the medical team:
- Prolonged labor
- Facial trauma
- Facial and upper airway edema (fluid build-up in the face, often caused by trauma)
- Skull molding (abnormal head shape that results from pressure on the baby’s head during childbirth)
- Respiratory distress or difficulty in ventilation (the baby being able to move air in and out of lungs) due to upper airway trauma and edema
- Spinal cord injury
- Abnormal fetal heart rate patterns
- 10-fold increase in fetal compromise
- Brain bleeds
- Intracranial hemorrhages
- Permanent brain damage
Brow presentation
Brow presentation is similar to face presentation, but the baby’s neck is less extended. A fetus in brow presentation has the chin untucked, and the neck is extended slightly backward. As the term “brow presentation” suggests, the brow (forehead) is the part that is situated to go through the pelvis first. Vaginal delivery can be difficult or impossible with brow presentation, because the diameter of the presenting part of the head may be too big to safely fit through the pelvis.
Risk factors and conditions associated with brow presentation
Brow presentation has been linked to several risk factors and co-occurring conditions. These include:
- Multiparity (having previously given birth)
- Premature delivery
- Fetal anomalies such as anencephaly (an absence of major parts of the brain and skull) or anterior neck mass (a growth on the front of the neck)
- Previous c-section delivery
- Polyhydramnios (excessive amniotic fluid: infants swallow amniotic fluid while in utero, but this may be difficult if their neck is extended)
Diagnosis of brow presentation
Brow presentation can often be diagnosed through a vaginal examination during labor. If there are no conclusive signs from the physical examination alone, an ultrasound can also be used. Warning signs of brow presentation may include signs of fetal distress or lack of labor progression.
Management of brow presentation
Infants who assume a brow presentation early in labor may spontaneously move into a more optimal position during the delivery process. Additionally, safe delivery in brow presentation may be possible if the infant is unusually small and/or the mother’s pelvic opening is unusually large. For these reasons, physicians occasionally recommend vaginal delivery of infants in brow presentation.
Doctors attempting vaginal delivery of a baby in brow presentation must be very careful to watch for signs of fetal distress (such as an abnormal heart rate), and to monitor the progression of labor. Prolonged labor can cause extended periods of fetal oxygen deprivation, which can cause birth asphyxia and permanent injury. Signs of fetal distress can indicate that a baby is in danger of sustaining serious brain damage if action is not quickly taken to prevent this. If an infant in brow presentation begins to show signs of distress, or if labor progress stops or slows significantly, physicians should be ready to move on to a cesarean delivery.
Labor induction or augmentation with the drug Pitocin (synthetic oxytocin) is very dangerous in cases of brow presentation. Pitocin can lead to excessive uterine contractions, which can put pressure on the infant’s head and cut off their oxygen supply; this is especially risky when safe fetal descent is already compromised, such as in cases of brow presentation.
Complications of brow presentation
If brow presentation is diagnosed in a timely fashion and is appropriately managed, there are typically no serious negative effects on the mother or baby. However, if medical professionals fail to recognize brow presentation and intervene as necessary, there can be lasting consequences. Infants may suffer oxygen deprivation due to prolonged labor, or traumatic injuries from a difficult delivery. Some of the most severe conditions resulting from mismanaged brow presentation births include:
- Hypoxic-ischemic encephalopathy
- Periventricular leukomalacia
- Seizure disorders
- Developmental disabilities
Shoulder presentation (transverse lie)
Shoulder presentation (transverse lie) is when the arm, shoulder or trunk of the baby enter the birth canal first. When a baby is in a transverse lie position during labor, C-section is almost always used as the delivery method (8). Mothers who have polyhydramnios (too much amniotic fluid), are pregnant with more than one baby, have placenta previa, or have a baby with intrauterine growth restriction (IUGR) are more likely to have a baby in the transverse lie position (8). Once the membranes rupture, there is an increased risk of umbilical cord prolapse in this position; thus, a C-section should ideally be performed before the membranes break (8). Failure to quickly deliver the baby by C-section when transverse lie presentation is present can cause severe birth asphyxia due to cord compression and trauma to the baby. This can cause hypoxic-ischemic encephalopathy (HIE), seizures, permanent brain damage, and cerebral palsy.
Legal help for birth injuries from abnormal position or presentation
The award-winning birth injury attorneys at ABC Law Centers have over 100 years of joint experience handling birth trauma cases related to abnormal position or presentation. If you believe your loved one’s birth injury resulted from an instance of medical malpractice, you may be entitled to compensation from a medical malpractice or personal injury case. During your free legal consultation, our birth injury attorneys will discuss your case with you, determine if negligence caused your loved one’s injuries, identify the negligent party, and discuss your legal options with you.
- Free Case Review
- Available 24/7
- No Fee Unless We Win
Featured Videos
Testimonial from keziah’s family, posterior position, hypoxic-ischemic encephalopathy (hie).
Featured Testimonial
What Our Clients Say…
After the traumatic birth of my son, I was left confused, afraid, and seeking answers. We needed someone we could trust and depend on . ABC Law Centers was just that.
Helpful resources
More about our firm.
- Meet our birth injury attorneys
- Meet our in-house medical staff
- Verdicts and settlements
- Testimonials
- Julien, S., and Galerneau, F. (2017). Face and brow presentations in labor. Retrieved from https://www.uptodate.com/contents/face-and-brow-presentations-in-labor .
- World Health Organization, UNICEF, and United Nations Population Fund. Malpositions and malpresentations. Retrieved from http://hetv.org/resources/reproductive-health/impac/Symptoms/Malpositions__malpresetations_S69_S81.html .
- Barth, W. (2016). Compound fetal presentation. Retrieved from https://www.uptodate.com/contents/compound-fetal-presentation .
- Gabbe, S.G., … Grobman, W.A. (2017). Compound Presentation. Retrieved from https://expertconsult.inkling.com/read/gabbe-obstetrics-normal-problem-pregnancies-7e/chapter-17/compound-presentation .
- Argani, C.H. and Satin, A.J. (2018) Occiput posterior position. Retrieved from https://www.uptodate.com/contents/occiput-posterior-position .
- Hofmeyr, G.J. (2018). Overview of issues related to breech presentation. Retrieved from https://www.uptodate.com/contents/overview-of-issues-related-to-breech-presentation .
- Hofmeyr, G.J. (2017). Delivery of the fetus in breech presentation. Retrieved from https://www.uptodate.com/contents/delivery-of-the-fetus-in-breech-presentation .
- Strauss, R.A. (2017). Transverse fetal lie. Retrieved from https://www.uptodate.com/contents/transverse-fetal-lie .
- Moldenhauer, J.S. (2018). Abnormal Position and Presentation of the Fetus. Retrieved from https://www.merckmanuals.com/home/women-s-health-issues/complications-of-labor-and-delivery/abnormal-position-and-presentation-of-the-fetus .
Over $350 Million Recovered
In Verdicts, Settlements, & Judgements
$4.75 Million
$3.9 Million
$5.85 Million
Awards & Memberships
- Planning and Preparing
- Trying to Conceive
- Infertility
- Pregnancy Week by Week
- Prenatal Care
- Signs & Symptoms
- Labour & Delivery
- Complications
- Diet & Nutrition
- Postnatal Care
- Development Month by Month
- Vaccination Schedule
- Breastfeeding
- Food & Nutrition
- Baby Sleep Basics
- Play & Activities
- Behavior & Discipline
- Development
- Contest & Winners
- Child Vaccination & Growth Tracker
- Breastfeeding Tracker
- Baby Teething
- Baby Kick Counter
- Due Date Calculator
- Baby Size Comparison
- Week by Week Fetal Development
- Fetal Development Video
- Period & Ovulation Calculator
Brow Presentation – An Overview

In this Article
What is Brow Presentation?
How can you get to know if your baby is in this position, what are the causes of brow presentation, how is the diagnosis made, complications of brow presentation delivery, alternative for labour during brow presentation, precautions to take before and after labour, how will brow presentation affect your baby during labour.
Pregnancy is a beautiful experience that is also fraught with a host of complications and risks. One of them concerns the normal orientation of your baby inside your uterus, which is essential for a smooth delivery. This article will explain all about abnormal forehead presentation and its associated causes, complications, diagnosis, treatment and precautions.
Babies assume a fixed position in the uterus, that is with their chins tucked firmly into their chests. This position is ideal to exit the uterus smoothly. However, in some cases, the baby’s head and neck will extend backwards away from their chest. This is known as a brow presentation or forehead presentation. It is an extremely rare condition, occurring once in 1500 births. Brow presentation might obstruct vaginal births from occurring as there is less space for the baby to drop down towards the pelvic girdle. However, if brow presentation occurs early in labour, there is still time for them to flex their neck back to the right position. If not, labour might be hindered, causing stress for both, the mother and the baby. In these instances, your doctor might recommend a caesarean section. A brow baby tends to occur in women pregnant for the second or third time, or due to physical defects like an abnormally developed spine.
Brow babies are rarely detected before labour begins, but around half of them will shift to a face first or crown first presentation suitable for delivery. A brow presentation delivery will take much longer than normal, which is usually when the condition is discovered.
There are several potential reasons for your baby to assume this orientation. Some of them are:
- Foetal Size: Babies born preterm, or with low birth weights, raise the likelihood of them presenting brow first. This is also observed in large babies, who usually flex their head outwards rather than in towards their chest. Brow presentation can also be caused if your pelvic girdle and your baby’s head are disproportionate to each other.
- Polyhydramnios: Polyhydramnios is the condition in which there is too much amniotic fluid in your uterus. Thus, it might be tricky for your baby to fix their heads in the correct position.
- Multiple Pregnancy: Carrying twins or more in your womb decreases the amount of space available, making your babies take alternative positions to fit properly.
- Maternal Defects: If your pelvis is not the right shape and size, it might be difficult for your foetus to assume normal presentations. The most common cause of brow presentation is the triangle-shaped android pelvis and the atypically small contracted pelvis. Another maternal defect is a lax uterus, which is not firm enough to hold the baby in place, resulting in different presentations.
- Foetal Defects: If your baby has conditions such as anencephaly and hydrocephalus, their abnormally large heads will not be able to take the right position.
to diagnose brow presentation, an experienced doctor will be able to help. Ultrasound scans are compulsory for monitoring the situation. Your doctor might even conduct a digital examination to check the orientation of the baby’s facial features. If they find that the baby’s head does not rotate enough for a natural birth, they might recommend a caesarean section.

Several risks come with brow presentation birth. Some of them are:
- Labour time might be extended as the baby would have a hard time getting past the pelvis.
- Forceps might be required, which could cause cranial damage
- Baby’s head shape might be altered due to difficulty while moving through the birth canal
- Baby may go through stress during delivery as it would be difficult birth and may require a caesarean.
- Injuries may occur to the baby’s spinal cord due to trauma
- Increased risk of cerebral haemorrhage in the baby as the head may take in damage
As explained already, a baby in brow presentation might not have enough space to move downwards towards the cervix. If this happens, there are a few methods your doctor might implement to reduce the complications of natural birth. These methods require medical skill and enough space within the cervix to be attempted.
- Ventouse Birth: In this case, your doctor will use a small vacuum extraction device known as a ventouse to pull the baby’s head towards their chest. This method can be used even after you have begun to push.
- Manual Rotation: After the cervix undergoes complete dilation, your doctor might attempt to move the baby’s head into the correct position using their hands.

- Choose a doctor who is accomplished in obstetrics and gynaecology, so they are experienced in dealing with any potential outcome.
- Visit your doctor regularly, especially at the end of your third trimester.
- If you have been diagnosed with brow presentation, do not hesitate to go for a caesarean if strongly recommended by your doctor, as it dramatically reduces the risks involved.
Babies might end up with abnormally shaped heads if they go through vaginal birth with a brow presentation. However, as their heads are malleable, they will return to normal shape in a few days. Extended labour might cause stress in your baby who has been stuck in an uncomfortable position the whole time. This might also lead to vertebral problems, so consult a paediatric osteopath if you are concerned.
Brow presentation can happen to anyone, so not encountering it in your first pregnancy does not mean you will not see during later pregnancies. Consume a balanced, nutritious diet, stay hydrated and get enough sleep. Avoiding tension and anxiety will help you stay strong for when your baby arrives.
RELATED ARTICLES MORE FROM AUTHOR
10 pregnancy care tips during winter season, 10 tips to stay healthy during a summer pregnancy, skin care & hygiene essentials for your newborn, keep these 56 things handy when your newborn arrives, coronavirus vs the common flu – this is what doctors want you to know, infant head circumference – age by age chart.
The Federal Register
The daily journal of the united states government, request access.
Due to aggressive automated scraping of FederalRegister.gov and eCFR.gov, programmatic access to these sites is limited to access to our extensive developer APIs.
If you are human user receiving this message, we can add your IP address to a set of IPs that can access FederalRegister.gov & eCFR.gov; complete the CAPTCHA (bot test) below and click "Request Access". This process will be necessary for each IP address you wish to access the site from, requests are valid for approximately one quarter (three months) after which the process may need to be repeated.
An official website of the United States government.
If you want to request a wider IP range, first request access for your current IP, and then use the "Site Feedback" button found in the lower left-hand side to make the request.
IMAGES
COMMENTS
The term presentation describes the leading part of the fetus or the anatomical structure closest to the maternal pelvic inlet during labor. The presentation can roughly be divided into the following classifications: cephalic, breech, shoulder, and compound. Cephalic presentation is the most common and can be further subclassified as vertex, sinciput, brow, face, and chin.
There are several complications associated with a brow presentation if vaginal delivery is attempted without proper measures. Increased chances of spinal cord injury are associated with brow presentation. Fetal distress. Abnormal shape of the baby's head after delivery. Prolonged labor.
The vast majority of fetuses at term are in cephalic presentation. Approximately 5 percent of these fetuses are in a cephalic malpresentation, such as occiput posterior or transverse, face ( figure 1A-B ), or brow ( figure 2) [ 1 ]. Diagnosis and management of face and brow presentations will be reviewed here.
In the brow presentation, the occipitomental diameter, which is the largest diameter of the fetal head, is the presenting portion. Descent and internal rotation occur only with an adequate pelvis and if the face can fit under the pubic arch. While the head descends, it becomes wedged into the hollow of the sacrum. ...
Brow Presentation: Definition: Brow presentation occurs when the baby's head is partially extended, causing the brow (forehead) to lead the way through the birth canal. Causes: Brow presentation may result from abnormal fetal positioning, poor engagement of the fetal head, or other factors that prevent full flexion or extension.
Brow presentation is a rare complication, which affects only one in every 500 to one in every 1,400 births. So the chances of it happening are low. If a brow presentation is picked up in early labour, your baby may still flex her head in time for the birth. Alternatively, she may tip her head further back and be born face first.
7.10.1 Diagnosis. 7.10.2 Management. Foetus alive. Foetus dead. Brow presentation constitutes an absolute foeto-pelvic disproportion, and vaginal delivery is impossible (except with preterm birth or extremely low birth weight). This is an obstetric emergency, because labour is obstructed and there is a risk of uterine rupture and foetal distress.
In brow presentation, the neck is moderately arched so that the brow presents first. Usually, fetuses do not stay in a face or brow presentation. These presentations often change to a vertex (top of the head) presentation before or during labor. If they do not, a cesarean delivery is usually recommended.
Brow presentation is considered the rarest of all malpresentation with a prevalence of 1 in 500 to 1 in 4000 deliveries. Both face and brow presentations occur due to extension of the fetal neck instead of flexion; therefore, conditions that would lead to hyperextension or prevent flexion of the fetal neck can all contribute to face or brow ...
Brow Presentation: Brow is a cephalic deflection malpresentation with the partially deflexed fetal head midway between complete flexion (vertex) and full extension (face) (Fig. 2 ). The frontal bone is the designated point for its position in maternal pelvis. On vaginal examination, the brow, orbits, and root of the nose are palpable.
Abnormal presentations include face, brow, breech, and shoulder. Occiput posterior position (facing toward the pregnant patient's pubic bone) is less common than occiput anterior position. Key Points . If a fetus is in the occiput posterior position, operative vaginal delivery or cesarean delivery is often required.
Definition — Brow presentation refers to a presentation in which the fetal surface presenting in the birth canal extends from the anterior fontanelle to the brow (orbital ridge), but does not include the mouth and chin . The fetal neck is extended, but not to the degree of a face presentation. ...
Brow Presentation. It is a cephalic presentation in which the head is midway between flexion and extension. About 1:1000 labour. As face presentation. It is difficult. The occiput and sinciput may be felt at the same level. Ultrasonography and X-ray may be helpful. root of the nose but not the chin. The engagement diameter is the mento-vertical ...
Brow positions. The fetal head stays between full extension and full flexion so that the biggest diameter (the mento-vertex) presents. Brow presentation occurs in 0.14% of deliveries . Brow presentation is usually only diagnosed once labour is well established. The anterior fontanelle and super orbital ridges are palpable on vaginal examination.
Cephalo pelvic disproportion has been associated with brow presentation in from 7.7 to 53.8 per cent of cases,l' 8-12, 15, 19, 20 but the impor-tance of this factor has been doubted by some.21, 22 Leiomyomas of the uterus10, 19 and bicornuate uterus19 have been reported to be associated with the abnormal presentation.
The diagnosis of brow presentation is made by vaginal examination. The posterior fontanelle, mouth, and chin cannot be palpated in the brow presentation. Ultrasound to exclude major anomalies or macrosomia should be considered. The position is defined using the anterior fontanelle as the reference point (ie, frontum anterior or frontum posterior).
Brow presentation might obstruct vaginal births from occurring as there is less space for the baby to drop down towards the pelvic girdle. However, if brow presentation occurs early in labour, there is still time for them to flex their neck back to the right position. If not, labour might be hindered, causing stress for both, the mother and the ...
A fetus in brow presentation has the chin untucked, and the neck is extended slightly backward. As the term "brow presentation" suggests, the brow (forehead) is the part that is situated to go through the pelvis first. Vaginal delivery can be difficult or impossible with brow presentation, because the diameter of the presenting part of the ...
This is known as a brow presentation or forehead presentation. It is an extremely rare condition, occurring once in 1500 births. Brow presentation might obstruct vaginal births from occurring as there is less space for the baby to drop down towards the pelvic girdle. However, if brow presentation occurs early in labour, there is still time for ...
brow presentation: presentation of any part of the fetal head, usually the upper and back part, as a result of flexion such that the chin is in contact with the thorax in vertex presentation; there may be degrees of flexion so that the presenting part is the large fontanel in sincipital presentation, the brow in brow presentation, or the face ...
Define brow presentation. brow presentation synonyms, brow presentation pronunciation, brow presentation translation, English dictionary definition of brow presentation. brow presentation. Translations. English: brow pre·sen·ta·tionn. presentación frontal del feto.
Revise the definition for the White category to remove references to MENA, ... Similarly, with respect to tabulation and presentation, the seven minimum race and ethnicity categories shall also be treated co-equally, which means that when tabulating and presenting data, agencies may not use different tabulation approaches or rules for different ...
The high-definition release with a screen-filling presentation brings to life the gritty world of pro wrestling with a welcome clarity in the ring as the production design reproduces the grit of ...