| - Term used to describe an animal born in a helpless state, with incomplete development of sensory systems at birth. For example rats and mice are born with incomplete development of visual and auditory systems. (More? ) - Term used to describe an anatomical dilation of a tube or canal lumen. Anatomical description of the opening end of the uterine tube lying above the ovary and the enlarged initial segmeny of the semicircular canals of the inner ear vestibular system. (More? ) - (Greek, = a widening, aneurysm) A term used to describe an abnormal widening of a vessel or anatomical tubal structure. - see vestibular aqueduct (More? ) - (AN) abnormality of transmission of sound information to the brain. - (eustachian tube) between the middle ear and oral cavity, has a bony (tympanic 1/3) and cartilaginous (pharyngeal 2/3) portion. The main role is equalization of pressure and fluid drainage in the middle ear. (More? ) - see hillock (More? ) - narrowing, usually of an anatomical tube or cavity. - (Greek, auto = self, phagy = eating, also called autophagy) a cell death mechanism that uses the cell's own lysosomes to self digest. - columnar cells within the organ of Corti on the medial portion of the basilar membrane. (More? ) - (ductus reuniens, canaliculus reuniens, canalis reuniens, Hensen's canal, Hensen's duct, uniting canal, canalis reuniens of Hensen) short narrow canal connecting the cochlea duct to the saccule. (Victor Hensen, 1835-1924) (More? ) - (ear wax) produced by glands in the skin of the outer portion of the ear canal. (More? ) - the developmental differentiation of cartilage from mesenchye, an embryonic connective tissue. - located in the ampulla of the membranous semicircular canals a region with both supporting and hair cells. The hair cell cilia are embedded in the gelatinous cupula. (More? ) - (cells of Claudius) columnar cells with microvilli overlying the basilar membrane and extend from Hensen's cells to the spiral prominence. Barrier cells that lie external to the organ of corti in endolymph. (More? ) - embryonic structure, which will form the coiled cochlear duct and contribute to the saccule. (More? ) - a bony channel containing the fibrous periotic duct. It connects the basal turn of the cochlea perilymphatic space with the subarachnoid space of the posterior cranial cavity. (More? ) - major constituent of the inner ear extracellular matrix. (More? ) - major constituent of the inner ear extracellular matrix. (More? ) - term used to describe one of the two major classes of hearing loss involving external and middle ear abnormalities (other form is Sensorineural loss). - channel proteins of the gap junctions that allow rapid communication between adjacent cells. The two connexins Cx26 and Cx30 are the major proteins of cochlear gap junctions. - A strikingly high proportion (50%) of congenital bilateral nonsyndromic sensorineural deafness cases have been linked to mutations in the GJB2 coding for the connexin26 - basophilic material on the cupulae of the semicircular ducts, an postnatal ageing phenomenon seen in some vestibular labyrinth. (More? ) - taken from last menstrual period (LMP) and therefore approximately two weeks before fertilization occurs. - (outer phalangeal cells) - (DDR1) a tyrosine kinase receptor activated by native collagen, expressed in the basement membrane and with fibrillar collagens. Found in basal cells of the stria vascularis, type III fibrocytes, and cells lining the basilar membrane of the organ of Corti. - inner ear structure, a canal from the utricle that joins the ductus endolymphaticus from the saccule posterior wall, and then passes along the aquaductus vestibuli and ends in a blind pouch (saccus endolymphaticus) in the petrous portion of the temporal bone, also in contact with the dura mater. (More? | | ) - the process of bone formation from a pre-existing cartilage template. (More? ) - One of the initial 3 germ cell layers (ectoderm, mesoderm and endoderm) formed by the process of . The endoderm forms as a cuboidal epithelium and contributes not only to the , but also lines the yolk sac. It will form the entire epithelial lining of the gastrointestinal tract (GIT), contribute to the accessory organs of GIT and also forms the epithelial lining of the respiratory tract. - (endolymph, Scarpa's fluid) fluid that fills all the membranous labyrinth of the inner ear, except for the cochlea scala tympani and scala vestibuli which are filled with perilymph. - inner ear structure that has anatomically both an intraosseous and extraosseous component. Th e sac has functions regulating endolymph that are both secretory and absorptive. Also the site of endolymphatic sac tumors either sporadical occurring or associated with the autosomal-dominant von Hippel-Lindau (VHL) disease, due to a germ line mutation. (More? ) - taken from the time of fertilization which typically occurs around the middle (day 14), or just after, of the typical 28 day menstrual cycle. (More? ) - homeobox gene affecting middle ear and inner ear development. - (auditory tube) A cavity linking the pharynx to the middle ear, which develops from the first pharyngeal pouch. Named after Bartolomeo Eustachi (1500 - 1574) an Italian anatomist. (More? ) - (ear canal) develops from the first pharyngeal cleft. (More? ) - see cerumen. (More? ) - calcium-resistant actin-bundling proteins enriched in hair cell stereocilia and sensory cell microvilli and spiral ganglion neurons (SGNs) - (auditory tube) between the middle ear and oral cavity, equalization of pressure in the middle ear. (More? ) - (EAM, ear canal) cavity connecting the external ear to the tympanic membrane. The adult human ear canal is about 2.5 cm long and 0.7 cm in diameter. (More? ) - (oval window) separates the tympanic cavity from the vestibule of the osseous labyrinth. (More? ) - (round window) separates the tympanic cavity from the scala tympani of the cochlea. (More? ) - (foetus) term used to describe human development after the 8th week (10th clinical week, LPM) and covers the developmental periods of second and third trimester. - ( -1) a growth factor released from cochlea sensory epithelium which stimulates spiral ganglion neurite branching. - ( -8) a growth factor released by inner hair cells which regulates pillar cell number, position and rate of development. - (Fgfr-3) a tyrosine kinase receptor with a role in the commitment, differentiation and position of pillar cells in the organ of corti - (natural frequency) the lowest frequency in a harmonic series, for the female voice this is about 225 Hz. - (petrotympanic fissure, squamotympanic fissure) the fissure in the temporal bone that runs between the temporomandibular joint to the tympanic cavity. Named after Johann Glaser (1629–1675) a Swiss anatomist. - term used to describe the cochlear apex. (More? ) - within the tectorial membrane a ridge that runs longitudinally along the lower surface immediately adjacent to the hair bundles of the inner hair cells. - (hairy and enhancer of split) family of factors, which has been shown to be a general negative regulator of neurogenesis (Zheng, 2000). - a small hill, used to describe the six surface elevations on pharyngeal arch one and two. (More? ) - (anvil) auditory ossicle (More? ) - in the cochlea a single row of cells, that along with and three rows of outer phalangeal cells (Deiter's cells), are the hair cell supporting cells. (More? ) - organ of Corti cells arranged in rows and form a boundary between the single row of inner hair cells and three rows of outer hair cells. These cells have surface-associated microtubule bundles. (More? ) - area of the cochlear duct. (More? ) - (internal acoustic meatus, IAM) Anatomical canal in which CN VII and CN VIII ganglia reside and pass through to the brainstem. This bony canal lies between the posterior surface of the petrous pyramid and the bony labyrinth within the dense petrous bone. Also associated clinically with the site where acoustic neuromas may occur. (More? ) - (Kimura’s membrane) within the tectorial membrane a thickening of the lower surface into which the hair bundles of the outer hair cells are imbedded. - inner ear hair cell specialised type of cilium on the cell apex. - (Kollicker's organ, greater epithelial ridge) Developing cochlear structure consisting of columnar-shaped supporting cells filling the inner sulcus and lying directly under the tectorial membrane. This transient organ regresses and generates the space of the inner sulcus. Rudolph Albert von Kolliker (1817-1905)?? (More? - (external) (More? )
-
- acronym for last menstrual period, used to clinically measure gestation.
- (hammer) auditory ossicle (More? ) - of temporal bone (More? ) - homolog of the Drosophila proneural gene atonal, necessary and sufficient for the production of hair cells in the mouse inner ear. Negatively regulated by Hes1 and Hes5 - temporary blockage of the external auditory meatus which forms at the end of the embryonic period and remains present until the seventh month. - anatomical opening, cavity or space (external acoustic meatus, internal auditory meatus) - (MET) occurs within the cochlear hair cells hair bundle. A mechanical stimulus of the hair bundle causes the tip-links to be tensioned, opening ion channels, resulting in the generation of the cell receptor potential. (More? ) - first pharyngeal ach cartilage, located within the mandibular prominence. This cartilage first appears at stage 16, stage 20 the beginning of membranous ossification. Named after Johann Friedrich Meckel, (1781 - 1833) a German anatomist. ( ) (More? ) - (More? ) - (MPS IIIB, Sanfilippo Syndrome type B) abnormality caused by a deficiency in the lysosomal enzyme N-acetyl-glucosaminidase (Naglu). Children with MPS IIIB develop abnormal hearing, and mental functioning culminating in early death. - secreted growth factor, expressed in the organ of Corti and spiral ganglion cells, role in process outgrowth. (More? ) - (OET) hearing test measures sounds generated by the outer hair cells of the cochlea in response to clicks or tone bursts emitted and recorded by a tiny microphone placed in the infant’s external ear canal. (More? ) - brainstem cholinergic and GABAergic efferent system that innervates sensory cells and sensory neurons of the inner ear. - (spiral organ) cochlea component required for converting vibration into neural signals. (More? ) - (OCP-II) cytosolic protein or transcription factor? (More? ) - extracellular matrix that cover the sensory epithelia of the inner ear. (More? ) - (small bone, auditory ossicles) the individual bone of the three middle ear bones ( , , ), which reduce vibrational amplitude but increase force to drive fluid-filled inner ear. (More? ) - to form bone. (More? | ) - - middle ear infection, peak age prevalence is 6 to 18 months old with many children (75%) have at least one episode by school age. Forms include on-suppurative, suppurative, acute otitis media, chronic otitis media. (More? , ) - the early embryonic transient structure formed by the invagination (folding inward) of the otic placode, to cup, then vesicle stage. This will eventually form structures. - Embryonic ectodermal epithelium giving rise to inner ear structures. (More? | ) - the early embryonic transient structure formed by the invagination (folding inward) and fusion of the otic cup, separating this structure from the embryo surface. This will eventually form structures.(More? ) - inner ear biominerals required for vestibular apparatus function. (More? ) - (Otog) an inner ear specific glycoprotein expressed in cochlea cells at different developmental times. (More? ) - a membrane within the utricle and saccule containing embedded hair cell cilia and small crystalline bodies of calcium carbonate (otoliths). Functions to detect head motion. - small crystalline bodies of calcium carbonate found within the otolitic membrane of the utricle and saccule. (More? ) - compound or drug causing temporary or permanent hearing loss. (More? {{hearing abnormalities) - (OHCs) three rows of hair cells that function to increase basilar membrane motion through a local mechanical feedback process within the cochlea, the " cochlear amplifier". - arranged in rows and form a boundary between the single row of inner hair cells and three rows of outer hair cells. (More? ) - muscles lying beside the auditory (Eustachian) tube. The tensor veli, palatini (TVP) and tensor tympani muscles. (More? ) - the fluid between the membraneous labyrinth of the ear and the bone which encloses it. - the space between the outer wall of the membranous labyrinth and the wall of the bony labyrinth that contains the perilymph. - - in humans, two missense mutations in this gene cause non-syndromic recessive deafness (DFNB59) by affecting the function of auditory neurons. - (Glaserian fissure, squamotympanic fissure) the fissure in the temporal bone that runs between the temporomandibular joint to the tympanic cavity. - (More? ) pharyngeal pouch pharyngeal membrane Pharynx - (PC) form an inner and outer row of support cells that form a boundary between inner and outer hair cells. (More? ) - ear flick in in response to sound. - age-related hearing loss, is the cumulative effect of aging on hearing. - a motor protein structurally similar to the anion transporter family expressed in cochlear outer hair cells. (More? ) - skin tags located in front of the external ear opening, are common in neonates and in most cases are normal, though in some cases are indicative of other associated abnormalities. - (Pcdh15) required for initial formation of stereocilia bundles and changes in the actin meshwork within hair cells. The Ames waltzer (av) mouse mutant has both auditory and vestibular abnormalities from a mutation in this gene. - pharyngeal arch 2 cartilage, named after Karl Bogislaus Reichert (1811 - 1883) a German anatomist. (More? | ) - (vestibular membrane, vestibular wall) is a membrane located inside the cochlea separating the scala media from scala vestibuli. Named after Ernst Reissner (1824-1878) a German anatomist. It primarily functions as a diffusion barrier, allowing nutrients to travel from the perilymph to the endolymph of the membranous labyrinth. - hindbrain rostrocaudal segmentation established by expression of Hox homeodomain transcription factors. Histologically rhombomeres are visible as undulating folds (scalloping) of the neural tube in the hindbrain region and have associated cranial nerves. ) - (Latin, sacculus = a small pouch) sensory cells in the inner ear that translate head movements into neural signals for the brain to interpret. (More? ) - thought to have a role in maintaining the relative position of the head and the body against the vertical linear acceleration of gravity. - one of the three cochlea cavities, it is filled with perilymph. - (vestibular ganglion) primary afferent vestibular neuron ganglion of the vestibular nerve. Located within the internal auditory meatus. (More? ) - series of fluid-filled loops of the inner ear required for balance and sensing acceleration. (More? ) - term used to describe one of the two major classes of hearing loss involving the central pathway from the cochlear (other form is conductive loss). - within the cochlea, an organ of Corti space between the outer pillar cells and the phalangeal and hair cells. Named after Jean-Pierre Nuel (1847-1920) a Belgian ophthalmologist. (More? ) - (SGN) innervate the inner (Type I) and outer (Type II) hair cells of the cochlea. (More? ) - (innervated by CN VII tympanic branch) one of the two muscles in the middle ear, contraction of this muscle pulls the stapes and dampens auditory ossicle movement. (More? ) - (stirrup) a middle ear auditory ossicle (bone) (More? ) - (More? ) - {Moro reflex) -finger-like projections from the apical surface of sensory hair cells forming the hair bundle in the cochlea. Formed by tightly cross-linked parallel actin filaments in a paracrystalline array with cell surface specializations (tip links, horizontal top connectors, and tectorial membrane attachment crowns). - classification of epithelium which transiently forms a plug in external ear canal to the outer eardrum. - forms the outer wall of the cochlear duct of the mammalian cochlea is composed primarily of three types of cells. Marginal cells line the lumen of the cochlear duct and are of epithelial origin. Basal cells also form a continuous layer and they may be mesodermal or derived from the neural crest. Intermediate cells are melanocyte-like cells, presumably derived from the neural crest, and are scattered between the marginal and basal cell layers. The stria forms endolymph and also contains a rich supply of blood vessels. (More? ) - - anatomically normally separate skeletal bones fused together. (More? ) - within the cochlea an extracellular matrix produced by interdental cells, that covers the sensory epithelial hair cells of the organ of corti. (More? ) - (TECTA, TECTB) major non-collagenous protein component of the tectorial membrane forming a striated-sheet matrix. Synthesized as glycosylphosphatidylinositol-linked, membrane bound precursors. - (More? ) - (innervated by CN V mandibular nerve) one of the two muscles in the middle ear, contraction of this muscle pulls the malleus and tenses the tympanic membrane, dampening auditory ossicle movement. The muscle arises from auditory tube (cartilaginous portion) and is inserted into the malleus (manubrium near the root). - - term describing the mapping along the tectorial membrane within the cochlea of the different sound frequencies. (More? ) - (ear drum) - an incomplete circle, in the concavity of which is a groove, the tympanic sulcus, for the attachment of the circumference of the tympanic membrane. In the newborn the ring is still open and expands laterally to form the tympanic part of temporal bone. - (Scarpa's ganglion) primary afferent vestibular neuron ganglion of the vestibular nerve. Located within the internal auditory meatus. (More? ) - (Reissner's) extends from the spiral lamina to the outer wall and divides the cochlea into an upper scala vestibuli, a lower scala tympani. (More? ) - Cranial Nerve VIII - A PDZ scaffold protein expressed in hair cells at the stereocilia tips, essential for the stereocilia elongation process. The DFNB31 gene mutations cause hearing loss in human and mouse. This protein can interact with membrane-associated guanylate kinase (MAGUK) protein, erythrocyte protein p55 (p55). (More? ) - signaling through the Wnt pathway regulates the development of hair cell unidirectional stereociliary bundle orientation. (More? ) | Other Terms Lists | | : | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | External LinksExternal Links Notice - The dynamic nature of the internet may mean that some of these listed links may no longer function. If the link no longer works search the web with the link text or name. Links to any external commercial sites are provided for information purposes only and should never be considered an endorsement. UNSW Embryology is provided as an educational resource with no clinical information or commercial affiliation. | Embryo Images Unit | | | | | | | |  BGDB : Lecture - Gastrointestinal System | Practical - Gastrointestinal System | Lecture - Face and Ear | Practical - Face and Ear | Lecture - Endocrine | Lecture - Sexual Differentiation | Practical - Sexual Differentiation | Tutorial Glossary LinksCite this page: Hill, M.A. (2024, July 1) Embryology BGD Lecture - Face and Ear Development . Retrieved from https://embryology.med.unsw.edu.au/embryology/index.php/BGD_Lecture_-_Face_and_Ear_Development   MARY L. LEWIS, MD Am Fam Physician. 2014;90(5):289-296 This is part I of a two-part article on the newborn examination. Part II, “ Skin, Trunk, Extremities, Neurologic ,” appears in this issue of AFP . Author disclosure: No relevant financial affiliations. A comprehensive newborn examination involves a systematic inspection. A Ballard score uses physical and neurologic characteristics to assess gestational age. Craniosynostosis is caused by premature fusion of the sutures, and 20% of children with this condition have a genetic mutation or syndrome. The red reflex assessment is normal if there is symmetry in both eyes, without opacities, white spots, or dark spots. If the red reflex findings are abnormal or the patient has a family history of pertinent eye disorders, consultation with an ophthalmologist is warranted. Newborns with low-set ears should be evaluated for a genetic condition. Renal ultrasonography should be performed only in patients with isolated ear anomalies, such as preauricular pits or cup ears, if they are accompanied by other malformations or significant family history. If ankyloglossia is detected, a frenotomy may be considered if it impacts breastfeeding. The neck should be examined for full range of motion because uncorrected torticollis can lead to plagiocephaly and ear misalignment. Proper auscultation is crucial for evaluation of the broncho-pulmonary circulation with close observation for signs of respiratory distress, including tachypnea, nasal flaring, grunting, retractions, and cyanosis. Benign murmurs are often present in the first hours of life. Pulse oximetry should be performed in a systematic fashion before discharge. Part I of this two-part article discusses the assessment of general health, head and neck, heart, and lungs. Part II focuses on assessing extremities, and neurologic function. 1 | | | |
|---|
| Screening for hypoglycemia should be performed in newborns who are large or small for gestational age, newborns of mothers with diabetes mellitus, and late preterm infants (34 to 36 6/7 weeks gestational age). | C | | | Regardless of red reflex test results, all newborns with a family history of retinoblastoma, cataracts, glaucoma, or retinal abnormalities should be referred to an ophthalmologist who is experienced in the examination of children. | C | | | Hearing should be evaluated in all newborns before one month of age, but preferably before discharge, using the auditory brainstem response or the otoacoustic emissions test. | C | | | Recent data indicate that ultrasonography should be performed in newborns with isolated ear anomalies, such as preauricular pits or cup ears, only when they are associated with one or more of the following characteristics: other malformations or dysmorphic features, teratogenic exposures, a family history of deafness, or a maternal history of gestational diabetes. | C | , | | Routine screening for congenital heart disease via pulse oximetry is recommended before discharge at 24 hours of life or later. Diagnostic echocardiography should be performed if screening results are positive. | C | |
General AssessmentA detailed newborn examination should begin with general observation for normal and dysmorphic features. A term newborn should have pink skin, rest symmetrically with the arms and legs in flexion, cry vigorously when stimulated, and move all extremities equally. Table 1 shows the normal ranges for newborn vital signs at 40 weeks' gestation. 2 – 4 The new Ballard score ( http://www.ballardscore.com ) was designed to assess a newborn's gestational age through a scoring system that combines physical characteristics with neuromuscular development. 5 A video depicting this examination is available at http://www.ballardscore.com/Pages/videos.aspx . Once the child's gestational age is established, weight, length, and head circumference should be plotted on a nomogram to determine percentiles. Using this information, the newborn can be classified as average, large, or small for gestational age. | | |
|---|
| Heart rate | 120 to 160 beats per minute | | Respiratory rate | 40 to 60 breaths per minute | | Systolic blood pressure | 60 to 90 mm Hg | | Temperature | 97.7°F to 99.5°F (36.5°C to 37.5°C) | | Weight | Females: 3.5 kg (7 lb, 12 oz); range, 2.8 to 4.0 kg (6 lb, 3 oz to 8 lb, 14 oz) | | Males: 3.6 kg (8 lb); range, 2.9 to 4.2 kg (6 lb, 7 oz to 9 lb, 5 oz) | | Length | 20 in (51 cm); range, 19 to 21 in (48 to 53 cm) | | Head circumference | 14 in (35 cm); range, 13 to 15 in (33 to 37 cm) |
A newborn is considered small for gestational age if birth weight is below the 10th percentile. Intrauterine growth restriction occurs when the baby's growth during pregnancy is poor compared with norms. Measurements that are symmetrically decreased suggest that the newborn has a chronic exposure (e.g., maternal smoking or drug use) that impacted growth, or a congenital infection such as a TORCH infection (toxoplasmosis, other agents, rubella, cytomegalovirus, herpes simplex), a metabolic disorder, or a chromosomal abnormality (e.g., Turner syndrome, trisomies). Newborns with these conditions often display dysmorphic features or are simply constitutionally small. If the causative factor occurred later in pregnancy (e.g., uteroplacental insufficiency), the head circumference will be preserved relative to other measurements. 6 A newborn with a birth weight above the 90th percentile is considered large for gestational age. The most common cause is maternal diabetes mellitus, although other causes include a metabolic or genetic syndrome such as Beckwith-Wiedemann syndrome. Because of an increased risk of hypoglycemia, the American Academy of Pediatrics recommends scheduled glucose screening for newborns who are large or small for gestational age, newborns of mothers with diabetes, and late preterm newborns (34 to 36 6/7 weeks gestational age), and provides protocols for their management. 7 At 40 weeks' gestation, the average head circumference is 14 in (35 cm); range, 13 to 15 in (33 to 37 cm, 10th to 90th percentile). 2 Microcephaly (isolated asymmetrically small head, less than the second percentile or two standard deviations below the mean for age and sex) may indicate central nervous system malformation (e.g., holoprosencephaly, neural tube defect), an infection (e.g., toxoplasmosis, cytomegalovirus infection), or a genetic syndrome (e.g., trisomy 13 and 18 syndrome, fetal alcohol syndrome). Macrocephaly (isolated head enlargement, greater than the 98th percentile or greater than two standard deviations above the mean) may be hereditary or the result of a central nervous system disorder (e.g., hydrocephalus, brain tumor), and imaging may be needed. 3 , 4 After evaluating the overall size and shape of the head for asymmetry or gross structural abnormalities, the fontanelles and sutures should be palpated with the newborn in the upright position. Figure 1 illustrates a normal newborn skull and common deformities. The anterior fontanelle is generally 3 to 6 cm in diameter, whereas the posterior fontanelle is no larger than 1 to 1.5 cm in diameter. A large anterior fontanelle may indicate increased intracranial pressure, Down syndrome, hypophosphatemia, trisomy, or congenital hypothyroidism. Fontanelles are often small in newborns with microcephaly. A prematurely fused suture indicates craniosynostosis and occurs in one out of 1,000 newborns. 8 , 9 Craniosynostosis limits growth of the skull in a direction perpendicular to the suture, while growth may continue in other directions. More than 20% of cases are caused by specific single-gene mutations or chromosomal abnormalities and may be associated with conditions such as Crouzon, Apert, and Pfeiffer syndromes. 10 A misshapen head may be caused by prenatal compressions rather than true synostosis. If this is the case, the misshapen head should resolve spontaneously within the first few months of life. 11 The scalp examination may reveal caput succedaneum, cephalohematoma, and other lesions ( Figure 2 ) . A caput succedaneum is scalp edema that is not limited by suture lines, is often pitting, and decreases over time. Most caputs resolve within 48 hours. A cephalohematoma is caused by injury of a blood vessel in the subperiosteal layer of the calvaria. It is limited by suture lines and occurs more commonly in deliveries in which forceps or a vacuum extractor was used. Cephalohematoma is a risk factor for jaundice and sepsis and may worsen over 48 hours, potentially taking up to three to four months to fully reabsorb. Skull fractures are rarely present. If a fracture is depressed or accompanied by neurologic symptoms, computed tomography should be performed to rule out intracranial pathology. 12 Forceps use or a difficult delivery may also lead to a facial nerve palsy resulting in the inability to close the eye, loss of the nasolabial fold, drooping at the corner of mouth, or the inability to contract the ipsilateral lower facial muscles. This usually resolves within the first few weeks of life, but further evaluation is warranted if symptoms persist. 13 The newborn evaluation should include noting eye color; pupil size; appearance of the conjunctiva, sclera, and eyelid; eye movement; and spacing between the eyes. Genetic syndromes often cause unusual eye shape, such as epicanthal folds (excess skin over the medial aspect of the eye) and upslanting of palpebral fissures associated with Down syndrome. Colobomas (a gap or defect in the structure of the eye, primarily the iris) may occur with many syndromes, including CHARGE (coloboma of the eye, heart defects, choanal atresia, retraction of growth and/or development, genital and/or urinary abnormalities, and ear abnormalities and deafness). Infants with colobomas need a formal ophthalmology evaluation. Hypertelorism (increased space between the eyes) and hypotelorism (decreased space between the eyes) are often associated with a genetic disorder. 14 The visual acuity of newborns is approximately 20/400, and a dysconjugate gaze is normal in the first two to three months of life. Subconjunctival hemorrhages from blood vessel rupture are also a common benign finding that may take weeks to resolve. The red reflex test is performed by using an ophthalmoscope, with the lens power set at 0 and the examiner standing approximately 18 inches away. Light should project onto both eyes simultaneously. A red reflex result is normal if there is symmetry in both eyes without opacities, white spots, or dark spots ( Figure 3 15 ) . The color of the reflex may be different among ethnic groups because of varying amounts of pigmentation in the ocular fundus; however, the reflex should not be white. 14 , 16 Table 2 gives a differential diagnosis of leukokoria. 14 , 16 An abnormal red reflex result warrants urgent referral to an ophthalmologist. Regardless of red reflex findings, all newborns with a family history of retinoblastoma, cataracts, glaucoma, or retinal abnormalities should be referred to an ophthalmologist experienced in the examination of children because of the high risk of serious eye abnormalities. 17  | | |
|---|
| Cataract | Opacity or clouding of the lens, often due to a genetic or systemic disorder | | Chorioretinitis | Inflammation of the retina and choroid, may be due to cytomegalovirus or toxoplasmosis | | Coats disease | Congenital disorder caused by abnormal blood vessels behind the retina, leads to progressive deterioration of vision | | Coloboma | Full-thickness defect of the eye | | Persistent fetal vasculature | Failure of the hyaloid vascular system and the embryonic vitreous to completely involute | | Retinoblastoma | Most common intraocular tumor in children | | Retinopathy of prematurity | Abnormal blood vessel development, occurs primarily in premature infants | | Vitreous hemorrhage | Blood clot in the vitreous body, often due to trauma or hemorrhagic disease |
Dacryostenosis should be differentiated from ophthalmia neonatorum, which is conjunctivitis within the first four weeks of life ( Table 3 ) . 18 With dacryostenosis, a blocked tear duct causes secretions to accumulate with a yellow sticky appearance while the rest of the eye appears normal. 19 With conjunctivitis, however, there is often edema and conjunctival injection. 18 | | |
|---|
| Chemical irritant | First 24 to 36 hours, conjunctival injection and erythema | | Gonococcal infection | Days 2 to 7, bilateral purulent conjunctivitis | | Chlamydia infection | Days 5 to 14, varies from mild hyperemia to diffuse swelling and chemosis | | Herpes simplex virus infection | Days 6 to 14, keratoconjunctivitis is often present |
Hearing should be evaluated in all newborns before one month of age, but preferably before discharge, using the auditory brainstem response or the otoacoustic emissions test. 20 Assessing the size, shape, and position of the ears may reveal congenital abnormalities. Ears are considered low-set when the helix of the ear meets the cranium at a level below that of a horizontal plane through both inner canthi ( Figure 4 ) . Low-set ears are often a sign of a genetic condition (e.g., Down, Turner, or trisomy 18 syndrome). Microtia (small and underdeveloped pinnae) is commonly associated with another defect, such as CHARGE syndrome. 21 Because preauricular skin tags and ear pits are associated with permanent hearing impairment in newborns, screening and close monitoring are warranted. 22 There is a known association between ear and renal abnormalities, and a variety of syndromes demonstrate both ear and renal defects. 23 – 25 In the past, there was uncertainty about which ear malformations warranted screening renal ultrasonography. Recent data indicate that ultrasonography should be performed in patients with isolated ear anomalies, such as preauricular pits or cup ears, only when they are associated with one or more of the following characteristics: other malformations or dysmorphic features, teratogenic exposures, a family history of deafness, or a maternal history of gestational diabetes. 26 – 28 Ear canals should be observed for patency. Choanal atresia occurs when one or both sides of the nasal airway are narrowed or blocked. To assess patency of the nostrils, a small-caliber catheter can be passed through the nasal passages. If bilateral choanal atresia is present, the infant may have cyanosis that is relieved by crying. Asymmetry of the nasal septum is often due to in utero positioning. If it can be corrected by depression of the tip of the nose, it will usually resolve on its own. However, asymmetry that does not correct with depression of the nose tip indicates a dislocated septum, and the patient should be evaluated by an otolaryngologist. 29 , 30 The maxilla and mandible should fit together well and open at equal angles. Micrognathia (a small mandible) occurs with Pierre Robin syndrome. Table 4 details common oral cavity findings. 31 Ankyloglossia occurs when a short frenulum attaches the tongue to the floor of the mouth, limiting its mobility. This may interfere with breastfeeding or impair articulation, although frenotomy is controversial. 32 – 34 Palpating the palate can reveal submucosal and mucosal clefts. A bifid uvula is often associated with a submucosal cleft. Cleft lip and palate are the most common anomalies of the head and neck. Midline clefts warrant investigation for a midline defect in the brain or other abnormalities. 35 | | |
|---|
| Bohn nodules | Remnants of salivary gland tissue on the lateral aspect of the gum, resolve spontaneously | | Epstein pearls | White cystic vesicles (1 to 3 mm) on the median palatal raphe of the mouth, oral counterpart to milia, resolve spontaneously | | Natal teeth | Often occur on the lower gum, should be removed if loose because of aspiration risk | | Ranula | Mucus retention cysts on the floor of mouth, often require surgical removal |
The neck should be inspected for full range of motion because congenital torticollis is a common musculoskeletal anomaly of newborns. Torticollis is primarily due to birth trauma to the sternocleidomastoid muscle that causes swelling or sometimes hematoma formation within the muscle. It can usually be corrected with physical therapy. 36 If not corrected, torticollis can lead to plagiocephaly and ear misalignment. Other possible findings on the neck examination include webbing, which can occur with Turner syndrome, and branchial clefts, pits, and masses. A cystic hygroma is a congenital lymphatic malformation in the neck region. A midline neck lesion may represent a thyroglossal duct cyst and typically shifts with movement of the tongue. The clavicles should be palpated for fracture, which may manifest only as asymmetric Moro reflex if nondisplaced. A suspected fracture should be confirmed with a radiograph. Fractures can be a result of birth trauma and are typically treated with analgesics for pain. 37 When a newborn takes the first breath, subsequent decreases in resistance in the pulmonary vasculature and increases in oxygen concentration result in eventual closure of the shunts, which allow the newborn to transition to adult circulation. Congenital heart disease occurs in approximately six out of 1,000 live births. 38 Newborns with heart disease often exhibit tachypnea without retractions. Cyanosis is often present with severe disease. 38 This appearance should be differentiated from acrocyanosis (isolated cyanosis of the hands and feet), which is normal in newborns. Upon auscultation of the heart in the standard four locations (right upper sternal border, left upper sternal border, left lower sternal border, and between the fifth and sixth intercostal space in the midclavicular line), the first heart sound should be single and the second heart sound split. Table 5 summarizes important cardiac examination findings. 38 , 39 Because of changes in vasculature immediately after birth, benign murmurs are common in the first hours of life. 38 , 39 Routine screening for congenital heart disease via pulse oximetry is recommended before discharge at 24 hours of life or later, or shortly before discharge if earlier than 24 hours. Diagnostic echocardiography should be performed if screening results are positive ( Table 6 ) . 40 , 41 | | |
|---|
| Weak pulses | Poor cardiac output (e.g., aortic stenosis) | | Bounding pulses | High cardiac output (e.g., patent ductus arteriosus) | | Single second heart sound | Often cyanotic heart disease (e.g., truncus arteriosus, hypoplastic left heart) | | Holosystolic, continuous, harsh murmur | Pathologic | | Grade 3 or higher murmur | Pathologic | | Diastolic murmur | Pathologic | | Hepatomegaly | Left heart failure |
| | | | |
|---|
| 24 hours of life or later (or shortly before discharge, if earlier) | ≥ 95% in right hand or foot, with 3% or less absolute difference in oxygen saturation between the right hand and foot | Negative screening result | Plan for discharge | | 24 hours of life or later (or shortly before discharge, if earlier) | 90% to 94% in right hand or foot, or 3% or less absolute difference in oxygen saturation between the right hand and foot | Repeat screening needed in one hour | If repeat results are in this range, repeat screening again in one hour; three readings in this range warrant echocardiography | | 24 hours of life or later (or shortly before discharge, if earlier) or on repeat screening | < 90% in right hand or foot | Positive screening result | Echocardiography |
The respiratory examination is important because the infant is transitioning from fetal to neonatal life. The alveoli are filling with air, the systemic vascular resistance is increasing, and the pulmonary vascular resistance is decreasing. The examiner should observe for signs of respiratory distress, including tachypnea, nasal flaring, grunting, retractions, and cyanosis. Breath sounds should be equal on auscultation. Unequal breath sounds may indicate a pneumothorax and should prompt imaging. Transient tachypnea of the newborn occurs predominantly in those born via cesarean delivery or precipitous delivery. It is caused by retained fluid in the lungs, which can result in alveolar hypoventilation. 42 Treatment includes supportive respiratory care because the condition resolves within 48 hours. Respiratory distress syndrome arises from lack of surfactant, which leads to alveolar collapse. Although it is most common in preterm infants, it may occur in term infants, particularly if the mother has diabetes. A previous article in American Family Physician includes a detailed review of respiratory distress in the newborn. 43 Data Sources : A PubMed search was completed using the terms infant, newborn, developmental delay, developmental disturbance, and physical examination. The search included meta-analyses, randomized controlled trials, clinical trials, and reviews. We also searched POEMs (patient-oriented evidence that matters), Clinical Evidence, the Cochrane database, and Essential Evidence Plus. Search dates: January 1, 2012, and May 2, 2014. The opinions and assertions contained herein are the private views of the author and are not to be construed as official or as reflecting the views of the U.S. Army Medical Department or the U.S. Army Service at large. Lewis ML. A comprehensive newborn examination: part II. Skin, trunk, extremities, neurologic. Am Fam Physician. 2014;90(5):297-302. Lissauer T. Physical examination of the newborn. In: Martin RJ, Fanaroff AA, Walsh MC, eds. Fanaroff and Martin's Neonatal-Perinatal Medicine: Diseases of the Fetus and Infant . 9th ed. Philadelphia, Pa.: Saunders/Elsevier; 2011:485. Sniderman A. Abnormal head growth. Pediatr Rev. 2010;31(9):382-384. Tschudy MM, Arcara KM; Johns Hopkins Hospital. The Harriet Lane Handbook . 19th ed. Philadelphia, Pa.: Mosby Elsevier; 2012. Ballard JL, Khoury JC, Wedig K, Wang L, Eilers-Walsman BL, Lipp R. New Ballard score, expanded to include extremely premature infants. J Pediatr. 1991;119(3):417-423. Intrauterine growth restriction. Washington, DC: American College of Obstetricians and Gynecologists; May 2013. ACOG Practice Bulletin No. 134. Adamkin DH Committee on Fetus and Newborn. Postnatal glucose homeostasis in late-preterm and term infants. Pediatrics. 2011;127(3):575-579. Marchac D, Renier D. Treatment of craniosynostosis in infancy. Clin Plast Surg. 1987;14(1):61-72. Nagaraja S, Anslow P, Winter B. Craniosynostosis. Clinic Rad. 2013;68(3):284-292. Johnson D, Wilkie AO. Craniosynostosis. Eur J Hum Genet. 2011;19(4):369-376. Kabbani H, Raghuveer TS. Craniosynostosis. Am Fam Physician. 2004;69(12):2863-2870. Uhing MR. Management of birth injuries. Pediatr Clin North Am. 2004;51(4):1169-1186. Falco NA, Eriksson E. Facial nerve palsy in the newborn: incidence and outcome. Plast Reconstr Surg. 1990;85(1):1-4. Guercio JR, Martyn LJ. Congenital malformations of the eye and orbit. Otolaryngol Clin North Am. 2007;40(1):113-140. Bell AL, Rodes ME, Collier Kellar L. Childhood eye examination [published correction appears in Am Fam Physician . 2014;89(2):76]. Am Fam Physician. 2013;88(4):241-248. Cheng KP, Hiles DA, Biglan AW. The differential diagnosis of leukokoria. Pediatr Ann. 1990;19(6):376-383. American Academy of Pediatrics; Section on Ophthalmology; American Association for Pediatric Ophthalmology and Strabismus; American Academy of Ophthalmology; American Association of Certified Orthoptists. Red reflex examination in neonates, infants, and children [published correction appears in Pediatrics . 2009;123(4):1254]. Pediatrics. 2008;122(6):1401-1404. Prevention of neonatal ophthalmia. In: Pickering LK, ed. Red Book: 2009 Report of the Committee on Infectious Diseases . 29th ed. Elk Grove Village, Ill.: American Academy of Pediatrics; 2012:880–882. Robb RM. Congenital nasolacrimal duct obstruction. Ophthalmol Clin North Am. 2001;14(3):443-446. American Academy of Pediatrics, Joint Committee on Infant Hearing. Year 2007 position statement: principles and guidelines for early hearing detection and intervention programs. Pediatrics. 2007;120(4):898-921. Harris J, Källén B, Robert E. The epidemiology of anotia and microtia. J Med Genet. 1996;33(10):809-813. Roth DA, Hildesheimer M, Bardenstein S, et al. Preauricular skin tags and ear pits are associated with permanent hearing impairment in newborns. Pediatrics. 2008;122(4):e884-e890. Leung AK, Robson WL. Association of preauricular sinuses and renal anomalies. Urology. 1992;40(3):259-261. Hilson D. Malformations of ear as a sign of malformations of genitourinary tract. Br Med J. 1957;2(5048):785-789. Wang RY, Earl DL, Ruder RO, Graham JM. Syndromic ear anomolies and renal ultrasounds. Pediatrics. 2001;108(2):e32. Kugelman A, Tubi A, Bader D, Chemo M, Dabbah H. Pre-auricular tags and pits in the newborn: the role of renal ultrasonography. J Pediatr. 2002;141(3):388-391. Wang RY, Earl DL, Ruder RO, Graham JM. Syndromic ear anomalies and renal ultrasounds. Pediatrics. 2001;108(2):E32. Deshpande SA, Watson H. Renal ultrasonography not required in babies with isolated minor ear anomalies. Arch Dis Child Fetal Neonatal Ed. 2006;91(1):F29-F30. Myer CM, Cotton RT. Nasal obstruction in the pediatric patient. Pediatrics. 1983;72(6):766-777. Hengerer AS, Brickman TM, Jeyakumar A. Choanal atresia: embryologic analysis and evolution of treatment, a 30-year experience. Laryngoscope. 2008;118(5):862-866. Mueller DT, Callanan VP. Congenital malformations of the oral cavity. Otolaryngol Clin North Am. 2007;40(1):141-160. Forlenza GP, Paradise Black NM, McNamara EG, Sullivan SE. Ankyloglossia, exclusive breastfeeding, and failure to thrive. Pediatrics. 2010;125(6):e1500-e1504. Messner AH, Lalakea ML. Ankyloglossia: controversies in management. Int J Pediatr Otorhinolaryngol. 2000;54(2–3):123-131. Ballard JL, Auer CE, Khoury JC. Ankyloglossia: assessment, incidence, and effect of frenuloplasty on the breastfeeding dyad. Pediatrics. 2002;110(5):e63. Fisher DM, Sommerlad BC. Cleft lip, cleft palate, and velopharyngeal insufficiency. Plast Reconstr Surg. 2011;128(4):342e-360e. Cheng JC, Wong MW, Tang SP, Chen TM, Shum SL, Wong EM. Clinical determinants of the outcome of manual stretching in the treatment of congenital muscular torticollis in infants. A prospective study of eight hundred and twenty-one cases. J Bone Joint Surg Am. 2001;83-A(5):679-687. Hsu TY, Hung FC, Lu YJ, et al. Neonatal clavicular fracture: clinical analysis of incidence, predisposing factors, diagnosis, and outcome. Am J Perinatol. 2002;19(1):17-21. Wren C, Reinhardt Z, Khawaja K. Twenty-year trends in diagnosis of life-threatening neonatal cardiovascular malformations. Arch Dis Child Fetal Neonatal Ed. 2008;93(1):F33-F35. Dolbec K, Mick NW. Congenital heart disease. Emerg Med Clin North Am. 2011;29(4):811-827. Mahle WT, Martin GR, Beekman RH, Morrow WR Section on Cardiology and Cardiac Surgery Executive Committee. Endorsement of Health and Human Services recommendation for pulse oximetry screening for critical congenital heart disease. Pediatrics. 2012;129(1):190-192. Centers for Disease Control and Prevention. Screening for critical congenital heart defects. http://www.cdc.gov/ncbddd/pediatricgenetics/pulse.html . Accessed April 22, 2014. Machado LU, Fiori HH, Baldisserotto M, Ramos Garcia PC, Vieira AC, Fiori RM. Surfactant deficiency in transient tachypnea of the newborn. J Pediatr. 2011;159(5):750-754. Hermansen CL, Lorah KN. Respiratory distress in the newborn. Am Fam Physician. 2007;76(7):987-994. Continue Reading More in AFPCopyright © 2014 by the American Academy of Family Physicians. This content is owned by the AAFP. A person viewing it online may make one printout of the material and may use that printout only for his or her personal, non-commercial reference. This material may not otherwise be downloaded, copied, printed, stored, transmitted or reproduced in any medium, whether now known or later invented, except as authorized in writing by the AAFP. See permissions for copyright questions and/or permission requests. Copyright © 2024 American Academy of Family Physicians. All Rights Reserved. You are using an outdated browser. Please upgrade your browser or activate Google Chrome Frame to improve your experience.  Normal ear and its evaluationThe mammalian ear can be divided into three main parts: the outer ear, middle ear, and inner ear, all of which are required for effective hearing. Author: Ian Suchet 1 , Janelle Santos 2 1. Ian Suchet MBBCh FRCPC, Calgary MFM Centre, EFW Radiology, Calgary, Alberta Canada 2. Mayo Clinic, Department of Obstetrics and Gynecology, Rochester, MN, USA Reviewers: Karen Fung-Kee-Fung, Mauro Schenone Imaging of the fetal earImaging modalities that evaluate the fetal ear include: - 2D ultrasound.
- 3D ultrasound.
- MRI of the fetal face and temporal bone.
Ear anomalies, although frequently encountered in many syndromes, has received little attention in the ultrasound literature due to several factors that include: - Visualization of the fetal ear is not part of the routine assessment of the fetus, and therefore isolated ear anomalies are generally missed. Ears are more frequently evaluated when other anomalies present.
- Evaluation of ear location and morphology usually requires 3D imaging as they are more difficult to evaluate on 2D imaging.
- Fetal position and more advanced gestational age make it difficult to image both ears.
- Asymmetry of ear anomalies are common, therefore, each ear must be evaluated separately.
- Very few syndromes have a pathognomonic ear shape. Due to this lack of specificity, evaluation of the ear alone, does not alone make the diagnosis of a syndrome, rather it helps to confirm a syndrome when other more classical sonographic signs are present.
The advantages of assessing the fetal ear include: - Unambiguous findings of an abnormality as the anatomy of the human ear is constant and not ethnically dependent.
- Assessment of ear size, shape, morphology, and location on the fetal face can be obtained.
- Confirmation of a syndrome based on the presence of an abnormal ear.
A retrospective study in Sweden revealed that no ear abnormalities were detected on routine ultrasound, although the prevalence of minor ear abnormalities was 2.4 per 1000 and major ear malformations of 0.3 per 1000 (1). Shih and colleagues obtained adequate images of the fetal ears in 84% of cases when utilizing 3D ultrasound (2). Chang and coworkers (3) determined that 3D ultrasound was superior to 2D ultrasound given that 3D ultrasound allowed for the evaluation of ear shape in 93% of cases versus only 40% with 2D ultrasound (3). First trimester ultrasoundThe ear has been extensively evaluated in the first trimester. Ear size can be measured (Figure 3), however, morphology of the auricle cannot be evaluated at this early GA. Ear location cannot be evaluated due to progressive superior migration and rotation of the auricle with advancing gestational age. Sacchini and coworkers (4) measured fetal ear length at 11-14 weeks of gestation while screening for chromosomal defects. The fetal ear length was measured in 450 fetuses immediately before chorionic villus sampling for karyotyping at 11-14 weeks of gestation. The fetal ear was successfully examined in all cases. The fetal karyotype was normal in 409 cases and abnormal in 41, including 32 cases of trisomy 21. In the chromosomally normal group, the fetal ear length increased with crown-rump length from a mean of 3.7 mm at 45 mm to 6.9 mm at 84 mm (Table 1). Table 1 . Reference range (mean, 5 th and 95 th centiles) of ear length against crown–rump length in chromosomally normal fetuses at 11–14 weeks of gestation (4). 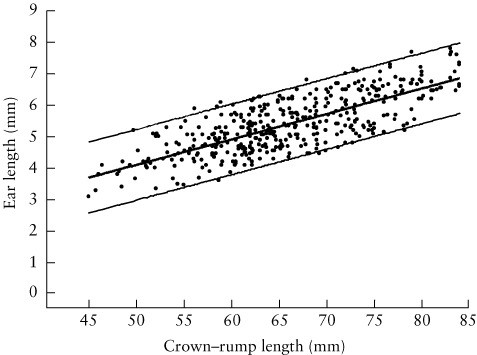 Figure 3: First trimester evaluation of the normal fetal ear. a. Coronal plane (13+6 6 wks GA). Ear length can be measured in this view. b. Sagittal plane in a normal fetus (13+6 wks GA). Ear length can be measured however location and morphology cannot be evaluated. c. 9+3 wks – 3D surface rendered view demonstrates the low location of ear (closed arrow) due to current GA. d. 3D surface rendered view demonstrates normal ear size at 12 wks GA 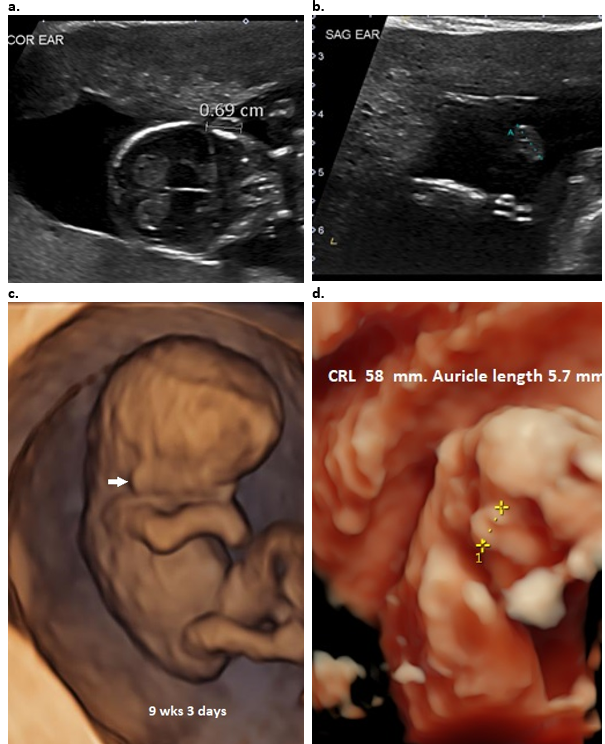 Second and Third trimester ultrasoundA. 2D Ultrasound: The ears are more difficult to evaluate on 2D ultrasound and therefore not routinely imaged. The ears can be evaluated in all three planes which confer different information. Axial / transverse plane – The outer ear should be visible in the same transverse plane as the orbits. Each ear is usually evaluated separately as we have found it extremely difficult to obtain both ears and orbits on the same transverse image (Figure 4 a). Care must be taken to avoid angling the scanning plane inferiorly as low set ears will be demonstrated in the same plane as the orbits and falsely suggest that they are normally located. The major axis of the ear is vertical and parallel to the head (Figure 4b). This view can also be used for evaluating ear protrusion but cannot be used to evaluate anatomy of the auricle. The ear length cannot be measured in this plane, however ear width (Figure 4c) can be measured. Coronal plane – Anatomy of the pinna cannot be evaluated in the coronal plane, however, measurement of ear length and location on the face can be evaluated in this plane (Figure 4d). Sagittal plane – Outer ear morphology is best visualized in the sagittal plane (Figure 5a). The helix and lobe are always well visualized. The tragus and EAC are more difficult to visualize. The full length of the antihelix can be visualized by subtle probe manipulation into an oblique sagittal view (Figure 5b). The location of the ear on the face cannot be evaluated, however ear width and length can be measured in this plane. Figure 4: 2D images through the auricle. - A true transverse / axial image without rotation. Both orbits are imaged (closed arrow). Both ears (open arrows) are difficult to delineate without rotation of the head, however they are located at the level of the orbits.
- Transverse plane with rotation of the head for ear location. Only left ear (open arrows) can be visualized and is at the same level as the orbits (closed arrows). The right orbit is visualized, however the contralateral right ear is not visualized.
- Transverse plane. The width of the ear can be measured from anterior to posterior.
- Coronal image through the auricle – the ear length can be measured from superior helix to inferior portion of the lobe.
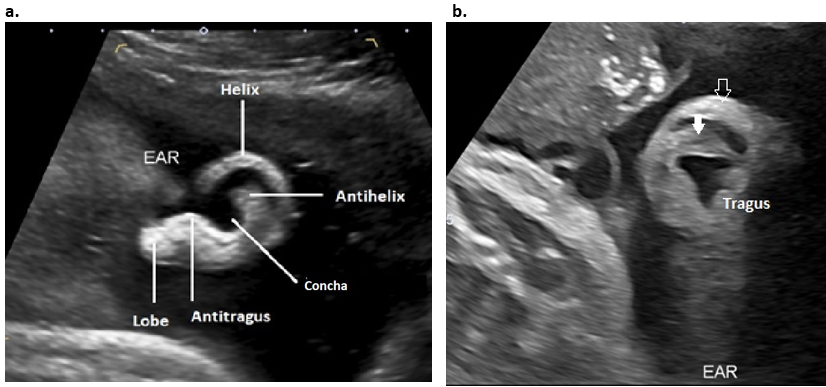
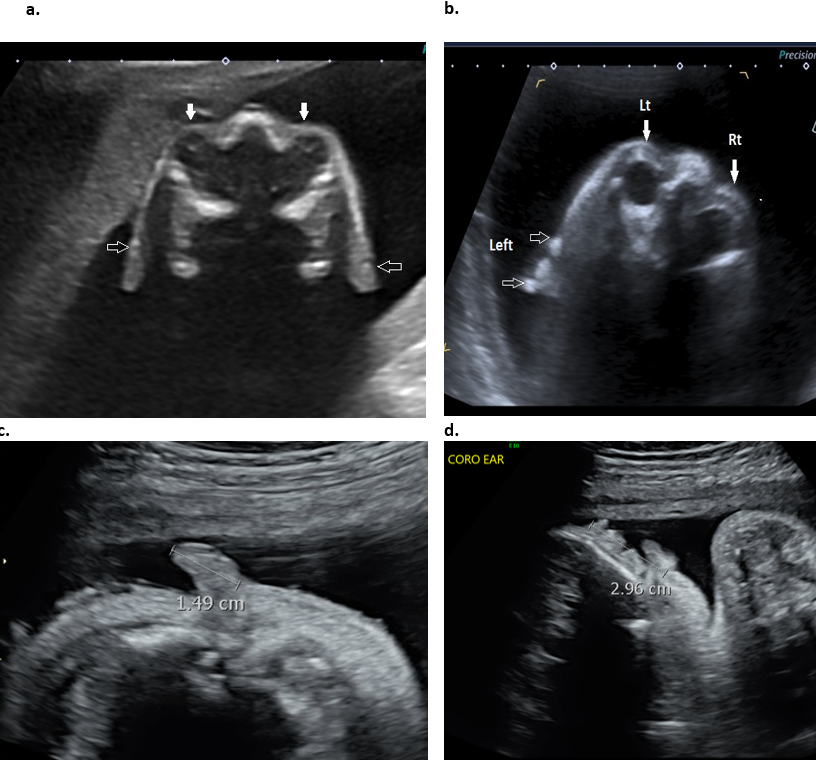 Figure 5: 2D Sagittal plane through the auricle. - Surface anatomy of the ear. The entire helix, the lobe, the stem of the antihelix and antitragus are visualized in this plane, however the superior and inferior branches of the antihelix and tragus are not visualized.
- Rotation of the image into an oblique plane is necessary to visualize the full length of the antihelix (closed arrow) and tragus. The open arrow represents the superior helix.
 B. 3D ultrasound: 3D ultrasound has been shown to be useful in the differentiation between normal and abnormal fetal anatomy (1,2). There are several publications that have evaluated the fetal ear using 3D ultrasound (1-6). Results show that 3D ultrasound reduces the limitations of 2D ultrasound (3) and offers an excellent screening mode for ear malformations and associated disease. 3D ultrasound offers far better visualization and more accurate evaluation of the size, location and anatomy of the auricle. The ears are best examined at 18-25 wks of gestation when they are easy to identify as they are surrounded by more abundant amniotic fluid. Amniotic fluid must be present surrounding the ear in order to obtain and adequate 3D surface rendered images. After the ear is identified on 2D imaging, the 3D volume is acquired in either a coronal or transverse plane (Figure 6). The reconstructed volume is rotated until the ear is visualized in a sagittal plane. The sagittal plane enables visualization of the profile of the face and by widening the render box, the entire face and auricle is visible on the same image. Rotation of the ear along its x- and y-axes enables one to better demonstrate facial and ear anatomy and the degree of protrusion of the ear in the coronal and transverse planes. Most of the major improvements in ultrasound in the last few years have come from the use of high-frequency transducers and the advent HD live technology . There are different 3D surface display modes that are available for assessing outer ear morphology (Figure 7 a-d). All are considered satisfactory, however some demonstrate improved visualization of surface anatomy. The HD live surface mode (GE Medical Systems) shows consistent superiority over the other surface display modes. This improvement is acquired by applying an artificial light source to the rendered image that exposes more anatomical detail. This light source is flexible allowing the user to manipulate the light and highlight the anatomical structure of interest. This 3D rendering method takes advantage of “shadowing effects” to improve the visualization of details on the image. This technique uses a virtual light source and reflects the light off the skin surface rather than a fixed light source in conventional 3D surface rendering, HD live rendering calculates the propagation of light through the skin and the tissue creating shadows where light has moved through denser tissues. The virtual light source can be changed and directed easily from any angle and can be manipulated to enhance visualization of tissue structures, define precise outlines and highlight important clinical details (Figure 7 e-h). This tool is especially valuable when evaluating surfaces, especially the facial area. By changing the angle of virtual light, one can adjust it perfectly to emphasize and get depth perception in visualizing a region of interest that may be an anomaly. A translucent effect is gained if the light source is placed behind the object (5). The effect results in more “lifelike” images. Other workers have shown superiority using a similar display mode called “TrueVue” (Philips Medical Systems). Other 3D modalities that can be used to evaluate the outer ear include multiplanar reformat images (MPR) and volume contrast imaging (VCI). Figure 6. MPR and surface rendered 3D image of the fetal right ear. The original acquisition plane was coronal resulting in the 3D plane being demonstrated in a sagittal plane. The solid arrow represents the location of the render dot that demonstrates a periarticular tag in all planes. The open arrows represent the green render line. 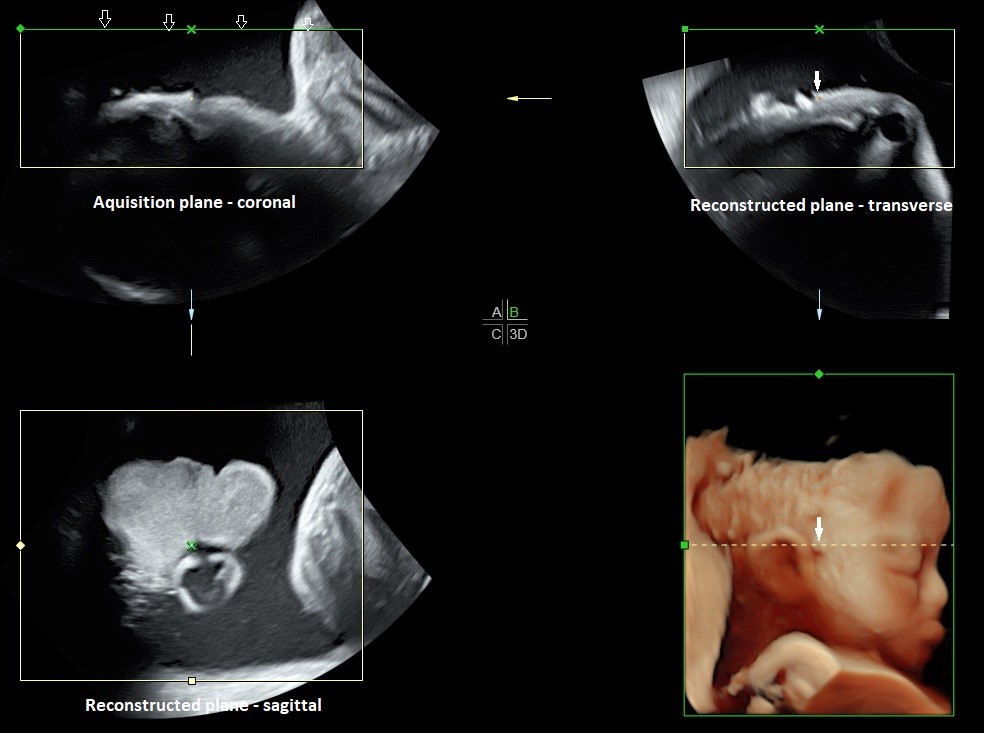 Figure 7. Different surface rendered modes for evaluating the auricle. - Surface mode - The surface is displayed in “texture” mode. The gray values of the surface are identical with the gray values of the original scan.
- Surface smooth mode - The surface is displayed “smoothed” in “texture” mode.
- Surface enhanced mode - This requires HD rendering. The surface display is improved by homogenous smoothing while details are retained in the image.
- HD live surface mode - HD Live allows one to generate realistic life like images of the ear using an advanced illumination model. HD Live supports shadows, using a virtual light source and advanced skin rendering techniques. By highlighting structures from the side the 3D impression is improved and the surface does not appear flat anymore.
e-h. HD live evaluation of the auricle with different positioning of the virtual light (white arrow delineates position of the virtual light). By moving the light source, different areas of the ear are highlighted. 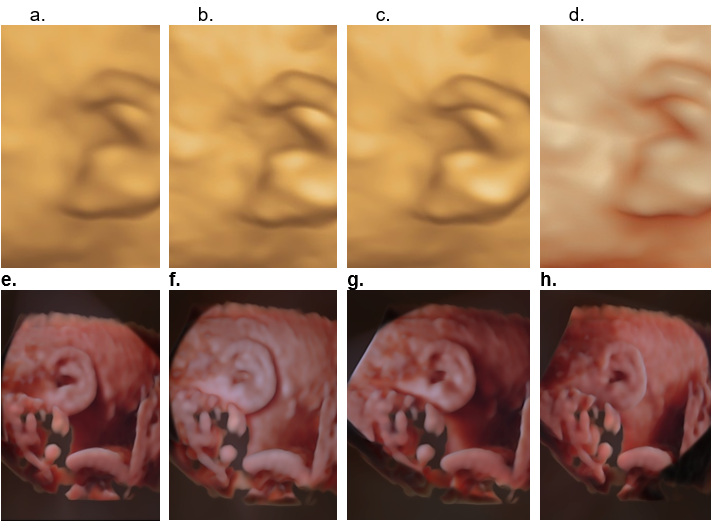 Advantages of 3D over 2D (2) - 3D offers clearer visualization of anatomy especially the helix, the tragus and antitragus.
- Spatial information (location, axis orientation) can only be obtained with 3D
- Clearer observation of ear anomalies increases the threshold of suspicion of other organ anomalies which may have gone unnoticed.
- Unfavourable location of fetal position may make visualization with 2D impossible and can only be visualized by 3D.
Both the left and right auricles must both be evaluated separately as unilateral or asymmetrical abnormalities may be present (e.g. unilateral Microtia, OAV spectrum / Goldenhar syndrome). The auricle is best visualized in the sagittal plane. The anatomy that can be evaluated on sagittal images include: - Size of the auricle
- Shape / morphology of the auricle
- Level of insertion of the auricle
- Evaluation of the angle of the auricle for assessment of auricular protrusion requires the volume to be rotated into a coronal plane (Figure 8). The 3D volume is rotated 90 degrees to the sagittal plane to assess the ear in a PA (posterior-anterior) plane.
Figure 8: 3D surface rendered view of the normally orientated fetal auricle in an AP plane. Note the normal close approximation of the helix (H) and lobe (L) of the auricle to the mastoid region (M) of the skull with no measurable auriculocephalic angle. This close arrangement obscures the actual site of attachment of the ear to the skull.  External auditory canal and meatus (EAC and EAM)The EAC is only visualized after 28 wks once involution of ectodermal plug has occurred. It is fluid filled (amniotic fluid) and reportedly seen in only 59% of normal fetuses (Figure 2 d,e). By the 16th week of embryological development, the contour of the external ear is basically formed. By the 26th week, the external auditory canal can reach one-third of its full length. The EAC rises upward and laterally nearly parallel to the tympanic ring. It reaches its auricular opening, the EAM at the lower border of the squamous temporal bone. Middle ear and inner earThe tympanic rings are round oval echogenic structures in a plane tangential to the inferolateral surface of the fetal skull below the inferior border of the squamous portion of the temporal bone (8). The tympanic ring is an incomplete bony ring due to the tympanic notch that is present in the lateral margin. Visualization of the tympanic rings can be achieved with both 2D and 3D sonography (using multiplanar reconstruction; Figure 9 d). Leibovitz and coworkers (8) elegantly describe the embryology, anatomy and sonographic technique for their demonstration. Ossification of the rings are complete by 19 weeks of gestation when they reach an internal diameter of 7.5 mm (9). Visualization was best in the early second trimester (16 wks) as echogenic structures superimposed on a hypoechoic cartilaginous petrous ring background. Inner ear (7). 2D and 3D US can readily evaluate the auricle, however, sonographic evaluation of the temporal bone is more challenging. Identification of the fetal cochlea caudal to the temporal lobes via US can be obtained in approximately 50% of cases in the second trimester using the fetal anterior fontanelle and coronal plane insonation. The semicircular canals (Figure 9 a-c) may be identified by second-trimester ultrasound, although with limited resolution. Figure 9. The middle and inner ear. a-c Inner ear. a. Schematic illustration of the inner ear. b. Coronal plane MPR image of the superior, posterior, and lateral semicircular canals. c. MPR of the semicircular canals in a coronal and parasagittal plane. d. Middle ear. The tympanic ring and auricles at 18 weeks of gestation obtained from a single volume acquisition after rotating the volume. The 3D rendered image is displayed in a maximal mode. TR – tympanic ring; TB – squamous portion of the temporal bone; PB – parietal bone; FB – frontal bone. 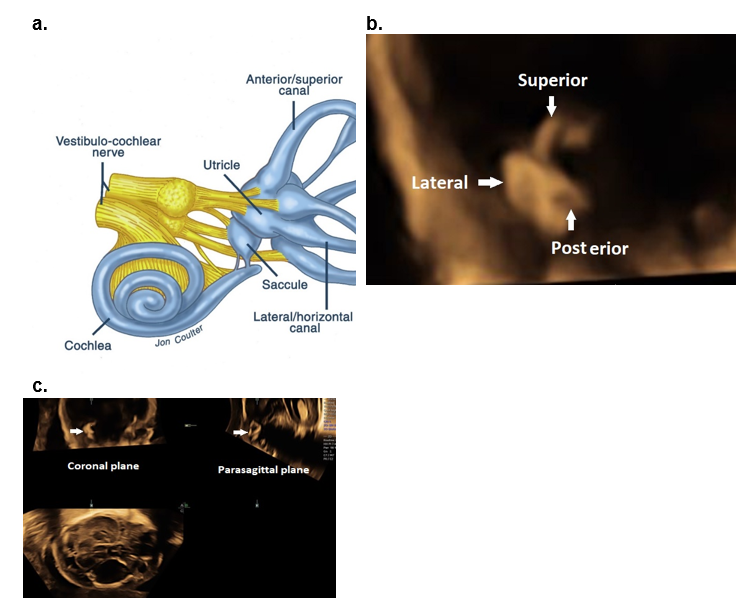 - Romosan G, Henriksson E, Rylander A et.al. Diagnostic performance of routine ultrasound screening for fetal abnormalities in an unselected Swedish population in 2000-2005. Ultrasound Obstet Gynecol 2009;34:526-533.
- Shih JC, Shyu MK, Lee CN et.al. Antenatal depiction of the fetal ear with three-dimensional ultrasonography. Obstet Gynecol,1998; 91(4):500-5
- Chang CH, Chang F M, Yu CH et.al. Fetal ear assessment and prenatal detection of aneuploidy by the quantitative three-dimensional ultrasonography. Ultrasound in Medicine and Biology, 2000; 26(5):743–749.
- Sacchini C, El-Sheikhah A, Cicero S et.al. Ear length in trisomy 21 fetuses at 11-14 weeks of gestation. UOG 2003;22:460-463
- Benoit B, Levaillant JM. Voluson GE healthcare technology. Available at: www.volusonclub.net. 10 Dec 2016.
- Merz E, Welter C. 2D and 3D Ultrasound in the evaluation of normal and abnormal fetal anatomy in the second and third trimesters in a level III center. Ultraschall Med. 2005;26(1): 9–16.
- Daudruy et.al. OP06.04: US anatomy of the middle and inner ear with high‐frequency probe: a pictorial essay. Ultrasound Obstet Gynecol 2017.
- Leibovitz Z, Egenburg S, Brohnshtein M et.al Sonographic imaging of the fetal tympanic rings. Ultrasound Obstet Gynecol 2013;42:536-544.
- Anson BJ, Hanson JS, Richany SF. Early embryology of the auditory ossicles and associated structures in relation to certain anomalies observed clinically. Ann Oto Rhinol Laryngol 1960;69:427-447.
This article should be cited as Suchet I, Santos J: Normal ear and its evaluation . Visual Encyclopedia of Ultrasound in Obstetrics and Gynecology, www.isuog.org , June 2023. Leave feedback or submit an imageWe rely on your feedback to update and improve VISUOG. Please use the form below to submit any comments or feedback you have on this chapter. If you have any images that you think would make a good addition to this chapter, please also submit them below - you will be fully credited for all images used. Feedback formPlease note that the maximum upload size is 5MB, and larger images and video clips can be sent to [email protected] . CALL NOW FOR CONSULTATION (310) 285-9612  - Incisionless Otoplasty
- Non-Surgical Molding
- Rhinoplasty
- Revision Rhinoplasty
- Hair Transplant
- Salivary Gland / Parotid
- Sinus Surgery
- Thyroid & Parathyroid
- About Practice
INFO ON THE EAR - EAR PRESENTATIONDr. ruder in the press. INFO ON THE EARDevelopment of the ear begins during the first few weeks of pregnancy. At this time the developing fetus looks like a FISH with gills. As the shape of the auricle forms, the developing ear moves (migrates) from under the chin to its proper position on the skull. These two patients have auricles that failed to completely move from under the chin to the skull. This slide shows the proper position of the ear. The auricle should attain its adult size by age 8. The auricle should lie between the eyebrow and the bottom of the nose. It should not lie straight, but be parallel to the bride of the now. It should also lie approximately 6 cm (the average height of an adult ear) from the eye. As the ear is developing in the first few weeks of gestation its shape not only changes to that of a normal ear, but it moves from under the chin to it proper position on the skull. These two patient’s developing ears (auricles) failed to adequately move to their proper adult position. These diagrams picture the developing ear (auricle) from the first three weeks of pregnancy through the end of the third month of pregnancy. Initially the ear looks like “gills” on a fish. By the end of the third month of pregnancy, the ear has attained its adult shape. Concomitant developing organ systemsOther organ systems are also developing at the same time as the ear. Therefore the doctor must evaluate a Microtia child’s kidneys, heart, neck, and middle ear that may also be abnormally affected. Situations that may cause a child to have Microtia are - Mother having fevers during the first few months of pregnancy.
- Any genetic predisposition (family history of others with ear anomalies).
- Exposure to excessive radiation.
- Thalidomide
Microtia occurs in 1:7,000 children. 30% of affected children have Microtia in BOTH ears. 30% of affected children have OTHER congenital anomalies that must be searched for. Evaluation of susceptible organ systemsSeveral tests may be necessary to find other anomalies: - Ultrasound of the kidneys.
- Heart beats.
- X rays of the neck
- Hearing testing
Treacher Collins SyndromePatients with Treacher Collins Syndrome have other abnormalities of their face. Their ears are ”low set”, and their cheek bones have not properly developed. Goldenhar’s SyndromeThese patients often also have problems with their kidneys. This syndrome represents other developmental problems that can occur at the same time the outer ear (auricle) is developing. The facial nerve (nerve to the face) has not developed causing a paralysis of this patient’s right side of his face. The ears are also “low set” and mal-developed. Also there are often problems with the kidneys with these patients. Mandible and TMJOften one side of the face and jaw are smaller than the normal opposite side. This phenomenon is called “hemi-facial microsomia”. The auricle is not round, triangular, or square, but OVAL shaped. It is not flat, but is three dimensional consisting of THREE layers (concha, scapha, and helix). Using ones fingers many anomalies can be easily seen. Most Common Anomalies- Protruding ear
- Concha too deep
- Flattened helix
- Low lying crus helicis
- Overhanging helix
- Scapha too narrow
- Loss of fossa triangularis
- Ears low set
- Skin pocket too small
- Lack of cartilage
Gradation of DeformitiesThese patients illustrate the most common deformity from a protruding ear, to and ear that “falls over” upon itself because of poor structural support, to Microtia where parts of the ear are absent. Common Abnormalities (Dysmorphic)This patient with a “protruding” auricle has two major defects. There is inadequate “folding” of the antehelix fold, and the inner layer (concha) is excessively deep. Common Abnormalities (Dysplastic ears)Dysplastic ears do NOT have all of the “parts” present. Reconstruction requires making a new framework. Dysmorphic EarsWhen one uses their fingers to push the auricle backwards, many anomalies quickly come into view. Ear MoldingThese ears have all parts present, but only deformed. We can correct these problems with simple non surgical MOLDING procedures. However, reconstruction must be initialed within the first three days of birth while the ear cartilage is still soft and pliable. Conchal Excision and Suture SetbackThese deformities can be corrected WITHOUT incisions at age four . This patient excessively “protruding” ears were corrected using an “incisionless otoplasty” technique. No cuts (incisions) were made. Bandages were removed after ONE day. Conchal excision suture setbackThis patient was helped with INCISIONLESS Otoplasty Suture SetbackPost operative patient Dysplastic EarsThese problems require “open” surgery techniques to add support and add elements that are missing. Timing of ReconstructionThis is the most severe ear deformity where most of the parts of the auricle never developed. Another common anomaly with Microtia is no ear canal is present (atresia). Microtia ReconstructionIt is essential to properly place (position) the newly reconstruct ear. These photographs demonstrate that an improperly positioned ear will give less than acceptable results. A template is drawn over the normal opposite ear. This “map” is drawn on the Microtia side to ensure that the new ear framework is properly placed. Templates for Configuration of FrameworkA second template is copied from the normal ear to help us make the reconstructed ear look similar in shape and size to the normal ear.  Harvesting Rib GraftsPatients have a choice to either use their own tissue from their ribs, or to use a preformed biosynthetic Medpor framework. If ribs are used to construct a framework, the lower ribs are harvested. Cartilage FrameworkA three layered rib cartilage framework is sculptured to conform to the shape and size of the normal side. Creation of Subdermal PocketInsertion of drain, transposition of lobule. The ear lobe is moved to its proper position. Conchal Excavation & Creation of TragusCreation of tragus. - Skin graft from postauricular area
- Chrondrocutaneous graft
Elevation of FrameworkPlace the ear is elevated from the skull and a graft of skin is placed to gain “protrusion” of the ear. PRE OPERTIVE AND POST OPERATIVE MICROTIA RECONSTRUCTION. Identification of VascularityWe are now using a more effective procue that uses MEDPOR (a porous poly-ethylene framework) instead of ribs. This reconstruction is accomplished in only TWO to THREE outpatient procedures. We need to identify the vascularity of the blood vessels in the scalp as illustrated in this slide. Sculpturing of ImplantThe Medpor (porous polyethylene) framework is sculptured to match the size and shape of the opposite normal ear. Post Auricular Skin GraftA graft of skin in taken behind the normal ear to help “cover” the Medpor framework. Abdomenal Skin GraftAnother graft of skin is taken from the “belly’ also to cover the Medpor framework. Skin Graft from AbdomenThis skin graft from the belly is sutured to the back of the normal ear. Medpor ImplantThe sculptured Medpor implant is sutured into proper place. Temporoparietal Fascial FlapTissue from the scalp (temporoparietal fascia) is folded onto the Medpor framework. - Superior Temporal vessels
- 11 to 12 cm
- Facial nerve
- Folded over
TPFF CoverageThe temporoparietal fascia from the scalp is folded down and covers the Medpor framework. Placement of Skin GraftThe previously harvested skin graft is placed over the framework. Skin Graft with DrainsMedpor implant, complications. - Perichondritis
- Malposition
- Suture reaction
- Keloid/Hypertrophic scarring
 - CALL US (310) 285-9612
- CONTACT US »
- SCHEDULE APPOINTMENT »
- ABOUT PRACTICE
PRIVACY POLICY | TERMS & CONDITIONS Copyright © Robert O. Ruder M.D. 2022 All Rights Reserved.  - Congenital Ear Deformities
- Author: Carl H Manstein, MD, MBA, CPE; Chief Editor: Tang Ho, MD, MSc, FACS more...
- Sections Congenital Ear Deformities
- Practice Essentials
- History of the Procedure
- Epidemiology
- Pathophysiology
- Presentation
- Indications
- Relevant Anatomy
- Contraindications
- Laboratory Studies
- Imaging Studies
- Diagnostic Procedures
- Histologic Findings
- Medical Therapy
- Surgical Therapy
- Preoperative Details
- Intraoperative Details
- Postoperative Details
- Complications
- Outcome and Prognosis
- Future and Controversies
- Media Gallery
Approximately 5% of the population has some sort of ear malformation. Protruding ear and external ear microtia (or a variant) are the two most frequently encountered congenital ear problems in plastic surgery. The former condition is commonly treated by many practitioners, while the latter has become the bailiwick of just a few surgeons. Most of this discussion focuses on prominent ears because of their common occurrence. Otoplasty has undergone important developments, with numerous techniques being presented in the surgical literature. Congenital ear microtia and atresia is treated in only a few centers by surgeons with an established reputation, similar to the way some centers specialize in craniofacial osteotomy surgery. Examples of preoperative and postoperative otoplasty are shown in the images below.  An observational study by Litschel et al indicated that when viewing a face with protruding ears, observers tend to have a longer visual fixation time on the ears than they do when viewing an individual with nonprotruding ears but that protruding ears do not significantly affect the observer’s opinion of an individual’s personality with regard to assiduousness, intelligence, and likeability. The study involved 20 observers who viewed photos of children with either protruding or nonprotruding ears. [ 1 ] Historically, prominent or protruding ears have been treated surgically. However, nonsurgical techniques have emerged to treat neonates immediately after delivery. [ 2 ] The posterior helical rim is taped to the posterior retroauricular region with surgical tape. Tubular elastic net bandage or some type of ear wrap is used for reinforcement. To achieve the desired result, such techniques must begin in the first few weeks of life and take several weeks or months of constant and vigilant therapy. Surgical techniques employed in the correction of prominent or protruding ears include the following: - Skin excision
- Radial placed mattress sutures
- Conchomastoid sutures
- Excision of conchal cartilage
- Incisionless and sutureless methods - Authors have elaborated on techniques in which the cartilage of the ear is split without sutures [ 3 ] and the incisionless otoplasty technique [ 4 ]
- Laser-assisted cartilage reshaping
Many different approaches to setback otoplasty have been developed. Originally, the first operations were merely resection of skin from the posterior sulcus. Approximately 200 different techniques have now been described for setback otoplasty; each technique has strengths and weaknesses. Over the years, an evolution of operations has occurred, including those with and without sutures, with and without resection of cartilage, and with or without scoring of cartilage. With this many variations, no single "right" technique exists. Microtia as a modern operation was first pioneered by Tanzer from Dartmouth Medical School. Tanzer was the first to develop the technique of using a whole piece of rib cartilage to simulate the cartilaginous structure of the external ear. Burt Brent from Stanford, Calif, expounded upon Tanzer's work and has written extensively about microtia reconstruction. The expression "beauty is in the eye of the beholder" is often quoted and still quite relevant. What constitutes a prominent ear? Ray Elliot stated in his 1990 review article in Clinics of Plastic Surgery, "the esthetic ear protrudes less than 2 cm when measured from the surface of the helix to the mastoid scalp at the midpoint of the ear's length." [ 5 ] However, once this measurement achieves a distance of less than 1.2 cm, the ear has an equally displeasing "pinned back" appearance. The ear protrudes more at the lower pole and less so at the upper pole because of the shape of the skull. The scaphoconchal angle should have a natural soft roll and should not block the view of the helix anywhere along its course when viewed anteriorly. No statistics are available on the prevalence of protruding or prominent ears. Heredity plays a role in many deformities of the external ear. Most embryologic studies of the ear focus on the development of the 6 ear hillocks. These hillocks appear around the fundus of the first branchial groove by 38 days of gestation. As the groove closes and the first and second arches come together, the primitive ear is formed by day 50 of gestation. The first 3 hillocks come from the first branchial arch and the second 3 from the second branchial arch. Absence of hillocks 2-5 produces a frequent and typical microtia. Malformations of the ear can appear anywhere during this development. Features seen in the patient with prominent or protruding ears (in decreasing order of importance) include the following: Absent antihelical fold Obtuse scaphoconchal angle Increased distance of helical rim to scalp Deep conchal bowl Address some or all of these problems in the planning and execution of the operation to correct the abnormality. Auricular anatomy in children varies only slightly from that in adults. By the third year, 85% of ear growth and development occurs, and little growth occurs after 10 years. The ear's height may increase gradually into adulthood but its distance from the scalp changes little after 10 years. Because of this, setback otoplasty can safely be performed on children as young as 5-6 years. Most parents, while emotionally distressed when their baby is born with a portion of the external auricle missing or severely distorted, are unconcerned about protruding ears at birth. Patients tend to seek surgical opinion for protruding ear problems at two stages of life. Parents often seek medical advice for their children at the start of school because of the child's complaints of classmates' teasing. The jeer of "Dumbo" is difficult for a first grader. The second group of patients consists primarily of women in their twenties or early thirties. These patients also are embarrassed about their protruding ears. For the child born without an external ear, the indications for surgical reconstruction are obvious. Parents are anxious to proceed as soon as possible to spare their child any embarrassment. Unlike cleft lip surgery, which is performed in the first few weeks of life, most experienced surgeons recommend waiting to do multistages at age 6-7 years. The more important question is not whether surgery is indicated, but which of the techniques for reconstruction is indicated for the individual. Even with microtia, the physiologic effects of an ear deformity are negligible. The aesthetic and psychological effects are significant. [ 6 ] In the patient born with a prominent ear or deformity, the situation may be a little different. With the obtuse scaphoconchal angle and absent antihelical fold, distance from the helical rim varies. Many authorities believe the external ear should protrude no more than 2 cm from the surface of the helix to the mastoid scalp at the midpoint of the ear's length. This measurement is a guide and not an absolute rule. Much depends upon the patient's expectations as well as the surgeon's experience. Although congenital absence is almost always unilateral, patients with prominent ears usually require a bilateral operation. Children with protruding ears generally do well when operated on as early as age 5-6 years. A study from the Medical College of Wisconsin presented a series of 12 patients in whom otoplasty was performed before the age of 4 years with good results. [ 7 , 8 ] Taunts from schoolmates begin at this time. Parents, not realizing how cruel kindergarten children can be, are often oblivious to this ridicule. Young girls reveal much less of this mental anguish because they are able to wear their hair long and cover their ears. They never wear a ponytail, lest a peer discovers their ears stick out. In this author's practice, a common indication for setback otoplasty is the approximately 20-year-old woman who is getting married and now wants to wear her hair in an upswept fashion. Boys do not have that option. Because of a genetic predisposition to protruding ears, some parents find that seeking plastic surgical consultation for their children is difficult. To admit his or her child is flawed, the parent must admit he or she is flawed. Nerve supply of the external earSee the list below: Great auricular nerve (C2, C3) - Lower half of ear Auriculotemporal nerve (from mandibular brand of trigeminal) - Tragus, anterior/superior portions of auricle Lesser occipital nerve (C2, C3) - Posterior/superior aspect of ear Auricular branch of vagus nerve (Arnold nerve) - Concha and posterior auditory canal Anatomy of the normal earWidth of ear equals approximately 55% of length Helix-to-mastoid distance - Upper third equals 10-12 mm; middle third equals 16-18 mm; lower third equals 20-22 mm Sides should be within 3 mm of each other Axis of ear is parallel to profile of nose The ear can be difficult to reproduce surgically because only a thin layer of skin covers the cartilaginous structure. [ 9 ] This cartilaginous structure is attached to the temporal bone medially by several minor intrinsic muscles. A looser attachment of skin is found upon the posterior aspect of the auricle than the anterior aspect of the auricle. The vascular supply comes from the superficial temporal and posterior auricular vessels. Corresponding veins drain the ear. A study by Oliveira et al stated that a natural plica can be found at the anatomic base of the antihelix, with the creation of this plica being an important part of antihelix reconstruction in patients with protruding ears. [ 10 ] Prominent or protruding earsIncreased scaphoconchal angle Increased distance from helical rim to scalp Flattening of superior crus Normal helical length Cup ear deformity (lop-ear, constricted ear)Flattening of antihelix Widening of concha Overhang of helix Compression of scapha and fossa triangularis Indistinct antihelix and crura Shortened length of helix Ear appears small, but no difference in size Absence of retroauricular sulcus, causing the superior pole of ear to appear buried Sharply curved antihelical crus No foreshortening of auricle Presence of third crus Flat antihelix Malformed scaphoid fossa Contraindications for treatment of prominent ears include the following: Unreasonable expectations from either patient or family Child younger than 5 years Patient who is unable to tolerate postoperative wound care, including a protective bandage head wrap Patient who opposes the operation despite his or her parents' wishes to proceed Litschel R, Majoor J, Tasman AJ. Effect of protruding ears on visual fixation time and perception of personality. JAMA Facial Plast Surg . 2015 May-Jun. 17 (3):183-9. [QxMD MEDLINE Link] . Matsuo K, Hayashi R, Kiyono M, et al. Nonsurgical correction of congenital auricular deformities. Clin Plast Surg . 1990 Apr. 17(2):383-95. [QxMD MEDLINE Link] . Obadia D, Quilichini J, Hunsinger V, Leyder P. Cartilage splitting without stitches: technique and outcomes. JAMA Facial Plast Surg . 2013 Dec 1. 15(6):428-33. [QxMD MEDLINE Link] . Strychowsky JE, Moitri M, Gupta MK, Sommer DD. Incisionless otoplasty: a retrospective review and outcomes analysis. Int J Pediatr Otorhinolaryngol . 2013 Jul. 77(7):1123-7. [QxMD MEDLINE Link] . Elliott RA Jr. Otoplasty: a combined approach. Clin Plast Surg . 1990 Apr. 17(2):373-81. [QxMD MEDLINE Link] . Gosain AK, Kumar A, Huang G. Prominent ears in children younger than 4 years of age: what is the appropriate timing for otoplasty?. Plast Reconstr Surg . 2004 Oct. 114(5):1042-54. [QxMD MEDLINE Link] . Gosain AK, Recinos RF. Otoplasty in children less than four years of age: surgical technique. J Craniofac Surg . 2002 Jul. 13(4):505-9. [QxMD MEDLINE Link] . Janz BA, Cole P, Hollier LH Jr, Stal S. Treatment of prominent and constricted ear anomalies. Plast Reconstr Surg . 2009 Jul. 124(1 Suppl):27e-37e. [QxMD MEDLINE Link] . Furnas DW. Complications of surgery of the external ear. Clin Plast Surg . 1990 Apr. 17(2):305-18. [QxMD MEDLINE Link] . Oliveira MM, Oliveira DS, Oliveira GS. The Existence of a Natural Plica at the Anatomical Base of the Antihelix and its Surgical Importance to Address Protruding Ears: An Anatomicosurgical Study. Aesthetic Plast Surg . 2017 Apr. 41 (2):321-6. [QxMD MEDLINE Link] . Feijen MMW, van Cruchten C, Payne PE, van der Hulst RRWJ. Non-surgical Correction of Congenital Ear Anomalies: A Review of the Literature. Plast Reconstr Surg Glob Open . 2020 Nov. 8 (11):e3250. [QxMD MEDLINE Link] . [Full Text] . Erol OO. New modification in otoplasty: anterior approach. Plast Reconstr Surg . 2001 Jan. 107(1):193-202; discussion 203-5. [QxMD MEDLINE Link] . Furnas DW. Correction of prominent ears with multiple sutures. Clin Plast Surg . 1978 Jul. 5(3):491-5. [QxMD MEDLINE Link] . Taboada-Suarez A, Brea-Garcia B, Couto-Gonzalez I, Vila-Moriente JL. Correction of protruding ears (Weerda grade I deformity) using knotless bidirectional barbed absorbable sutures. Otolaryngol Head Neck Surg . 2014 Dec. 151 (6):939-44. [QxMD MEDLINE Link] . Bauer BS, Song DH, Aitken ME. Combined otoplasty technique: chondrocutaneous conchal resection as the cornerstone to correction of the prominent ear. Plast Reconstr Surg . 2002 Sep 15. 110(4):1033-40; discussion 1041. [QxMD MEDLINE Link] . Leclere FM, Vogt PM, Casoli V, Vlachos S, Mordon S. Laser-assisted cartilage reshaping for protruding ears: A review of the clinical applications. Laryngoscope . 2015 Sep. 125 (9):2067-71. [QxMD MEDLINE Link] . Orabona GD, Salzano G, Maglitto F, Seidita F, Abbate V, Califano L. Do combined otoplasty techniques really improve the surgical outcomes for prominent ear correction in adult patients?. Ann Ital Chir . 2018. 89:157-61. [QxMD MEDLINE Link] . Hendrickx BIMM, Hamdi M, Zeltzer A, Greensmith A. The 'WiFi' otoplasty : Combined concentric posterior microchondrectomies and sutures for correction of prominent ears. J Plast Reconstr Aesthet Surg . 2018 Jun. 71 (6):900-5. [QxMD MEDLINE Link] . Binet A, El Ezzi O, De Buys Roessingh A. A retrospective analysis of complications and surgical outcome of 1380 ears: Experience review of paediatric otoplasty. Int J Pediatr Otorhinolaryngol . 2020 Nov. 138:110302. [QxMD MEDLINE Link] . [Full Text] . Kadhum M, Atherton S, Jawad A, Wilson-Jones N, Javed MU. A Retrospective Analysis of Pinnaplasty Outcomes: The Welsh Experience. Facial Plast Surg . 2023 Sep 14. [QxMD MEDLINE Link] . Carvalho C, Marinho AS, Barbosa-Sequeira J, Correia MR, Banquart-Leitão J, Carvalho F. Quality of life after otoplasty for prominent ears in children. Acta Otorrinolaringol Esp (Engl Ed) . 2023 Jul-Aug. 74 (4):226-31. [QxMD MEDLINE Link] . - Preoperative otoplasty.
- Two years after otoplasty.
- Postoperative otoplasty.
Contributor Information and DisclosuresCarl H Manstein, MD, MBA, CPE Private Practice Carl H Manstein, MD, MBA, CPE is a member of the following medical societies: Pennsylvania Medical Society , Sigma Xi, The Scientific Research Honor Society , American Society of Plastic Surgeons Disclosure: Nothing to disclose. Francisco Talavera, PharmD, PhD Adjunct Assistant Professor, University of Nebraska Medical Center College of Pharmacy; Editor-in-Chief, Medscape Drug Reference Disclosure: Received salary from Medscape for employment. for: Medscape. Jaime R Garza, MD, DDS, FACS Consulting Staff, Private Practice Jaime R Garza, MD, DDS, FACS is a member of the following medical societies: Alpha Omega Alpha , American Academy of Otolaryngology-Head and Neck Surgery , American College of Surgeons , American Society for Aesthetic Plastic Surgery , American Society of Maxillofacial Surgeons , Texas Medical Association , Texas Society of Plastic Surgeons Disclosure: Received none from Allergan for speaking and teaching; Received none from LifeCell for consulting; Received grant/research funds from GID, Inc. for other. Tang Ho, MD, MSc, FACS Chief, Division of Facial Plastic and Reconstructive Surgery, Associate Professor, Department of Otorhinolaryngology-Head and Neck Surgery, University of Texas Health Science Center at Houston, McGovern Medical School Tang Ho, MD, MSc, FACS is a member of the following medical societies: American Academy of Facial Plastic and Reconstructive Surgery , American Academy of Otolaryngology-Head and Neck Surgery , American College of Surgeons , Chinese American Doctors Association of Houston , Harris County Medical Society , Houston Society of Otolaryngology - Head and Neck Surgery , Johns Hopkins Medical and Surgical Association , Texas Association of Otolaryngology - Head and Neck Surgery , Texas Medical Association Disclosure: Nothing to disclose. Lawrence Ketch, MD, FAAP, FACS Head, Program Director, Associate Professor, Department of Surgery, Division of Plastic Surgery, University of Colorado Health Sciences Center; Chief, Pediatric Plastic, The Children's Hospital of Denver Lawrence Ketch, MD, FAAP, FACS is a member of the following medical societies: American Academy of Pediatrics , American Association for Hand Surgery , American Association of Plastic Surgeons , American Burn Association , American Cleft Palate/Craniofacial Association , American College of Surgeons , American Society for Surgery of the Hand , American Society of Maxillofacial Surgeons , American Society of Plastic Surgeons , Association for Academic Surgery , andPlastic Surgery Research Council Disclosure: Nothing to disclose. What would you like to print?- Print this section
- Print the entire contents of
- Print the entire contents of article
- Mondini Deformity
- Aural Atresia of the External Ear
- Syndromic Sensorineural Hearing Loss
- Aural Atresia
- Ear Reconstruction
- Can AI Tool Improve Dx of Ear Infections?
- Crinecerfont Promising for Congenital Adrenal Hyperplasia
- SGLT2 Inhibitors Safe for HF in Congenital Heart Disease
- Dorsal Augmentation: A Review of Current Graft Options
 - Drug Interaction Checker
- Pill Identifier
- Calculators
 Skip to content Ear DeformitiesEar deformities program, what are ear deformities. Abnormal development or deformities of the ear anatomy can cause a range of complications, from cosmetic issues to hearing and development problems. An estimated 6 to 45 percent of children are born with some sort of congenital ear deformity. Some ear deformities are temporary. If the deformity was caused by abnormal positioning in the uterus or during birth, it may resolve as the child grows, the ear unfolds and takes on a more normal form. Other ear deformities will need medical intervention – either nonsurgical or surgical – to correct the ear anomaly. Because it’s unknown which ear deformities will correct on their own and which will not, it’s important to discuss treatment options as early as possible. At The Children's Hospital of Philadelphia, experienced otolaryngologists and plastic surgeons assess and treat infants, children and adolescents with a wide variety of ear deformities. Normal external ear anatomy The ear is made primarily of cartilage covered by skin. The earlobe has no cartilage and is made of skin and fat. Although there are some muscles attached to the ear, most people cannot control them, which is why only a small percentage of people can wiggle their ears. The external ear is supplied by four different sensory nerves. Types of ear deformitiesThere are several varieties of congenital ear deformities, including: - Protruding ears (also called prominent ears): Ears that, regardless of size, stick out more than 2 cm from the side of the head
- Constricted ears : A variety of ear deformities where the helical rim is either folded over (also called lop ear), wrinkled, or tight
- Cryptotia : Ear cartilage framework that is partially buried beneath the skin on the side of the head
- Microtia : Underdeveloped external ear
- Anotia : Total absence of the ear
- Stahl's ear Ears that have a pointy shape and an extra cartilage fold (crus) in the scapha portion of the ear
- Ear tags : Also known as an accessory tragus or a branchial cleft remnant, ear tags consist of skin and cartilage
- Earlobe deformities : These come in a variety of shapes, including earlobes with clefts, duplicate earlobes, and earlobes with skin tags
- Traumatic ear deformities : Lacerations, tears and bite injuries.
- Split earlobes : Occur gradually due to large or heavy earrings
- Cauliflower ear : Abnormal cartilage forms on top of the normal cartilage, resulting in bulky misshapen ears
- Ear keloids : Caused by excessive scar tissue formation after minor trauma, most commonly after ear piercing
- Ear hemangiomas : Most common benign tumor of infancy, can occur anywhere on the body, including the external ear and the salivary gland in front of the ear.
The causes of ear deformities are varied. Most ear deformities are congenital, meaning they are present from birth. In rare cases, children develop ear deformities from trauma or disease. In some children, an ear deformity is a symptom of a genetic disorder that can affect multiple body systems, such as Goldenhar syndrome and CHARGE syndrome. Ear deformities can be inherited or caused by genetic mutations. Traditional treatment for ear deformities has been to wait until a child is 5 years old to perform surgical correction. However, we have learned that many of these deformities, if treated early, can be corrected nonsurgically with ear molding. Unfortunately, we do not know which ear deformities will correct by themselves and which will require surgical treatment later in life. For this reason, it’s important to discuss early nonsurgical ear molding with your child’s physician. Nonsurgical treatmentAt The Children’s Hospital of Philadelphia, we believe every child with an ear deformity at birth should be examined by an experienced multidisciplinary team to consider if nonsurgical treatment could improve the appearance of the child’s ear. Early intervention is crucial and may help children avoid surgery later. Because of the increased maternal estrogen levels seen in infancy, infant ears are very moldable, soft and responsive to external ear molding during the first few weeks and months after birth. Learn more about ear molding . Surgical treatmentFor children with ear deformities that do not respond or are not candidates for nonsurgical correction, surgery may be needed. A team of expert plastic and reconstructive surgeons from CHOP’s Ear Deformities Program will work with you and your child to determine when surgical intervention, such as ear reconstruction , will benefit your child. Reviewed by David W. Low, MD , Scott P. Bartlett, MD Auditory Milestones: From Birth to 2 YearsPublished by Farheen on May 27, 2021 May 27, 2021  Before we get down with our auditory milestones series, here are some very important statistics for you. - Did you know that according to the World Health Organization, by the year 2050, almost 2.5 billion people may face some degree of hearing-related issues and hearing loss? Consequently, they may even require some form of hearing rehabilitation?
- Did you know that 34 million children alone need auditory habilitation due to their hearing loss?
 What are pediatric auditory milestones?Auditory milestones are the baby’s behavioral responses to sounds. And it develops and matures with the child’s physical and intellectual growth. These behaviors may correspond to a child’s cognitive maturation with age. These auditory responses build receptive language. So here we go on our discovery of pediatric auditory milestonesThe fetus starts hearing in the mother’s womb around 18 weeks of development. Ears’ structure is developed by 24 weeks of pregnancy. Inevitably, the newborn has exposed to the sound long before his birth. Below we present to you auditory milestones from 3 months to age two years old. Pediatric Auditory Milestones: From birth to 3 months| | | | | Firstly your child may react when presented with loud sounds through a startle reflex. | Consequently, the baby can also indulge in cooing sounds now. | | | Secondly, the baby may quiet, even soothed by the presentation of soft sounds. | Accordingly, the infant can change his crying tones for a variety of his needs. | | | Moreover, when you speak to her/him, s/he may turn his head towards you. | Necessarily, the smile to the newborn also contributes to his auditory-verbal skills development and maturation because it builds a social connection between you and your child. | |
also see: http://terteeb.org/blog/2021/05/24/joint-attention-an-important-tool-for-communication-cognition-development/  Overall, by the 3 months of a baby’s auditory skills maturation, an infant may awake by loud sounds and voices. However, by that time, s/he learns to smiles at you when he/she is spoken to. Also, the baby recognizes your voice, and your presence makes her/him calm down. Pediatric Auditory Milestones: From 3 to 6 Months| | | | Firstly he turns or looks towards a new sound | subsequently, the child learns babbles or coos to interact while playing with you or by him/herself | | Secondly, he seems also to recognize the voice tone changes of his parents. | As a result, his babbling seems more speech-like at this stage. Additionally, these sounds include utterances of syllables like , , and . | | Furthermore, your child now laughs and giggles in response to interaction. Congratulation, your baby is showing the sign of social cognitive development. | | Moreover, he may imitate after your action. | Over all by making sounds, he informs you if he/she is happy or upset. | | Lastly, a loud voice or noise may scare him. | Initiates repeating sounds through vocalization and babbling(aah, ooh, and ba-ba, ma-ma. He is building his phonological repertories with all passing days. |
 Pediatric Auditory Milestones: From 7 to 12 months| | | | Firstly a 7-month-old baby may respond when his/her name is called. Furthermore, he may run to pick up the ringing telephone. Even more, he may even respond to someone’s soft voice, | Babbling along certain sound strings emerge with more confident utterances “up-up, ,mamaaamaaama
| | Secondly, s/he may know some common nouns, including cup, phone, glass, shoe, and may even say hi, bye-bye, give, etc. | To gain and maintain attention, uses gestures and sounds. | | Next your baby babbles even when s/he is alone | When shown, objects point towards them to lead others. | | Now the child may respond to your requests such as come, give and go there. | Additionally, your baby now gestures to communicate like waving bye, hi. Furthermore, now he reaches for things up or down and nods his head for ‘ .’ | | Lastly, your child may look at pictures of things or when hears someone refers to them. | Moreover, your baby independently imitates various speech sounds. | | consequently, an infant utters 1 or 2 words with slight intelligibility, like , , or , at the time of his first birthday, |
also see about joint attention: http://terteeb.org/blog/2021/05/24/joint-attention-an-important-tool-for-communication-cognition-development/ Pediatric Auditory Milestones: Red Flags- The baby does not turn his head towards noises.
- The baby does not wake up when TV is on at a loud level.
- You need to check if the baby can hear properly. See the audiologist to rule out hearing impairment. Furthermore, you need to focus on any ear infections and consult your physician.
 Home Activities to Develop Auditory and Listening Skills (Birth -1 year)There are some activities that facilitate listening skills in your baby. - Respond to your child’s cry. In other words, by looking at him as he/she is busy making noises.
- You can talk to him and see if he pays attention, then You and your baby can take a turn in babbling.
- You can also teach your baby to imitate your actions and gestures.
- Games such as peek-a-boo, blowing kisses, clapping enhance communication skills.
- Talk to the baby as you bathe him/ her.
- Feeding time is an excellent opportunity for you to interact with your baby.
- Since talking increases baby’s communication skills, so you can use phrases such as” mom is going to brush your hair, or mom is going to make your milk, etc..”
- Additionally, while communicating, please make sure to take your child’s name, so he feels important.
- Talk to your child about where you are going, everything that you are doing there, and who and whatever you see there. “Like mom and baby are going to park, we will have fun there. We will see birds, etc.”.
- You can enhance auditory and verbal skills by teaching animal sounds like “lion goes roar, the duck says quack.”
- Additionally, reading daily to your baby develops listening and verbal skills in your child.
 Pediatric Auditory Milestones: From 1 to 2 years| | | | | Firstly, your child can point to a few body parts when asked to. | Consequently, the child can now use a variety of new words. | | | Secondly, your child can now follow commands such as “pick up the ball” or “Kiss the teddy.” | Furthermore, his speech now includes /b,m,h, , and / in his words. | | | Thirdly, at this stage, your child may answer your simple questions, such as “Where’s your ball?” or “Who’s that?” | Most importantly, he/she names pictures in books. | | | Above all your little one may now enjoy listening to short stories, nursery rhymes, and songs | In addition, to this, your child may be able to ask you simple WH questions, for example, “Who’s that?”, “What’s that?” and “Where’s doggy?” | | | As a result of you naming a picture in a book during story time, your child points to the exact pictures. | Furthermore, your one-year-old child may make a 2-word phrase such as”more milk,” “no food,” and “mommy ball.” | | | | |
 Home Activities to Develop Auditory and Listening Skills(1 -2 years). - Firstly, you may talk to your child while doing house chores or running errands like the grocery store. In other words, while shopping or taking a walk, point towards what you see, name it. For example, if you see a cat, you can say, “I see a cat. The cat says ‘meow.’ it’s a big cat. This cat is black.”
- Secondly, you can use short words and sentences that your child can imitate. In addition to this, you need to use correct grammar.
- Thirdly it is highly recommended that you talk about the different sounds heard around your house.
- In other words, when you listen to the tick of the clock, you can imitate the clock with a tick, “t-t-t.” utterance.
- You can also play with a variety of sounds during bath time. You need to be at eye level with your baby. Have fun blowing bubbles while making the “b-b-b-b” sound. Pop the bubbles making a “p-p-p-p” sound. While playing with toy engines, you both can make the “rrr-rrr-rrr” sound.
- Increase your child’s vocabulary through his auditory skills. If the child says “car,” that is a small blue car.”
- Moreover, you can read to your child daily.
- The larger the books, the better the results.
- Furthermore, while reading, you can also talk about all the pictures on every page, every detail with great excitement.
 Conclusion:We hope that our activities are fruitful for you. Try them out at home and do let us know of any issues you may be facing while practicing them. One of the most important things to remember is that during these activities you need to be very consistent in your practices. References :https://childrensnational.org/visit/conditions-and-treatments/ear-nose-throat/ageappropriate-hearing-milestones https://www.scholastic.com/parents/kids-activities-and-printables/activities-for-kids/activities-explore-hearing-0-2-year-olds.html https ://www.asha.org/public/speech/development/01/ Capute, A. J., & Accardo, P. J. (1978). Linguistic and auditory milestones during the first two years of life: a language inventory for the practitioner. Clinical pediatrics , 17 (11), 847-853. McMahon, E., Wintermark, P., & Lahav, A. (2012). Auditory brain development in premature infants: the importance of early experience. Annals of the New York Academy of Sciences , 1252 (1), 17-24. Datta, G., Odell, A., & Durbin, K. (2010). Nottingham auditory milestones: a profile to monitor the growth of active listening, understanding, auditory memory, and sequencing in babies and young children in the first three years after receiving cochlear implants. Cochlear implants international , 11 (sup1), 282-285. 33 Comments Samia · June 2, 2021 at 2:36 pmWell written and highly Informative  Farheen · June 2, 2021 at 3:19 pmJazakAllah bil Khair  Ambreen Naz · June 2, 2021 at 7:19 pmVery nicely written, easy and understandable explanation. I will suggest parents for young children to go through with that website on regular basis. Because the article and information shared on websites it is not only beneficial for parents of atypical children but also good for parents of typical children. All the parents should know the typical cycle of milestones to discriminate from odd to even. Hatts of to the writer! Farheen · June 3, 2021 at 1:49 amThank you so much for your appreciation and recommendation. That means a lot to my team and me.  Mrs.Aulakh · July 6, 2021 at 3:16 amSoooo nicely explained.very informative as usual.beneficial for many new parents also who struggling with their children who having profound hear loss… Dear Farheen your knowledge n experience is vast..My lovely wishes for you.. And thank you to helping where no one can guide you are a hope for world.. salute to your kindness n love for humanity…  panaloko gaming · November 3, 2023 at 1:48 pmSaved as a favorite, I love your site!  cipit88 · November 3, 2023 at 7:59 pmGreat post.  Lamar · November 3, 2023 at 9:07 pmPretty component of content. I simply stumbled upon your website and in accession capital to say that I acquire in fact enjoyed account your blog posts. Anyway I will be subscribing to your augment and even I success you access persistently fast.  유로247가입주소 · November 3, 2023 at 10:21 pmExcellent post. I was checking continuously this blog and I’m impressed! Very useful information particularly the last part 🙂 I care for such information a lot. I was looking for this particular info for a long time. Thank you and best of luck.  دوربین مداربسته · November 14, 2023 at 7:15 amThis piece of writing is genuinely a nice one it assists new internet people, who are wishing in favor of blogging. Farheen · November 22, 2023 at 2:10 amThank you so much for your kind words! We’re thrilled to hear that you found our content helpful and that you’re considering returning for more. Your encouragement means a lot to us. We’re dedicated to providing valuable and informative content, so your feedback inspires us to keep delivering. We look forward to having you back and hope you continue to find our website beneficial. If you have any specific topics you’d like us to cover in the future, feel free to let us know. Thanks again for your support! Farheen · November 22, 2023 at 2:12 amAbsolutely! Unpredicted feelings can often lead to some of the most genuine and authentic insights on various topics. We aim to capture and preserve those moments of un-ambiguity and raw emotions, translating them into valuable knowledge that resonates with our readers. It’s fantastic to hear that you found value in this aspect of our content. Thank you for sharing your thoughts! Farheen · November 22, 2023 at 2:20 amThank you all immensely for your incredibly kind words and appreciation! Your support means the world to us. We’re thrilled that our content resonates with you and that you’ve found the information valuable and well-explained. Your encouragement motivates us to keep delivering top-notch content. We truly appreciate each one of your comments and the time you’ve taken to share your thoughts. Please continue enjoying our posts, and if there’s anything specific you’d like us to cover, feel free to let us know. Thanks once again for your fantastic support! Farheen · November 22, 2023 at 2:23 amThank you for your kind words! We’re delighted to hear that you enjoyed your visit to our site. Your bookmark means a lot to us, and we’re thrilled that you’re considering returning. We’ll continue to work hard to provide valuable content that keeps you engaged. If there’s anything specific you’d like to see or if you have any feedback, feel free to let us know. Looking forward to having you back! Farheen · November 22, 2023 at 2:26 amThank you so much for your comment! We’re thrilled that our content aligns with your presentation topic. It’s fantastic to hear that you found the information here helpful for your upcoming academy presentation. If there’s anything more you need or if you have any specific questions related to your topic, feel free to reach out. Wishing you the best with your presentation – you’ve got this Farheen · November 22, 2023 at 2:28 amThank you for your kind words! We’re thrilled that you found our webpage post useful and packed with valuable information. Providing helpful content is what we aim for, and knowing it’s been beneficial to you makes it all worthwhile. If there’s anything specific you’d like to see more of or any questions you have, don’t hesitate to let us know. We appreciate your support! Farheen · November 22, 2023 at 2:30 amThank you for your wonderful comment! We’re thrilled that you appreciate our unique style. It means a lot to us that you’ve decided to bookmark our website. We strive to offer a distinct perspective and valuable content. If there’s anything specific you’d like to see more of or any feedback you have, feel free to share. We’re excited to have you as part of our community and look forward to providing more insightful content in the future!  real money poker sites · November 28, 2023 at 8:54 pmHello, I believe your blog may be having internet browser compatibility problems. Whenever I look at your web site in Safari, it looks fine however, if opening in IE, it has some overlapping issues. I merely wanted to give you a quick heads up! Aside from that, excellent website!  https://www.helpware.com/ · November 28, 2023 at 10:32 pmNice post. I learn something totally new and challenging on websites I stumbleupon on a daily basis. It’s always helpful to read content from other writers and use a little something from their web sites.  เว็บสล็อตออนไลน์ · December 2, 2023 at 5:05 pmYou actually make it seem so easy with your presentation however I to find this matter to be actually one thing that I believe I’d by no means understand. It sort of feels too complex and extremely wide for me. I’m looking forward in your next put up, I’ll attempt to get the dangle of it!  Major Model Agencia de Modelos · December 2, 2023 at 8:57 pmWonderful blog! I found it while searching on Yahoo News. Do you have any suggestions on how to get listed in Yahoo News? I’ve been trying for a while but I never seem to get there! Thank you  Blanca · December 6, 2023 at 4:20 amI don’t even understand how I stopped up right here, but I believed this post used to be good. I don’t understand who you might be however certainly you’re going to a well-known blogger when you are not already. Cheers!  amatricescams.com · December 6, 2023 at 12:25 pmYou really make it seem so easy with your presentation but I find this topic to be really something that I think I would never understand. It seems too complex and extremely broad for me. I am looking forward for your next post, I will try to get the hang of it!  Gilbert · December 7, 2023 at 10:43 pmWhat’s up, its fastidious article on the topic of media print, we all be familiar with media is a fantastic source of data.  토토사이트 · December 10, 2023 at 3:32 amAttractive section of content. I just stumbled upon your blog and in accession capital to assert that I acquire in fact enjoyed account your blog posts. Any way I will be subscribing to your feeds and even I achievement you access consistently fast.  situs bokep jepang · December 10, 2023 at 11:02 amThis ѡeb site trulү has all the informatіon I needed about this subject and didn’t know who to ask.  slot pulsa · December 12, 2023 at 1:48 amHi there! This is my 1st comment here so I just wanted to give a quick shout out and say I truly enjoy reading your blog posts. Can you recommend any other blogs/websites/forums that cover the same subjects? Thank you so much!  cipit88 · December 14, 2023 at 6:39 amI think this is one of the most significant information for me. And i’m glad reading your article. But should remark on some general things, The website style is perfect, the articles is really excellent : D. Good job, cheers  cipit88 · December 14, 2023 at 8:15 amHowdy! Would you mind if I share your blog with my zynga group? There’s a lot of folks that I think would really appreciate your content. Please let me know. Thanks  latest 2024 xxx videos free download · December 15, 2023 at 6:32 amI blog frequently and I truly thank you for your information. Your article has truly peaked my interest. I am going to book mark your blog and keep checking for new details about once per week. I subscribed to your RSS feed too.  cto services · December 16, 2023 at 4:55 amThank you for the auspicious writeup. It if truth be told was a leisure account it. Look complicated to far delivered agreeable from you! However, how can we keep in touch? Prelinguistic skills: What skills should I look for? - Terteeb · June 2, 2021 at 9:39 am[…] http://terteeb.org/blog/2021/05/27/pediatric-auditory-milestones-birth-to-2-years/ […] Leave a Reply Cancel reply Your email address will not be published. Required fields are marked * Save my name, email, and website in this browser for the next time I comment. Related Posts Speech & CommunicationAuditory milestones: from 2-3 years old. Listening skills are crucial for the achievement of auditory milestones. Yes, you got it right! Hearing though is necessary but not enough to develop auditory milestones. The hearing ability of your child provides crucial sensory Read more…  Listening Skills & Auditory Milestones : 3-5 Years old.Most children achieve auditory milestones and sharpen their listening skills at their own pace. However, there are specific age ranges for each milestone; therefore, your child might not have developed all or most of the Read more…  Sensory Processing Disorders & Picky EatersGeneral overview of swallowing disorder: Dysphagia Feeding preferences make children picky eaters. Sensory processing disorder and ASD impact daily living activities, including mealtime. Sensory processing disorder leads to dysphagia, a swallowing disorder. If a person Read more…  An official website of the United States government The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site. The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely. - Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now . - Advanced Search
- Journal List
- v.15(5); 2023 May
- PMC10310060
 Ectopic Unilateral Ear Pit in an Otherwise Well-Appearing Child: A Case Report and Literature ReviewHenry h nguyen. 1 Pediatrics, University of Illinois at Chicago, Chicago, USA 2 Pediatrics, The University of Chicago Medicine, Chicago, USA Sydney MartinLeslie jabine. Ear pits are a common congenital abnormality that is incidentally found on routine examinations. However, it is not well documented how many are found outside of their classical location or if these ectopic locations put patients at increased risk of having a hearing impairment, renal anomalies, genetic syndromes, or infection. Clinicians should be aware of the current guidelines for recognizing, screening, and evaluating for these risks in patients with ear pits, regardless of location. IntroductionPreauricular pits, also known as preauricular fistulas, preauricular tracts, preauricular cysts, ear pits, or ear sinuses, were first described in 1864 by Heusinger on a routine physical exam [ 1 ]. These common congenital abnormalities are small invaginations of stratified squamous epithelium, typically found on or adjacent to the auricle of the external ear. They are usually asymptomatic but are prone to infection. The estimated incidence of preauricular pits is 0.1-0.9% in the United States, occurring predominantly in Asian-American children (10%), African-American children (5%), and Caucasian-American children (1%) [ 2 - 6 ]. Ear pits can be found unilaterally or bilaterally. They can occur in isolation or in association with certain genetic syndromes, such as Branchio-Oto-Renal (BOR) syndrome. Patients with ear pits are also at increased risk of having hearing loss and/or renal abnormalities. Although current literature suggests no workup is needed for isolated ear pits, auditory testing and renal ultrasound may be useful for patients with an increased risk of hearing loss and renal dysfunction [ 4 , 6 ]. Medical and surgical management is typically reserved for patients with infected pits. In this article, we will briefly summarize the epidemiology, embryology, clinical significance, evaluation, and management of ear pits and address the question of whether variant ear pits have an increased relationship with hearing loss, kidney anomalies, and genetic syndromes. Case presentationA two-year-old male with well-controlled, moderately persistent asthma and eczema was brought into our pediatric clinic by his mother after she found a hole in his left outer ear while giving him a bath. This was the first time the mom noticed it, and there were no documented ear pits on prior well-child visits upon chart review. Mom reported no issues or changes to his hearing; no otalgia, fever, or drainage from the orifice. There was no recent trauma to the ear. The patient had normal speech development, and there was no history of frequent otitis media or externa. There were also no urinary symptoms or histories of urinary infections. There was no family history of hearing loss, ear pits, or genetic syndromes. On physical exam, the patient was afebrile and well-appearing. He had no apparent dysmorphic features. There was a small hole similar to an ear pit in the concha, just inside the external auditory meatus on the anterior portion of the external auditory canal of the left ear, without any drainage or surrounding inflammation (Figure (Figure1). 1 ). There were no other preauricular sinuses in either ear. The ear canals and tympanic membranes of both ears were normal.  Verbal consent was obtained The mother was advised that the appearance of the hole was similar to a preauricular sinus but in a variant location, likely benign, and not associated with any syndromes since his hearing was intact. The mother was also advised that sinus tracts can become infected, so anticipatory guidance was given to monitor for signs of infection, and the patient was referred to a pediatric ENT for further evaluation. ENT’s comprehensive audiology evaluation was unremarkable, showing normal tympanometry, acoustic reflexes, and otoacoustic emissions bilaterally. In addition, a microscopic exam of the ear and the tympanic membrane was normal in the ENT clinic. ENT further reiterated anticipatory guidance for signs of recurrent infection, and an audiology evaluation was recommended on an as-needed basis. Epidemiology Ear pits are a common congenital malformation and can occur either sporadically or hereditarily [ 2 , 4 , 7 ]. The incidence varies globally and is estimated to be 0.1-0.9% in the United States, occurring in 10% of Asian-American, 5% of African-American, and 1% of Caucasian-American children [ 2 - 6 ]. Both sexes are equally affected [ 8 ]. They are unilateral in over 50% of cases, more often on the right ear, and bilateral in 25-50% of cases [ 2 - 7 ]. Presentation Ear pits are small indentations or openings less than 3 mm from the external ear [ 6 ]. They are commonly found incidentally in newborns, but because of their small size and lack of symptoms, they are often missed on routine examinations and cause parental distress because of their cosmetic appearance. Pits have been categorized based on their location in relation to an imaginary tragal vertically extended line into classical types and variant types (Figure (Figure2) 2 ) [ 3 , 7 , 9 ]. The classical type is usually located anterior to the helix and superior to the tragus (preauricular) [ 6 ]. The variant type is uncommon and usually located post-auricularly, either in the middle of the crus (type 1), superior to the crus (type 2), or at the cymba concha (type 3) (Figure (Figure2) 2 ) [ 3 , 7 ]. Ear pits that do not conform to the classical or variant types are extremely rare, found in less than ten reported cases [ 6 , 7 , 9 , 10 ].  Classic: anterior to the helix and superior to the tragus. Variant: type I - middle of the crus; type II - superior to the crus; type III - at the cymba concha. Image Credits: Henry Nguyen, DO MS, author. Embryology and histology The embryogenesis of ear pits is not yet known. From the sixth week of gestation, tissue from the first and second branchial clefts develops into six auditory hillocks (known as the hillocks of His; three from the caudal edge of the first branchial cleft and three from the cephalic edge of the second branchial cleft), which unite to form the external ear within the next few weeks of embryogenesis (Figure (Figure3) 3 ) [ 2 - 9 , 11 - 15 ]. Currently, there are three theories for the development of ear pits: incomplete fusion of the first three auditory hillocks from the first branchial cleft, isolation of ectodermal folds during auricle formation, and defective closure of the most dorsal part of the first branchial cleft [ 2 - 9 , 12 , 14 , 15 ].  (1) Tragus, (2) Helix Crus, (3) Helix, (4) Antihelix, (5) Antitragus, (6) Lobule and Inferior Helix. The inner surface of ear pits consists of stratified squamous epithelium [ 3 , 13 ]. Ear pits can be filled with smegma-like material and can contain sebaceous glands, sweat glands, and hair follicles [ 6 ]. Clinical significance Ear pits are usually isolated and asymptomatic. However, pits can be superficial or have tracts that can vary in length, branch, and follow a tortuous course [ 4 - 10 ]. This can result in the formation of a cyst that can get infected or an abscess. The most common infectious pathogens are Staphylococcal species, followed by Proteus, Streptococcus, and Peptococcus species [ 4 - 6 , 9 ]. In addition, these tracts can extend to the facial nerve and parotid gland, potentially causing facial nerve damage/paralysis and parotitis [ 6 ]. Ear pits can appear concurrently with some congenital anomalies and syndromes associated with hearing impairment, occurring in as many as 15-30% of cases [ 2 ]. In one cross-sectional study of 68,484 infants, hearing impairment was found to be seven times more common among infants with isolated ear pits compared to infants without ear pits [ 12 ]. Even though hearing impairment is due to an inner ear malformation, which originates from different embryonic tissue than the external ear, multiple ear malformations may be possible due to the proximity of the different tissues and because the inner and external ear develop at the same time of embryogenesis [ 12 ]. About 2.6% of patients with ear pits are also associated with some syndromes with renal anomalies [ 2 , 11 ]. Although the incidence of kidney anomalies in patients with isolated ear pits is similar to that of the general population, they may be the first indication of BOR syndrome. It is characterized by hearing loss (70-93% of affected patients; one of the most common causes; approximately 2% of all childhood hearing loss), ear pits, branchial cysts or tracts, malformed ears, and kidney anomalies [ 16 , 17 ]. Ear pits and kidney anomalies can occur in several other syndromes, including CHARGE syndrome, Townes-Brocks syndrome, Nager syndrome, Miller syndrome, the oculo-auriculo-vertebral spectrum, and diabetic embryopathy, to name a few [ 18 ]. Patients with ear pits should have a formal audiologic evaluation. The risk of permanent hearing loss in these patients is five times that of the general population [ 2 , 6 , 12 ]. Routine renal ultrasound for patients with isolated ear pits is up for debate. A study involving 17,286 healthy newborns with isolated preauricular tags and pits did not find a significant association with urinary tract abnormalities, with those found being mostly common congenital anomalies such as mild pyelectasis or hydronephrosis [ 18 ]. However, due to the high incidence of renal anomalies in syndromes with auricular malformations, renal ultrasound should be obtained in children with ear pits accompanied by any of the following [ 2 , 6 , 18 ]: (1) other malformations or dysmorphic features; (2) family history of deafness or auricular or kidney malformations; (3) maternal history of gestational diabetes. Ear pits generally do not require intervention. However, patients require appropriate antibiotics when infected, incision and drainage if an abscess is present, and surgery for recurrent or persistent infections [ 4 , 5 , 8 - 10 , 14 ]. In one study, about 75% of subjects up to a median age of 19 years remained asymptomatic, and 28% of symptomatic patients experienced symptoms after age 16 [ 2 ]. Surgery includes methylene blue staining and probing to assess the extent of the tract course, followed by excision of the pit, its tract/cyst, and the cartilage at the root of the helix en bloc to avoid recurrence [ 4 - 6 , 14 , 15 ]. Recurrence typically occurs due to incomplete resection of sinus tracts due to potential branching between 19% and 40% [ 4 , 5 , 14 , 15 ]. Details of the different surgical methods are excluded from the discussion of this case report. ConclusionsEar pits are incidentally found as congenital abnormalities that are typically asymptomatic and require no intervention. Most pits are classically located anterior to the helix and superior to the tragus, but in rare cases, they are located elsewhere on or around the ear. Our patient’s ear pit would be categorized as a type 3 variant pit. Pits are associated with hearing loss and renal anomalies, as seen in various genetic syndromes, but there have been no studies that determine the prevalence of variant types or if they have a greater association compared to classical locations. These questions warrant further study. Regardless of location, patients with ear pits should have a formal audiologic evaluation. Given the high incidence of renal anomalies in syndromes with auricular malformations, renal ultrasound should also be considered for patients with ear pits and urinary symptoms or increased risk of kidney dysfunction, along with (1) other malformations or dysmorphic features, (2) family history of deafness, auricular, or kidney malformations, or (3) maternal history of gestational diabetes. Infected ear pits should be treated with antibiotics. Abscesses should be drained. Surgical exploration and complete excision of the sinus tract are the treatments of choice for recurrent and complex infections. The authors have declared that no competing interests exist. Human EthicsConsent was obtained or waived by all participants in this study Watch CBS News Trump and Biden's first presidential debate of 2024, fact checkedBy Arden Farhi , Hunter Woodall , Jui Sarwate , Julia Ingram , Layla Ferris , Laura Doan , James LaPorta , Daniel Klaidman , Alexander Tin , Pete Villasmil, Sierra Sanders Updated on: June 28, 2024 / 9:46 AM EDT / CBS News Here's the fact check of some of the statements made by President Biden and former President Donald Trump during the first 2024 presidential debate , which took place in Atlanta on Thursday, June 27. The two tangled on topics including immigration, the economy, abortion and their respective records. Mr. Biden seemed to ramble during many of his responses. CBS News covered the debate live as it happened . Trump claims "we had the greatest economy in the history of our country": FalseTrump : "We had the greatest economy in the history of our country. And we have never done so well. Every- everybody was amazed by it. Other countries were copying us." Details : Trump's claim is false that during his presidency the U.S. had the greatest economy in the history of the country by many of the common metrics used to judge economic performance. The claim struggles when looking at GDP. If the 2020 pandemic is excluded, growth after inflation under Trump averaged 2.49%, according to figures from the World Bank . This is far from the GDP growth under Democratic President Bill Clinton of 3.88%, according to World Bank data . Including the time period after COVID spread, that average drops to 1.18%. Trump's claim also falls short when compared to historical figures. Growth between 1962 to 1966 ranged from 4.4% to 6.6%. In 1950 and 1951, GDP ranged between 8.7% and 8%. Under Mr. Biden, annual GDP growth is averaging 3.4%, according to the Associated Press . *An earlier version of this fact check misstated World Bank figures for growth after inflation under Trump at 2.65%, rather than 2.49%, and 1.45%, instead of 1.18%, and also rounded the growth number for Clinton. This has been updated. Unemployment Trump's claim is also false even when evaluating the unemployment rate. In February 2020, a month before the COVID pandemic affected the economy, the unemployment rate stood at 3.5% — which was the lowest since December 1969 — but not the lowest ever. When Trump's term ended, the unemployment rate was 6.3%. In 1953, the unemployment rate fell as low as 2.5%. Under Mr. Biden, the unemployment rate is 4%, according to the most recent data from May 2024. In January 2023 and again in April 2023, the unemployment rate was 3.4%, lower than the best month during Trump's term. Stock market performance On Jan. 19, 2021, the S&P 500-stock average closed at 67.8% above where it had been the day before Trump was inaugurated in 2017. According to Investopedia , at the end of President Barack Obama's first term in office, the S&P closed 84.5% higher. Additionally the S&P gained 79% during President Bill Clinton's first term, and 70% during President Dwight Eisenhower's first term. So far, under President Biden, the S&P 500 has increased almost 40% , according to calculations on June 13. By Laura Doan and Hunter Woodall Biden claims he's the only president this century that doesn't have troops dying anywhere in the world: FalseBiden: "I'm the only president this century that doesn't have any — this decade — that doesn't have any troops dying anywhere in the world." Details : At least 16 U.S. service members have died while serving overseas during Mr. Biden's presidency. Thirteen U.S. service members died in an attack at the Kabul airport in Afghanistan in August 2021. Three soldiers were killed in an attack in Jordan in January of this year. By Layla Ferris Trump claims he did not refer to U.S. soldiers who were killed as "suckers and losers": FalseTrump: "First of all, that was a made-up quote. 'Suckers and losers,' they made it up." Details : Current and former U.S. military service members have detailed to CBS News multiple instances when Trump made disparaging remarks about members of the U.S. military who were captured or killed, including referring to the American war dead at the Aisle-Marne American Cemetery in France in 2018 as "losers" and "suckers." A senior Defense Department official and a former U.S. Marine Corps officer with direct knowledge of what was said detailed how Trump said he did not want to visit the cemetery because it was "filled with losers." These accounts were backed independently by two other officials — a former senior U.S. Army officer and a separate, former senior U.S. Marine Corps officer. In another conversation on the trip, Trump referred to the 1,800 Marines who died in the World War I battle of Belleau Wood as "suckers" for getting killed. The Atlantic was first to report Trump's comments in 2020. His former chief of staff John Kelly later confirmed to CNN the essence of what Trump had said. By James LaPorta and Sierra Sanders Biden claims 40% fewer people are crossing border illegally, better than when Trump was in office: Partially true Biden: "I've changed it in a way that now you're in a situation where there 40% fewer people coming across the border illegally; it's better than when he left office." Details : Since Mr. Biden issued a proclamation banning most migrants from asylum at the U.S.-Mexico border in early June, illegal crossings there have dropped. In the past week, daily illegal border crossings have averaged roughly 2,000, according to internal Department of Homeland Security data obtained by CBS News. That's a 47% drop from the 3,800 daily average in May. During the height of a spike in migration faced by the Trump administration in 2019, Border Patrol recorded an average of 4,300 daily illegal crossings, government data show. But there were months during the Covid-19 pandemic when the Trump administration averaged fewer than 2,000 illegal border crossings. By Camilo Montoya-Galvez Trump claims migrants coming to U.S. and "killing our citizens at a level...we've never seen before": MisleadingTrump: "People are coming in and killing our citizens at a level like we've never seen before." Details : Some migrants who are believed to have entered the U.S. along the southern border in recent years have been charged with murder and other heinous crimes in different parts of the country. They include the suspect in the high-profile murder of Georgia nursing student Laken Riley . But while the data on this question is not comprehensive, available studies have found that migrants living in the country illegally do not commit crimes at a higher rate than native-born Americans. Government statistics also show a very small fraction of migrants processed by Border Patrol have criminal records in the U.S. or other countries that share information with American officials. On COVID, Trump claims more people died under Biden administration than his: True, but needs context Trump: "Remember, more people died under his administration — even though we had largely fixed it — more people died under his administration than our administration, and we were right in the middle of it, something which a lot of people don't like to talk about. But [Biden] had far more people dying in his administration." Details : More than 460,000 people had died from COVID-19 by the end of the week that Biden was inaugurated in 2021, while more than 725,000 have died in the three years since then, according to data from the CDC . However, research has found that the counts of COVID-19 deaths, especially in the early days of the pandemic, were likely undercounted . By Julia Ingram and Jui Sarwate In discussing abortion, Trump claims former Virginia governor, a Democrat, supported killing babies: FalseTrump: "If you look at the former governor of Virginia, he was willing to do this — he said 'we'll put the baby aside and we'll determine what we'll do with the baby'.. .meaning we'll kill the baby." Details : In a 2019 radio interview then-governor of Virginia Ralph Northam, in discussing late-term abortions, addressed a hypothetical scenario in which a fetus was severely deformed or wasn't otherwise viable. He said, "the infant would be delivered, the infant would be kept comfortable, the infant would be resuscitated if that's what the mother and the family desired." Northam did not say the fetus should be killed. Killing a newborn baby — or infanticide — is illegal in every state, and not a single state is trying to change that. By Laura Doan and Daniel Klaidman Trump claims Biden "went after" his political opponent in New York "hush money" case to damage him: False Trump: "[Biden] basically went after his political opponent (Trump) because he thought it was going to damage me, but when the public found out about these cases, 'cause they understand it better than he does, he has no idea what these cases are, but when they found out about these cases, you know what they did? My poll numbers went up, way up." Details : There is no federal jurisdiction over a state case. The Manhattan district attorney's office is a separate entity from the U.S. Department of Justice. The department does not supervise the work of the Manhattan D.A.'s office, does not approve its charging decisions, and it does not try the D.A.'s cases. By Pete Villasmil Trump claims he brought insulin prices down for seniors: MisleadingTrump: "I'm the one that got the insulin down for the seniors. I took care of the seniors." Details : During Trump's time as president, Medicare created a voluntary program in 2020 between some plans and insulin manufacturers that agreed to cap out-of-pocket costs for insulin at $35 per month. Around half of Medicare Advantage or stand-alone prescription drug plans ended up participating by 2021. David Ricks, CEO of insulin drugmaker Eli Lilly, has taken credit for pioneering the idea with Trump administration officials at a congressional hearing and in an interview . In the same interview with STAT, Seema Verma, former Medicare agency chief in the Trump administration, gave Ricks the credit for the cap: "He is an unsung hero. He was actually the mastermind of all of this." Medicare ended the policy in 2023, after Mr. Biden signed into law the Inflation Reduction Act , which capped insulin costs for Medicare beneficiaries — not just for the portion of plans participating in the program. The law capped insulin costs at the same amount of $35 per month. By Alexander Tin and Hunter Woodall Trump claims Biden wants open borders: FalseTrump: "He wants open borders. He wants our country to either be destroyed or he wants to pick up those people as voters." Details : When he took office, Mr. Biden reversed numerous Trump-era immigration policies, including a program that required migrants to await their asylum hearings in Mexico. U.S. Border Patrol has also reported record numbers of migrant apprehensions along the southern border during Mr. Biden's presidency. But Mr. Biden has never endorsed or implemented an "open borders" policy. In fact, Mr. Biden has embraced some restrictive border policies that mirror rules enacted by his predecessor. In 2023, his administration published a regulation that disqualified migrants from asylum if they crossed into the country illegally after not seeking protection in a third country. Earlier this month, Mr. Biden enacted an even stricter policy: a proclamation that has partially shut down asylum processing along the border. His administration has also carried out over 4 million deportations, expulsions and returns of migrants since 2021, according to government data . Only U.S. citizens can vote in federal elections. Most who cross into the U.S. illegally are not on a path to permanent legal status, let alone citizenship. Even those who apply and win asylum — a process that typically takes years to complete — have to wait five years as permanent U.S. residents before applying for American citizenship. There's no evidence to suggest that the Biden administration's border policy is based on a desire to convert migrants into voters. Biden claims Trump wants to get rid of Social Security: False Biden "[Trump] wants to get rid of Social Security. He thinks there's plenty to cut in social security. He's wanted to cut Social Security and Medicare, both times." Details : Trump has repeatedly said he will try to protect Medicare and Social Security. Trump said in a March 21 Truth Social post that he would not "under any circumstance" allow Social Security to "be even touched" if he were president. Trump had said in a CNBC interview on March 11 that "there is a lot you can do" in terms of "cutting" spending under Social Security. Mr. Biden said the comments were proof Trump aimed to make cuts in the programs, but a Trump campaign spokesman said Trump was referring to "cutting waste and fraud," not Social Security entitlements. Trump claims Biden has the "largest deficit" in history of U.S.: FalseTrump: "But he's (Biden) got the largest deficit in the history of our country." Details : The national deficit was the largest it had been in over two decades under Trump's administration, not Mr. Biden's, according to data from the U.S. Treasury . The deficit peaked in fiscal year 2020 at $3.13 trillion, and declined to $1.7 trillion by the end of fiscal year 2023. By Julia Ingram - Presidential Debate
- Donald Trump
Arden Farhi is the senior White House producer at CBS News. He has covered several presidential campaigns and the Obama, Trump and Biden administrations. He also produces "The Takeout with Major Garrett." More from CBS News Biden debate performance was "tough to watch," Gov. Healey says Pan Mass Challenge rider who had cancer while pregnant looks forward to giving back Senior LGBTQ+-friendly housing complex in Boston opens its doors Celtics majority owner Wyc Grousbeck plans to sell his stake in team- Skip to Main Content
- Skip to audio player to listen live
Enter the username on file and we'll send you a code to reset your password. A verification code has been emailed to With Minnesota law change in effect, adoptees can access original birth records Log in to share your opinion with MPR News and add it to your profile. Thanks for liking this story! We have added it to a list of your favorite stories. Adoptees born in Minnesota will be able to access their birth records starting Monday. Last year, the state passed legislation allowing adopted adults access to those records held by the state. Until now, those records have not been available to adoptees. For the past couple of months, attorney Gregory Luce has been helping to prepare adoptees for the change in the law. While the change in the law is about accessing paperwork, Luce’s work is also about prepping adoptees emotionally for what they might learn by accessing those records. Luce is also an adopted person. He leads the Adoptee Rights Law Center and is the executive director of Adoptees United Inc., a national advocacy organization for adopted people. Support the News you NeedGifts from individuals keep MPR News accessible to all - free of paywalls and barriers.  On a Saturday in early June, Luce stood in front of a small group of people inside Plymouth Congregational Church in Minneapolis, walking them through what birth records they can access. Luce told the audience the law has helped simplify the process for adoptees who choose to apply. “The adopted person applies to the department of health and then within a few weeks, maybe it will take a little bit longer at first, they get the original birth certificate, and they may get some other stuff,” Luce said. “The birth parent can file a contact preference form that is then attached and goes with the records back to the adopted person. It’s simple.” ‘Part of this presentation is to prepare adopted people’ Luce approached the information session by centering on the experiences of adopted people and went step by step through a series of documents adoptees and family members could receive. “Birth records, that’s it,” said Luce. “We’re not talking about court records; you still have to have a court order to obtain those. It also doesn’t include the ‘holy grail’ of records themselves, the adoption agency records, which by far has the most information.” Luce moved on to explain adopted people will receive a non-certified copy of the original birth certificates and any evidence of the adoption filed with the state. Those records will include the names of birth parents. He also mentioned that adoptees might request personal effects from the department of health. “The personal effects could be anything from a letter left to be given to the adoptee or an item or an object.” “I think that’s immensely valuable for all adopted people.” said Luce. “Anyone who is an adoptee knows these personal effects are really valuable and meaningful.” Luce was careful to explain that while adoptees will receive records that include a birth parent’s name, they might also receive copies of legal document a birth parent would have filed previously indicating whether they wanted their name and other identifying information given to the adopted child. In some instances, birth parents may have indicated they didn’t want their information disclosed. “That’s gonna’ be tough for some adoptees — information that your biological parent didn’t want you to have … but I think it's important information for the adopted person to have.” Those older legal forms were invalidated as of June 30. “Part of this presentation is to prepare adopted people,” said Luce. Luce also took care to tell his audience that adoptees might also receive information about whether a birth parent prefers to be contacted. Over the past year, the department of health and human services made contact preference form available to birth parents. Those documents now take effect. - Law change will unseal original birth records for people born in Minnesota and later adopted
- People who were adopted, birth parents react to change in Minnesota birth records policy
Adoptees born in other states also have rights under the new law. Those born in another state but whose adoptions were finalized in Minnesota may request and receive the birth parents’ names and other information from the adoption placing agency. Luce explained that adoptees living in other countries or U.S. states will also have rights under this new law in those instances a birth record was created in Minnesota. Information about application process and fees can be found on the Foster Adopt Minnesota website which includes information about post-adoptee support. - New Hennepin County unit will review past criminal convictions
- Twin Cities celebrity chef Justin Sutherland charged with threatening to shoot girlfriend
- Sen. Nicole Mitchell seeks dismissal of burglary charge while calling for release of more evidence
Fact-checking Biden and Trump's claims at the first debateForget alternative facts and political spin: Thursday's presidential debate was more like a tsunami of falsity. Former President Donald Trump unleashed a torrent of misinformation on topics from terrorism to taxes during the first debate of the 2024 general election, while President Joe Biden flubbed figures and facts about military deaths and insulin prices. More than a dozen NBC News reporters, editors and correspondents fact-checked the key claims the presidential candidates made Thursday night. Here they are by topic: Economy, trade and health careFact check: did biden inherit 9% inflation. “He also said he inherited 9% inflation. Now, he inherited almost no inflation, and it stayed that way for 14 months, and then it blew up under his leadership,” Trump said about Biden. This is false. The inflation rate when Biden took office in January 2021 wasn’t 9%. It was 1.4%. It has risen on his watch, peaking at about 9.1% in June 2022, but by last month it had come down to 3.3%. Pandemic-related stimulus policies put in place by both Trump and Biden were blamed, in part, for the rise in the inflation rate. Fact check: Did Biden lower the cost of insulin to $15 a shot?“We brought down the price of prescription drugs, which is a major issue for many people, to $15 for an insulin shot — as opposed to $400,” Biden said. Biden capped the cost of insulin at $35 a month under Medicare, not $15 a shot, and some drug companies have matched that cap. The price cap doesn’t apply to everyone , however. What’s more, Biden’s also significantly overstating how much insulin cost before the change. A 2022 report by the Department of Health and Human Services found that patients using insulin spent an average of $434 annually on insulin in 2019 — not $400 a shot. Fact check: Did Trump lower the cost of insulin?Trump claimed credit for lowering the cost of insulin for seniors, saying, “I am the one who got the insulin down for the seniors.” That is mostly false. In 2020, Trump created a voluntary program under Medicare Part D. The program allowed Medicare Part D plans to offer some insulin products for no more than $35 per month. It was active from 2021 to 2023, with fewer than half of the plans participating each year. In 2022, Biden signed the Inflation Reduction Act, which included a provision that lowered the out-of-pocket cost for people on Medicare to $35 a month and covered all insulin products. The cap didn’t apply to those with private insurance. However, after the law was implemented, insulin manufacturers voluntarily lowered the out-of-pocket cost to $35 a month for people with private insurance. Fact check: Does Biden want to raise ‘everybody’s taxes’ by four times?“Nobody ever cut taxes like us. He wants to raise your taxes by four times. He wants to raise everybody’s taxes by four times,” Trump claimed. “He wants the Trump tax cuts to expire.” Biden’s tax plan “holds harmless for 98% of households,” said Kyle Pomerleau, senior fellow at the conservative American Enterprise Institute. And Biden wants to extend the majority of the Trump tax cuts, too, though he has advocated for hiking taxes on very high earners. Fact check: Biden said the U.S. trade deficit with China is at its lowest since 2010“We are at the lowest trade deficit with China since 2010,” Biden said. This is true. The U.S. had $279 billion more in imports than exports to China last year, the lowest trade deficit with the world’s second-largest economy since 2010. The highest deficit in recent years was $418 billion, in 2018, when Trump began a trade war with China. The decline has been driven largely by tariffs that Trump imposed in office and that Biden has maintained and in some cases expanded. Fact check: Are immigrants taking ‘Black jobs’?Asked about Black voters who are disappointed with their economic progress, Trump claimed Black Americans are losing their jobs because of illegal border crossings under Biden’s administration. “The fact is that his big kill on the Black people is the millions of people that he’s allowed to come through the border. They’re taking Black jobs now,” Trump said. There’s no evidence that undocumented immigrants are taking jobs away from Black Americans. In fact, according to the Bureau of Labor Statistics , the Black unemployment rate fell to 4.8% in April 2023 — an all-time low. Before that, the Black unemployment rate was as high as 10.2% in April 2021. ImmigrationFact check: did trump end catch and release. “We ended ‘catch and release,’” Trump said. Trump did not end “catch and release,” a term used to describe the practice of releasing migrants into the country with court dates while they await court hearings. The U.S. doesn’t have enough facilities to detain every migrant who crosses the border until they can see judges, no matter who is president, so Trump — like Barack Obama before him and Biden after him — released many migrants back into the U.S. Fact check: Did the Border Patrol union endorse Biden?“By the way, the Border Patrol endorsed me, endorsed my position,” Biden said. The National Border Patrol Council, the labor union for U.S. Border Patrol agents and staff members, has endorsed Trump. “The National Border Patrol Council has proudly endorsed Donald J. Trump for President of the United States,” the group’s vice president, Hector Garza, said in a statement shared exclusively with NBC News. The union posted on X , “to be clear, we never have and never will endorse Biden.” Biden may have been referring to a Senate immigration bill that he backed, which earned the union’s endorsement . Fact check: Did Trump have ‘the safest border in the history of our country’?“We had the safest border in the history of our country,” Trump said. It’s a clear exaggeration. In 2019, the last year before the Covid-19 pandemic brought down border crossings, there were roughly 860,000 illegal border crossings, far more than in any year during the Obama administration. Fact check: Trump says Biden is allowing ‘millions’ of criminals to enter U.S.“I’d love to ask him … why he’s allowed millions of people to come in from prisons, jails and mental institutions to come into our country and destroy our country,” Trump said. There is no evidence of this. Venezuela doesn’t share law enforcement information with U.S. authorities, making it very hard to verify criminal histories of immigrants coming to the U.S. But there’s no evidence that Venezuela is purposefully sending “millions” of people from mental institutions and prisons to the U.S. Fact check: Did Virginia’s former governor support infanticide?“They will take the life of a child in the eighth month, the ninth month and even after birth. After birth. If you look at the former governor of Virginia, he was willing to do so, and we’ll determine what we do with the baby. Meaning we’ll kill the baby. ... So that means he can take the life of the baby in the ninth month and even after birth. Because some states, Democrat-run, take it after birth. Again, the governor, the former Virginia governor, put the baby down so that we decide what to do with it. He’s willing to, as we say, rip the baby out of the womb in the ninth month and kill the baby. Nobody wants that to happen, Democrat or Republican; nobody wants it to happen,” Trump said. While some Democrats support broad access to abortion regardless of gestation age, infanticide is illegal, and no Democrats advocate for it. Just 1% of abortions are performed after 21 weeks’ gestation, according to the Centers for Disease Control and Prevention . Trump first made the claim in 2019, after Virginia’s governor at the time, Ralph Northam, made controversial remarks in discussing an abortion bill. NBC News debunked the claim then, reporting that Northam’s remarks were about resuscitating infants with severe deformities or nonviable pregnancies. Asked on a radio program what happens when a woman who is going into labor desires a third-trimester abortion, Northam noted that such procedures occur only in cases of severe deformities or nonviable pregnancies. He said that in those scenarios, “the infant would be resuscitated if that’s what the mother and the family desired, and then a discussion would ensue between the physicians and the mother.” Terrorism, foreign policy and the militaryFact check: trump said there was ‘no terror’ during his tenure. “That’s why you had no terror, at all, during my administration. This place, the whole world, is blowing up under him,” Trump said. There were two ISIS-inspired terrorist attacks while Trump was president. The first occurred in October 2017, when Sayfullo Saipov killed eight people and injured a dozen more in a vehicle ramming attack on the West Side Highway bike path in New York City. The second occurred in December 2017, when Akayed Ullah injured four people when he set off a bomb strapped to himself. Fact check: Biden suggests no troops died under his watch“The truth is I’m the only president this century that doesn’t have any this decade and any troops dying anywhere in the world like he did,” Biden said. The Defense Department confirmed that 13 U.S. service members were killed in a suicide bombing attack at Abbey Gate at the Kabul airport by a member of ISIS-K as the U.S. was leaving Afghanistan. EnvironmentFact check: did trump have the ‘best environmental numbers ever’. “During my four years, I had the best environmental numbers ever, and my top environmental people gave me that statistic just before I walked on the stage, actually,” Trump said. The figure Trump is referring to is the fact that carbon emissions fell during his administration. He posted the talking points his former Environmental Protection Agency chief emailed him on social media before the debate. And it’s true that carbon emissions are falling — they have been dropping for years. Emissions particularly plunged in 2020, dropping to levels around those in 1983 and 1984. That drop was in large part thanks to Covid lockdowns, and emissions rose again when air travel and in-person working resumed. Still, climate activists and experts are quick to note that those drops are nowhere near enough to head off predicted catastrophic effects of global warming. Other major countries cut their emissions at a much faster rate during the Trump administration. Fact check: The Jan. 6 crowd was not ‘ushered in’ by the police“If you would see my statements that I made on Twitter at the time and also my statement that I made in the Rose Garden, you would say it’s one of the strongest statements you’ve ever seen. In addition to the speech I made in front of, I believe, the largest crowd I’ve ever spoken to, and I will tell you, nobody ever talks about that. They talk about a relatively small number of people that went to the Capitol and, in many cases, were ushered in by the police. And as Nancy Pelosi said, it was her responsibility, not mine. She said that loud and clear,” Trump said. During a lengthy answer to a question about whether he would accept the result of the 2024 election and say all political violence is unacceptable, Trump made several false statements, including the claim that police “ushered” rioters into the U.S. Capitol and that then-House Speaker Nancy Pelosi, D-Calif., said it was her responsibility to keep the chamber safe. Video and news reports of the Jan. 6 riots clearly captured the U.S. Capitol under attack by pro-Trump crowds who overran the law enforcement presence around and inside the complex. On Pelosi, Trump was most likely referring to video shot by Pelosi’s daughter Alexandra for an HBO documentary that showed her during the events of Jan. 6, 2021, tensely wondering how the Capitol was allowed to be stormed. “We have responsibility, Terri,” Pelosi tells her chief of staff, Terri McCullough, as they leave the Capitol in a vehicle. “We did not have any accountability for what was going on there, and we should have. This is ridiculous.” “You’re going to ask me in the middle of the thing, when they’ve already breached the inaugural stuff, ‘Should we call the Capitol Police?’ I mean the National Guard. Why weren’t the National Guard there to begin with?” Pelosi says in the video. “They clearly didn’t know, and I take responsibility for not having them just prepare for more,” she says. Many allies of Trump have tried for the more than three years since the riots to paint Pelosi as somehow being responsible for the violence. Some Trump-backing Republicans have, for example, falsely claimed that she blocked the National Guard from going to the Capitol during the riots. And everything else ...Fact check: trump skipped world war i cemetery visit because the soldiers who died were ‘losers’. Biden said that Trump “refused to go to” a World War I cemetery and that “he was standing with his four-star general” who said Trump said, “I don’t want to go in there, because they’re a bunch of losers and suckers.” In 2018, during a trip to France, Trump canceled a visit to an American cemetery near Paris, blaming weather for the decision. But in September 2020, The Atlantic reported that Trump had axed the visit because he felt that those who’d lost their lives and been buried there were “losers.” The magazine cited “four people with firsthand knowledge of those discussions.” According to The Atlantic, Trump said: “Why should I go to that cemetery? It’s filled with losers.” In another conversation, The Atlantic reported, Trump said the 1,800 American Marines who died were “suckers.” Several media outlets confirmed the remarks, and Trump’s former White House chief of staff John Kelly also said those specific comments were true. Fact check: Trump says Biden didn’t run for president due to 2017 Charlottesville rally“He made up the Charlottesville story, and you’ll see it’s debunked all over the place. Every anchor has — every reasonable anchor has debunked it, and just the other day it came out where it was fully debunked. It’s a nonsense story. He knows that, and he didn’t run because of Charlottesville. He used that as an excuse to run,” Trump said about Biden. The “Unite the Right” rally in Charlottesville, Virginia, in 2017 featured torch-bearing white supremacists marching to protest the removal of a Robert E. Lee statue and chanting racist slogans like “You will not replace us.” It turned deadly when a car plowed into a crowd . In recent months, Trump has downplayed the violence, saying it was “nothing” compared to recent pro-Palestinian protests on university campuses. Meanwhile, Biden has always pointed to Trump’s 2017 comments as the primary reason he decided to seek the presidency in 2020, including in his campaign announcement video back in April 2019 .  Jane C. Timm is a senior reporter for NBC News.  Julia Ainsley is the homeland security correspondent for NBC News and covers the Department of Homeland Security for the NBC News Investigative Unit.  Adam Edelman is a political reporter for NBC News.  Tom Winter is a New York-based correspondent covering crime, courts, terrorism and financial fraud on the East Coast for the NBC News Investigative Unit. | 


























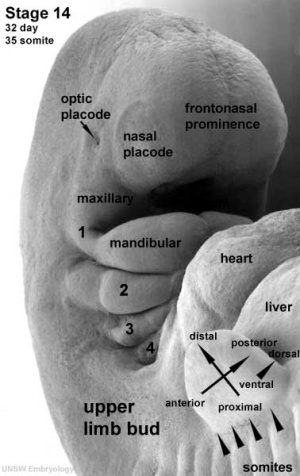




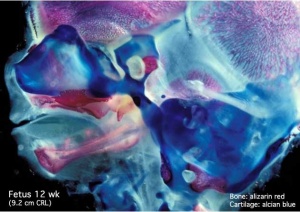
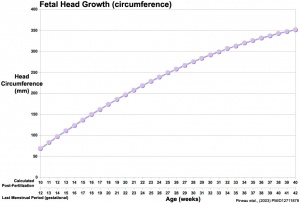





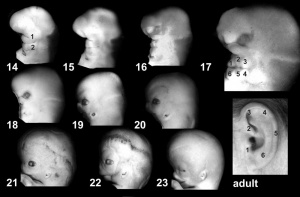



IMAGES
VIDEO
COMMENTS
Presentation refers to the part of the fetus's body that leads the way out through the birth canal (called the presenting part). Usually, the head leads the way, but sometimes the buttocks (breech presentation), shoulder, or face leads the way. Position refers to whether the fetus is facing backward (occiput anterior) or forward (occiput ...
The term presentation describes the leading part of the fetus or the anatomical structure closest to the maternal pelvic inlet during labor. The presentation can roughly be divided into the following classifications: cephalic, breech, shoulder, and compound. Cephalic presentation is the most common and can be further subclassified as vertex, sinciput, brow, face, and chin. The most common ...
Frank breech. When a baby's feet or buttocks are in place to come out first during birth, it's called a breech presentation. This happens in about 3% to 4% of babies close to the time of birth. The baby shown below is in a frank breech presentation. That's when the knees aren't bent, and the feet are close to the baby's head.
This is called cephalic presentation. This position makes it easier and safer for your baby to pass through the birth canal. Cephalic presentation occurs in about 97% of deliveries. There are different types of cephalic presentation, which depend on the position of the baby's limbs and head (fetal attitude).
Fetal presentation, or how your baby is situated in your womb at birth, is determined by the body part that's positioned to come out first, and it can affect the way you deliver. At the time of delivery, 97 percent of babies are head-down (cephalic presentation). But there are several other possibilities, including feet or bottom first (breech ...
Here's your guide to the different positions, or fetal presentations, your baby might be in before birth. Why Does My Baby's Position Matter? Vaginal births can become complicated quickly—and the odds of complication are much higher if your little one isn't in an ideal position, or presentation, for delivery.
Toward the end of pregnancy, the fetus moves into position for delivery. Normally, the presentation is vertex (head first), and the position is occiput anterior (facing toward the pregnant patient's spine) with the face and body angled to one side and the neck flexed. Abnormal presentations include face, brow, breech, and shoulder. Occiput ...
The ear is an incredible organ of hearing and equilibrium divided into three anatomic parts: the external, middle, and internal ear. The external ear, or outer ear, consists of the auricle or pinna, and the tubular external auditory canal ending at the tympanic cavity. The external ear resonates and amplifies sound, and it directs sound towards the tympanic membrane. The middle ear's tympanic ...
Presentation refers to which part of your baby's body is facing towards your birth canal. Position refers to the direction your baby's head or back is facing. Your baby's presentation will be checked at around 36 weeks of pregnancy. Your baby's position is most important during labour and birth.
Delivery presentations. Delivery presentation describes the way the baby is positioned to come down the birth canal for delivery. Your baby must pass through your pelvic bones to reach the vaginal opening. The ease at which this passage will take place depends on how your baby is positioned during delivery. The best position for the baby to be ...
Matsuo and colleagues (3) reported that the frequency of lop ear was 38.1% at birth and 6.1% at 1 year of age. ... Transverse creases may be present in Beckwith Wiedemann syndrome (Figure 37 c) while a complete cleft is a rare presentation (Figure 51 a,b). Classification.
Lecture Objectives. To introduce the developmental embryology of both the face and ear, and their associated abnormalities. To understand the formation and contribution of the pharyngeal arches to face and neck development. To know the main structures derived from components of the pharyngeal arches (groove, pouch and arch connective tissue).
Ears are considered low-set when the helix of the ear meets the cranium at a level below that of a horizontal plane through both inner canthi . Low-set ears are often a sign of a genetic condition ...
Otitis media is an infection of the middle ear. Most of the time, it is caused by bacteria that nearly all children have in their nose and throat at one time or another. Ear infections most often develop after a viral respiratory tract infection, such as a cold or the flu. These infections can cause swelling of the mucous membranes of the nose ...
Congenital malformations of the external ear are uncommon birth defects with long-term sequelae for children and their families. The impact of such deformities on the patient can be both physical and emotional. Parents often experience feelings of guilt because they believe they have caused the deformity. School-aged children may be the object ...
History. In assessing prematurity, gestational age dating by using the mother's history can be unreliable because of uncertainty of the dates. About 20% of women have an uncertain last menstrual period (LMP). Gestational age assessment begins prenatally with obstetric ultrasonography in the first trimester. Discovery of many fetal anomalies ...
Normal ear and its evaluation. The mammalian ear can be divided into three main parts: the outer ear, middle ear, and inner ear, all of which are required for effective hearing. Author: Ian Suchet 1 , Janelle Santos 2. 1. Ian Suchet MBBCh FRCPC, Calgary MFM Centre, EFW Radiology, Calgary, Alberta Canada.
Embryology. Ear Presentation. Development of the ear begins during the first few weeks of pregnancy. At this time the developing fetus looks like a FISH with gills. As the shape of the auricle forms, the developing ear moves (migrates) from under the chin to its proper position on the skull. These two patients have auricles that failed to ...
Presentation. Most parents, while emotionally distressed when their baby is born with a portion of the external auricle missing or severely distorted, are unconcerned about protruding ears at birth. Patients tend to seek surgical opinion for protruding ear problems at two stages of life. Parents often seek medical advice for their children at ...
The causes of ear deformities are varied. Most ear deformities are congenital, meaning they are present from birth. In rare cases, children develop ear deformities from trauma or disease. In some children, an ear deformity is a symptom of a genetic disorder that can affect multiple body systems, such as Goldenhar syndrome and CHARGE syndrome.
Pediatric Auditory Milestones: From 1 to 2 years. Hearing and auditory skills. Talking skills. Firstly, your child can point to a few body parts when asked to. Consequently, the child can now use a variety of new words. Secondly, your child can now follow commands such as "pick up the ball" or "Kiss the teddy.".
Presentation. Ear pits are small indentations or openings less than 3 mm from the external ear . They are commonly found incidentally in newborns, but because of their small size and lack of symptoms, they are often missed on routine examinations and cause parental distress because of their cosmetic appearance.
President Joe Biden and former President Donald Trump faced off during CNN's presidential debate in Atlanta Thursday night.
Trump claims he did not refer to U.S. soldiers who were killed as "suckers and losers": False. Trump: "First of all, that was a made-up quote. 'Suckers and losers,' they made it up."
Thousands of birth records become available to adopted people on Monday. Adopted people 18 years and older can apply to the Minnesota Department of Health to receive their birth records and ...
Trump made a series of misleading claims on topics ranging from Jan. 6 to terrorism to taxes at the first 2024 presidential debate, while Biden flubbed some facts.
Joe Biden and Jill Biden both praised Biden's performance at the CNN Presidential Debate against former President Donald Trump. Some Democrats criticized Biden's performance and are ...
President Biden delivered an energetic North Carolina rally, and a campaign official said there were no plans to replace him on the ticket. Former President Donald J. Trump, in Virginia, called ...